Perrigo Company plc

Perrigo Company plc is a large Irish manufacturer of private label over-the-counter pharmaceuticals.[2] The company’s shares are traded on the NYSE and the Tel Aviv Stock Exchange; as a result of the merger with Agis Industries the company is a constituent of the TA-25 Index. Perrigo is the only non-Israeli company on the TA-25.
Perrigo Company plc, through its wholly owned subsidiaries, engages in the manufacture and sale of consumer healthcare products, generic prescription drugs, active pharmaceutical ingredients (API), and consumer products primarily in the United States, Australia,Israel, Europe, India and Mexico.

| Type |
Public |
| Traded as |
NYSE: PRGO
TASE: PRGO
S&P 500 Component |
| Industry |
Pharmaceutical |
| Founded |
1887 |
| Headquarters |
Allegan, Michigan, USA |
| Key people |
Joseph C. Papa, Chairman, President and CEO |
| Products |
OTC, RX, API, Medical Diagnostic, pharmaceuticals |
| Revenue |
 $3,540 million (2013)[1] $3,540 million (2013)[1] |
| Operating income |
$805 million(2013) |
| Net income |
$ 530 million (2013) |
| Employees |
7,250 (2009) |
| Website |
www.perrigo.com |
Address:
515 Eastern Avenue
Allegan, Michigan 49010-9070
U.S.A.
Telephone: (269) 673-8451
Toll Free: 800-253-3606
Fax: (269) 673-7535
Website: www.perrigo.com
Public Company
Incorporated: 1892
Employees: 3,983
Sales: $826.0 million (2003)
Stock Exchanges: NASDAQ
Ticker Symbol: PRGO
NAIC: 325412 Pharmaceutical Preparation Manufacturing; 325413 In-Vitro Diagnostic Substance Manufacturing
History

Black and white photo of L.Perrigo Co. Aspirin tablets
The L. Perrigo Company was founded in 1887 in Allegan, Michigan, by Luther and Charles Perrigo, who ran a country general store .[3] In 1991 Perrigo had an Initial public offering onNASDAQ.
In March 2005 the firm acquired Agis Industries Ltd. (TASE:AGIS), an Israel based generic pharmaceuticals company in an $850 million transaction. Agis was founded in 1983 by Moshe (Mori) Arkin
 MOSHE ARKIN
MOSHE ARKIN
who developed his father’s small drug import business into a multinational generic pharmaceutical company. As a result of the acquisition Arkin owns 9% of Perrigo, and was appointed as Vice Chairman of the company.[4]
Acquisitions
On 9 January 2008, the firm acquired Galpharm Healthcare, Ltd., a supplier of over-the-counterstore brand pharmaceuticals in the United Kingdom.[5] On 16 September 2008, the firm acquired J.B. Laboratories.[6] On 6 October 2008, it acquired Laboratorios Diba S.A., enabling the company to market its products in Mexico.[7]On 13 November 2008, it acquired Unico Holdings, a manufacturer of store brand pediatric electrolytes, enemas and feminine hygiene products for retail consumers in the U.S.[8]
On 1 March 2010, the firm acquired Orion Laboratories Pty, Ltd. a supplier of over-the-counter (OTC) store brand pharmaceutical products in Australia and New Zealand.[9] On 23 March 2010, it acquired PBM Holdings, Inc.,a producer of over-the-counter store brand infant formula and baby foods in the United States, Canada, Mexico and China.[10]

Perrigo Company is the largest manufacturer of over-the-counter (OTC) pharmaceuticals and nutritional products for store brands in the United States. The company estimates that it holds more than 50 percent of the store brand market. Perrigo produces more than 30 billion pills per year and manufactures about 1,200 products. Most of these are pharmaceuticals–such as analgesics, cough and cold remedies, and gastrointestinal and feminine hygiene products–which account for about four-fifths of the company’s sales. Perrigo ranks as the largest producer of aspirin in the United States. The remaining 20 percent of revenues come from the sale of nutritional products, including vitamins and nutritional supplements and drinks. Perrigo supplies 300 different retailers with these products under the retailer’s own label so that they can be promoted as house brands. These customers include major drugstore chains (CVS, Eckerd, Walgreens), grocery chains (Albertson’s, Kroger, Safeway), mass discounters (Kmart, Target, Wal-Mart), and major wholesalers (McKesson, Supervalu). Perhaps not surprisingly, the largest Perrigo customer by far is retailing giant Wal-Mart, which accounted for 27 percent of net sales for fiscal 2003. The company also markets certain products under its own brand name, Good Sense, although such products account for only a small percentage of sales. Two non-U.S. subsidiaries generate a little more than 9 percent of revenues. Wrafton Laboratories Ltd. supplies store brand products to major grocery and drug retailers in the United Kingdom, while the Mexican firm Química y Farmacia, S.A. de C.V. produces mainly OTC and prescription pharmaceuticals for retail, wholesale, and government customers. Perrigo Company operates 11 manufacturing plants in Michigan, South Carolina, Mexico, and the United Kingdom. Perrigo has enjoyed nearly continuous growth since the end of World War II. This growth can be partly attributed to the mass acceptance of generic and store brand pharmaceutical products.
Early Years
The company was founded by Luther and Charles Perrigo in 1887. The Perrigo brothers had moved to Allegan County, Michigan, a few years earlier from New York. Once in Michigan the brothers established a modest business. Luther Perrigo ran a country general store and apple drying business, while Charles helped with sales. Luther decided to package generic home remedies and sell them to other small country stores like his own. The first packaging plant for these medicines was run out of Charles Perrigo’s home, but Charles soon moved to Ohio, leaving the business entirely to his brother. Luther became president of the firm when it incorporated in 1892. Perrigo remained a family-owned business for 90 years. Five of the company’s seven presidents were descendants of Luther Perrigo, who died in 1902. His son Harry became president at that time, holding the position for the next 49 years.
During the 1920s the company turned to the private label concept in order to build customer loyalty. Stores ordering a certain minimum number could have their own names imprinted on the labels. Products of the era that were the subject of such deals included aspirin, bay rum, epsom salts, sweet oil, and zinc oxide. In the mid-1930s Perrigo gained its first major private label customer, the K & W group, a buying organization that evolved into the People’s Drug Store chain. The second such customer was Sam’s, a major Detroit area drug chain. At the same time the company’s customer base was shifting from small general stores to large regional and national drug chains.
Post-World War II Shift from Packager to Manufacturer
Harry Perrigo turned over the reins to his brother Ray in 1951. It was in the 1950s that the company, while still under the leadership of Ray Perrigo and future President William L. Tripp, Sr., made a crucial decision. Perrigo shifted its focus from that of a repackager of generic drugs to a manufacturer of quality drugs and beauty aids.
William L. Tripp, one of Luther Perrigo’s grandchildren, became president in 1967. During Tripp’s tenure as president the company began to reap the rewards of the change from repackager to manufacturer. The company’s income and the number of Perrigo employees quadrupled. When Tripp died in 1969 his son Bill Tripp, Jr., took over the presidency. During the 1970s Perrigo’s base of customers expanded with the addition of grocery chains and mass merchandisers to the core drugstore chains. By the time of his death in a boating accident in 1980 at the age of 45, Perrigo was the leading private label manufacturer of health and beauty products in the United States. William C. Swaney had been named president of the company two years before the accident, becoming the first leader of the company who was not a member of the Perrigo family.
End of Family Ownership: Early 1980s
Swaney’s presidency lasted from 1978 until 1983. In those five years Perrigo sales tripled and the company became a much larger operation all around. Swaney acquired new companies, set up distribution centers in three states, and expanded and refurbished existing plants. Before leaving as president Swaney oversaw the sale of the company from the Perrigo family to the management. After almost 100 years of family operation the company was sold.
Michael Jandernoa, who had joined the company in 1979 as vice-president for finance, became the seventh president of Perrigo in 1984, while Swaney took over as chairman of the board and CEO. Swaney instituted a style of management at Perrigo that his successor Jandernoa admitted he probably would have tried to block had he been in a position to do so at the time. Yet Jandernoa came to appreciate the open style of administration that Swaney initiated. The company contended that the different disciplines interacted in the decision-making process much more than in traditional American businesses.
Part of the Grow Group, 1986-88
Jandernoa continued the policy of expansion started by Swaney. Perrigo acquired Bell Pharmacal Labs of South Carolina in 1984. Early in the Jandernoa presidency, however, the board of directors began entertaining offers from larger companies that might want to acquire Perrigo itself. In 1986 Perrigo became the largest single company in Grow Group, Inc., a publicly held group of 23 manufacturing companies that bought Perrigo for $45 million. Jandernoa was named CEO of Perrigo; he continued to serve as president. Perrigo represented about a third of Grow Group. As the largest component in a conglomerate with access to funds through the New York Stock Exchange, Perrigo was able to raise new funds for more expansion.
Perrigo celebrated the company’s centenary with two ambitious building projects. It built a $1.5 million plant for the manufacture of effervescent tablets and a $3.5 million graphics art complex to house all of the company’s printing needs. Because Perrigo supplied many different retailers with the same house brand product, their printing facilities were an important part of their production system. The graphics and printing department employed about 290 people and produced almost 70 percent of the company’s labels and 44 percent of their cartons in the early 1990s. The construction of the graphics department, coupled with other expenses, totaled approximately $12.6 million in outlays to the company’s printing and graphics department since the Grow purchase in 1986.
Back to Management Ownership and Then Taken Public: Late 1980s to Early 1990s
After only two years as a part of Grow Group, however, Perrigo was sold back to its management in 1988 in a $106 million deal. That year the company posted sales of $146 million, but by 1994 company sales had ballooned to $669 million. Three years after the sale by Grow to Perrigo management, Jandernoa took the company public. The stock proved popular, though the value fell and rose significantly over time. The market value of the company in July 1994 based on a closing price of $14 a share was $1 billion, for instance. But this price was down from a value of $32 a share in January 1994.
The drop in the value of Perrigo shares was attributed to a drop in sales growth. The company, in fact, had another year of record sales and continued to expand, but stock speculators felt that the market had overreacted to the Perrigo stock offering and had inflated the value beyond its true market worth. Some analysts predicted that the drop in growth was a sign that the national brands would win back bargain-hunting customers in a healthy economy.
Other problems that Perrigo faced in its competition with national brands in the early 1990s concerned finding the right price range for its products. While Perrigo had long wielded its ability to offer lower prices than national brand competitors, sometimes the price difference could be so dramatic–more than 50 percent in some cases–that it could have a reverse effect on the consumer. The consumer weighed the relative cost savings with a judgment on efficacy equivalence. If the price difference was too dramatic, some observers contended, the consumer became suspicious of the Perrigo brand and turned to the national brand. Perrigo therefore developed a system whereby some of the money that it saved from advertising was spent on market research to determine exactly how its products were accepted by the consumer, which products were worth developing, and which had limited potential because of brand allegiance.
One reason for Perrigo’s enormous dominance over the store brand market was its ability to work closely with retailers to promote consumer allegiance to store brands. Beginning in the 1980s Perrigo began a major campaign to help retailers design labels, manage inventory, and develop promotions. Perrigo used its house printing and graphics department to ensure accuracy and reliability in labeling and packaging, permitting rapid new product introductions. Perrigo also enjoyed an advantage over many of its competitors because retail stores had a real incentive to give Perrigo’s product prominence on their shelves. Profit margins for store brand products were considerably greater than for national brands. The store’s public image could be enhanced as well, provided the product sold under their name was satisfactory.
Most of Perrigo’s products were packaged to be readily identifiable with the national brand equivalents. There was a fine line between taking advantage of the competitor’s advertising and carving out a niche that was independently recognized by the consumer. The OTC Market Report disclosed in 1995 that the company was threatened with lawsuits “once or twice a year,” but the vast majority of them were settled in a short period of time. Most of the disputes focused on product dress rather than the actual content of the product. While Perrigo management had become accustomed to lawsuits from competitor companies, in July 1994 Perrigo found itself faced with a lawsuit from closer to home. Its former parent company, Grow Group, filed suit against the company. The Grow Group, valued at less than half of Perrigo, demanded the return of Perrigo stock or a sizable settlement in lieu thereof. Grow claimed that Perrigo management did not act in good faith at the time of the 1988 sale, particularly alleging that they did not reveal a pending agreement to supply products to Wal-Mart, and asked for $2 billion in actual damages and $2 billion in punitive damages. Perrigo contended that the suit was wholly without merit.
One of the company’s strengths was that it faced little legitimate competition. In December 1994 the company purchased Vi-Jon Laboratories, Inc., a leading manufacturer of store brand personal care products, thereby expanding Perrigo’s sales and eliminating a potential competitor at the same time. The purchase price was about $33 million. A similar acquisition occurred earlier, in January 1992, when Cumberland-Swan, Inc., a Tennessee-based maker of store brand personal care products and vitamins, was bought for $35 million.
As the patents on dozens of major prescription drugs began to run out in the mid-1990s, Perrigo began to aggressively go after these lucrative new sources of revenue. Once a prescription drug was reclassified as OTC, the patent holder had two years of exclusivity. At that point generic versions of brand-name OTC products could be produced. An example of this process was Tavist-D, a decongestant and antihistamine that switched from prescription-only to OTC status in 1992. Two years later, Perrigo reached an agreement with the drug’s maker, Sandoz Pharmaceuticals Corp., to begin making a store brand version of Tavist-D in 1995. In subsequent years, Perrigo increasingly turned to such joint ventures to develop new products.
Also in the mid-1990s, Perrigo began looking to the international market for growth, forming subsidiary Perrigo International, Inc. to lead this effort. Among the initially targeted countries were Canada, Japan, Mexico, and Russia.
On 20 January 2011, the firm announced that it would acquire Paddock Laboratories Inc., with the deal expected to close in fiscal 2012.[11]
In September 2012, Perrigo announced its intention to enter the animal wellness category by acquiring the assets of Sergeant’s Pet Care Products, Inc., a privately held manufacturer of over-the-counter companion animal healthcare products. [12]
On 11 February 2013, Perrigo announced the completion of the acquisition of Rosemont Pharmaceuticals Ltd., a specialty and generic prescription pharmaceutical company focused on the manufacturing and marketing of oral liquid formulations. [13]On 29 July 2013, the firm announced that it would acquire Élan, a major drugs firm based in Dublin.[14][15]
Segments
The company operates in three segments; Consumer Healthcare, Rx Pharmaceuticals, and Active Pharmaceutical Ingredients. The Consumer Healthcare segment produces over-the-counter pharmaceutical and nutritional products in the United States, the United Kingdom, and Mexico. This segment offers analgesic, cough/cold/allergy/sinus, gastrointestinal, smoking cessation, first aid, antacids, hemorrhoidal remedies, motion sickness, sleep aid products, feminine hygiene products, vitamin, and nutritional supplementproducts.
The Rx Pharmaceuticals segment produces generic prescription drugs in the United States. This segment provides creams, ointments, lotions, gels, and solutions, as well as nasal sprays, foams, and transdermal devices.
The Active Pharmaceutical Ingredients segment produces pharmaceutical ingredients in Israel with sales to customers worldwide. The company also offers cosmetics, toiletries, detergents, manufactured and imported pharmaceutical products, and medical diagnostic products. The company’s customers include national and regional retail drug, supermarket, wholesalers, and mass merchandise chains.

Management
Joseph C. Papa is the Chief Executive Officer and President.[16]

Joseph C. Papa Jr.
PATENTS
The Perrigo API R&D team has created dozens of ground-breaking, patent-protected industrial processes. These sophisticated, efficient manufacturing procedures facilitate cost-effective production and flexible pricing, helping to strengthen our customers’ long term competitive positions in the marketplace.
| Patents ROW |
| API |
Description |
Patent/Application no. |
| Anastrozole |
Preparation process |
DE 102005037484 |
| Imatinib |
Imatinib process |
IN 216/KOL/2009 |
| Imatinib |
Imatinib alpha form |
DE 102007021043 |
| Moxonidine |
Moxonidine polymorphs |
IL 176556 |
| Moxonidine |
Moxonidine process |
EP 1982983 |
| Moxonidine |
Moxonidine process |
EP 1873151 |
| Moxonidine |
Moxonidine purification |
EP 1873152 |
| Moxonidine |
Moxonidine salts |
EP 1894927 |
| Terbinafine Hydrochloride |
Preparation process |
IL 137364 |
| Theobromine |
Theobromine process |
CN 200710116201.8 |
| Theobromine |
Theobromine purification |
CN 200710116000.8 |
| Theobromine |
Theobromine production process |
WO 2009/089677 |
|
| Patents USA |
| API |
Description |
Patent/Application no. |
| Azacitidine |
Azacitidine crystallization |
US 2011-0288042 |
| Cetirizine Dihydrochloride |
Preparation process |
US 6,100,400 |
| Cilostazol |
Improved process |
US 7,524,960 |
| Cisatracurium |
Cisatracurium acid compounds |
US 2010-0168431 |
| Cisatracurium |
Cisatracurium acid process |
US 2010-0184988 |
| Cisatracurium |
Cisatracurium API from acid |
US 2010-0256381 |
| Cisatracurium |
Cisatracurium by-products |
US 2011-0185796 |
| Cisatracurium |
Cisatracurium flash chromatography |
US 2010-0174082 |
| Cisatracurium |
Cisatracurium normal phase |
US 2010-0099878 |
| Cisatracurium |
Cisatracurium purification |
US 2010-0234602 |
| Cisatracurium |
Cisatracurium reverse phase |
Us 2010-0087650 |
| Donepezil Hydrochloride |
Donepezil hydrochloride compositions |
US 6,734,195 |
| Donepezil Hydrochloride |
Preparation process |
US 6,844,440 |
| Donepezil Hydrochloride |
Purification via Donepezil maleate |
US 7,592,459 |
| Fluticasone Propionate |
Method of isolating a Fluticasone intermediate |
US 6,747,163 |
| Granisetron |
Granisetron intermediate |
US 7,060,841 |
| Halobetasol |
Halobetasol |
US 7,208,485 |
| Imatinib |
Imatinib process |
US 7,507,821 |
| Imatinib |
Imatinib with EDC |
US 7,550,591 |
| Imiquimod |
Imiquimod ammonia DMSO |
US 7,659,398 |
| Imiquimod |
Imiquimod process |
US 7,323,568 |
| Imiquimod |
Imiquimod urea/guanidine |
US 7,943,771 |
| Lamotrigine |
Preparation process |
US 6,329,521 |
| Letrazole |
Letrozole process |
US 7,538,230 |
| Letrazole |
Letrozole purification |
US 7,465,749 |
| Levocetirizine |
Levocetirizine purification |
US 2011-0230496 |
| Midazolam |
Midazolam Maleate process |
US 7,776,852 |
| Montelukast Sodium |
Amorphous montelukast |
US 7,544,805 |
| Montelukast Sodium |
Montelukast precursor |
US 7,572,930 |
| Montelukast Sodium |
Montelukast process |
US 7,528,254 |
| Palonosetron |
Palonosetron salts |
US 2010-0174080 |
| Rocuronium Bromide |
Rocuronium bromide process |
US 7,579,461 |
| Rotigotine |
Rotigotine crystalline base |
US 2010-0222602 |
| Temozolomide |
Improved process |
US 7,612,202 |
| Tramadol Hydrochloride |
Tramadol purification |
US 5,672,755 |
| Tramadol Hydrochloride |
Tramadol separation process |
US 5,874,620 |
| Zonisamide |
Derivatives of BIOS-H |
US 7,745,471 |
|
|
|
|
|
|
Awards
101 Best and Brightest Companies to Work For of West Michigan awarded Perrigo overall “Best of the Best” for 2009.[17]
In 2010 Perrigo was named one of the top 100 Fastest-Growing Companies by Fortune Magazine.[18]

From its beginnings as a packager of generic home remedies in 1887, Perrigo Company plc, headquartered in Ireland, has grown to become a leading global healthcare supplier. Perrigo develops, manufactures and distributes over-the-counter (OTC) and generic prescription (Rx) pharmaceuticals, nutritional products and active pharmaceutical ingredients (API), and receives royalties from Multiple Sclerosis drug Tysabri®. The Company is the world’s largest manufacturer of OTC healthcare products for the store brand market and an industry leader in pharmaceutical technologies. Perrigo’s mission is to offer uncompromised “Quality Affordable Healthcare Products®,” and it does so across a wide variety of product categories primarily in the United States, United Kingdom, Mexico, Israel and Australia, as well as more than 40 other key markets worldwide, including Canada, China and Latin America.
Perrigo API (formerly known as Chemagis) provides differentiated Active Pharmaceutical Ingredients (APIs) and Finished Dosage Forms (FDFs) for the branded and generic pharmaceutical industries.
Founded in 1987 in Israel and led by an accomplished team of industry experts, Perrigo API products comply with the highest regulatory requirements of leading health authorities such as FDA, PMDA, TGA, ANVISA and EU authorities. The company’s facility in Israel is FDA-inspected, cGMP-compliant and recognized for environmental stewardship.
Leveraging our strengths in complex chemistry, innovative patent development and in-depth regulatory expertise, Perrigo API provides tailor-made solutions to meet individual client requirements. We offer our customers comprehensive, customized solutions which include IP assets, API and FDF products, dossiers, bundling and P-IV partnerships, some through joint ventures and some independently, and all strengthened by well-designed and mutually beneficial strategic alliances.
Perrigo API offers comprehensive technical and regulatory support across the entire product lifecycle, from project inception to final production. Our state-of-the-art efficiency and control measures applied across the supply, development and manufacturing chain, allow Perrigo API to provide exceptional value and product differentiation to hundreds of customers worldwide. (Learn more about partnership opportunities)
With the ever-changing and increasingly competitive climate in the global API and Pharma industry, Perrigo API has been proactively searching for ways to continually add customer value and improve our leadership position. In 2009, Perrigo API (PAI) was established, following the acquisition of 85% of the holdings of a state-of-the-art API plant near Mumbai. Fully operational as of 2013, PAI supports Perrigo efforts to increase production capacity and competitiveness, while strictly complying with all industry regulations. This strategic move towards diversified capabilities further enhances Perrigo API highly valued operational flexibility, and adds to our company’s competitive edge.
FDFPerrigo API extends its Active Pharmaceutical Ingredients (APIs) product line with selected Finished Dosage Forms (FDFs) where it is strategically advantageous to customers, providing the most added value and differentiation for clients.Perrigo API focuses on developing those FDFs which require complex and sophisticated manufacturing processes, providing our valuable clients with highly professional regulatory support and reliable supply chain.All Perrigo API products, are made with high standards complying with GMP and regulatory requirements of leading health authorities.Products under patent are not sold until patent expiration in the relevant country.
| FDF |
Therapeutic Use |
More |
| Anastrozole tablets 1 mg |
Treatment of hormone receptor-positive breast cancer in postmenopausal women |
► |
| Cetirizine dihydrochloride 10 mg tablets Cetirizine dihydrochloride 10 mg/ml, oral drops Cetirizine dihydrochloride 1 mg/ml, oral solution |
Symptomatic treatment of allergic rhinitis |
► |
| Granisetron HCl ampoules 1 mg/ml 1ml, 3 ml |
Prevention and treatment of acute nausea and vomiting associated with chemotherapy and radiotherapy |
► |
| Granisetron HCl tablets 1, 2 mg |
Prevention and treatment of acute nausea and vomiting associated with chemotherapy and radiotherapy |
► |
| Letrozole tablets 2.5 mg |
First-line treatment in postmenopausal women with hormone-dependent breast cancer |
► |
| Moxonidine tablets 0.2, 0.3, 0.4 mg |
Mild to moderate essential hypertension |
► |
| Temozolomide hard gelatin capsules 5, 20, 100, 140, 180, 250 mg |
Treatment of patients with malignant glioma such as glioblastoma multiforme or anaplastic astrocytoma |
► |
|
|
|
|
|
Perrigo API specializes in tailor-made research and process development of Active Pharmaceutical Ingredients (APIs) and Finished Dosage Forms (FDFs), with special emphasis on complex, differentiated APIs and FDFs.
Perrigo API carefully selects APIs and FDFs which provide our customers with a competitive market position by delivering unique IP as part of a total solution. All Perrigo API products comply with the exacting regulatory requirements of leading health authorities, including the FDA, PMDA, TGA, ANVISA and other EU authorities.
Below is a list of APIs and FDFs which are currently under development.
Products under patent are not sold until patent expiration in the relevant country.
| API |
Therapeutic Use |
More |
| Esomeprazole Mg Dihydrate Form A |
Gastroesophageal reflux disease (GERD) |
► |
| Fexofenadine Hydrochloride |
Allergy symptoms |
► |
| Fluticasone Furoate |
Seasonal and perennial allergic rhinitis |
► |
| Fulvestrant |
Breast cancer |
► |
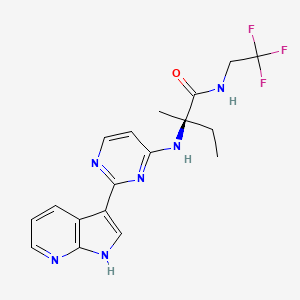
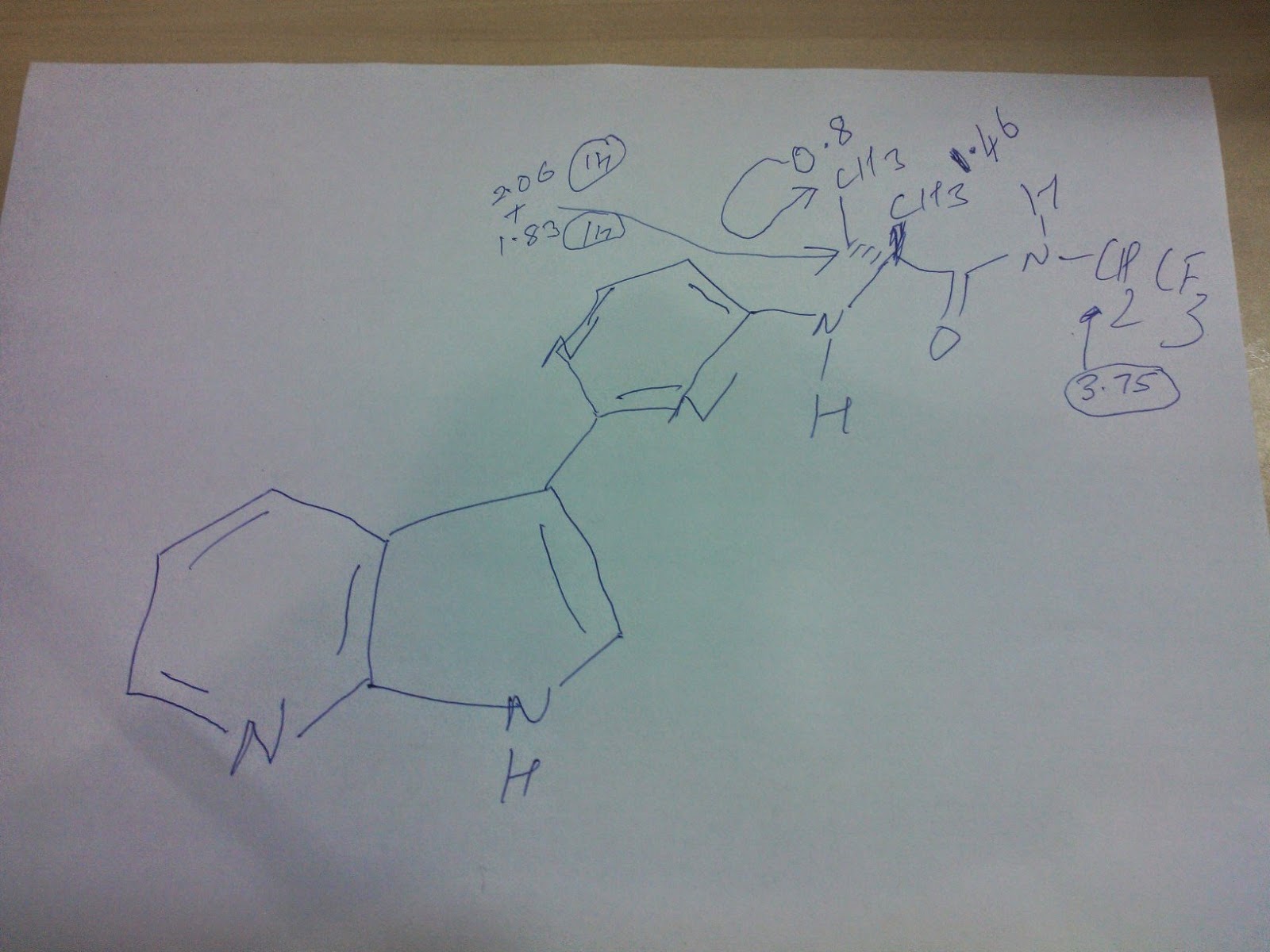
| Ibrutinib |
Leukemia |
► |
| Loratadine |
Seasonal allergic rhinitis; Chronic idiopathic urticaria |
► |
| Montelukast Sodium |
Prophylaxis and chronic treatment of asthma |
► |
| Tiotropium Bromide Monohydrate |
Bronchospasm associated with chronic obstructive pulmonary disease (COPD) |
► |
| Vilanterol Trifenatate |
Bronchospasm associated with chronic obstructive pulmonary disease (COPD) |
► |
| FDF |
Therapeutic Use |
More |
| Azacitidine |
myelodysplastic syndromes and chronic myelomonocytic leukaemia |
► |
| Fulvestrant |
Breast cancer |
► |
|
API
Perrigo API team is deeply committed to achieving uncompromising quality and reliability at every point in the value chain, from product inception to production, from regulatory affairs to go-to-market activities.
Mr. Yoav Grinberg
General Manager
Mr. Grinberg brings extensive general management experience as well as international marketing and sales experience. Previously MR. Grinberg was responsible for Perrigo API sales and marketing activities worldwide. Before joining Perrigo API in 2010, Mr. Grinberg worked for 20 years in the chemical and plastics industries in various senior general management and sales and marketing positions, based in Israel and Europe. Mr. Grinberg holds an MBA from Tel Aviv University.
Dr. Shireesh Ambhaikar
CEO, Perrigo API India Private Limited (PAI)

Dr. Ambhaikar has held numerous positions of increasing responsibility in manufacturing, project management and general management in the pharmaceutical industry. Prior to joining PAI, Dr. Ambhaikar was head of manufacturing, supply chain and global sourcing at UCB Pharm. Prior to that, he was with Sandoz/Novartis, with responsibilities in both manufacturing and project management. Dr. Ambhaikar holds a PhD degree in Organic Chemistry from Mumbai University.
Mr. Ilan Avni
Director Business Development & Pipeline

Mr. Avni joined Perrigo in 2006 and has held several Business Development positions of increasing responsibility both in the US Rx and API business units with experience in acquisitions, divestures, joint ventures, co development and product licensing. In his previous position, Mr. Avni served as an integration project leader for Perrigo API India. Mr. Avni holds an MBA with dual major in Finance and Marketing from Tel Aviv University and a BSc Pharm from the Hebrew University of Jerusalem.
Dr. Tami Greenberg
Head of Quality Perrigo Israel API

As Head of Quality for Perrigo Israel API, Dr. Greenberg is responsible for all QA/QC operations, regulatory compliance and meeting customers’ technical needs. Prior to joining Perrigo API in 2006, Dr. Greenberg was part of the R&D team in Bromine Compounds and lead different development projects. Dr. Greenberg holds Ph.D. in Material engineering from the Ben-Gurion university of the Negev.
Mrs. Dina Hanuna
API Finance Controller
Mrs. Hanuna joined Perrigo Israel (formerly Agis) in 1991. Prior to joining Perrigo, Mrs. Hanuna held the position of Senior Manager with the CPA firm Jungerman, Gilboa & Co. Mrs. Hanuna has more than 20 years of experience in several roles in the Finance Department at Perrigo Israel, nine years of which have been in senior management roles. Mrs. Hanuna is a Certified Public Accountant (Israel). She holds a BA in Economics and Business Administration from Bar Ilan University as well as a BA in Accounting from Tel Aviv University.
SEE…http://investing.businessweek.com/research/stocks/private/person.asp?personId=8971366&privcapId=881270&previousCapId=881270&previousTitle=Perrigo%20Israel%20Pharmaceuticals%20Limited
Mrs. Ayala Kost
VP of Global Operations Perrigo API
As the Perrigo API executive in charge of Operations, Previously Mrs. Kost was responsible for Quality Assurance and control as well as regulatory compliance and meeting customers’ technical needs. Prior to joining Perrigo API in 2002, Mrs. Kost was U.S. Marketing Director and Pilot Lab Manager at, a leading manufacturer of crop protection chemicals. Prior to that she held the position of Process Engineer at Nepro Negev Projects. Mrs. Kost holds an MBA from Tel Aviv University and a BSc in Chemical Engineering from Ben-Gurion University.
Mrs. Dganit Vered
VP, API Research & Development

Mrs. Vered joined Perrigo in 2012 as VP Research and Development. Mrs. Vered is responsible for all Perrigo API R&D activities worldwide. Prior to joining Perrigo she worked at Intel Corporation for more than 17 years and at total of 21 years in the semiconductors business. While with Intel Mrs. Vered held several senior management positions and performed R&D, Engineering, Operations and Facilities, QA/QC and project management roles. Mrs. Vered holds BSc of Chemical engineering from the Technion.
Dr. Alexander Weisman
CSO

Dr. Weisman has more than 25 years of experience in R&D in Analytical and Organic Chemistry, out of which15 years in the pharmaceutical industry including 10 years in management roles. Dr. Weisman joined Perrigo API in 1998, as manager of Analytical R&D and later nominated as VP R&D. In 2012 Alex became the CSO of the company. Dr. Weisman has more than 15 articles and patents to his credit. He holds a PhD in Biochemistry from Moldova State University.
References
External links
Key Dates:
- 1887:
- Luther and Charles Perrigo begin packaging generic home remedies and selling them at their own and to other general stores.
- 1892:
- Company is incorporated.1920s:Perrigo begins offering private label products.1930s:Customer base begins to shift from general stores to large regional and national drug chains.1950s:Company shifts from a repackager of generic drugs to a manufacturer of quality drugs and beauty aids.
1970s:Grocery chains and mass merchandisers are added to the customer base.
- 1980:
- Perrigo is now the nation’s largest private label manufacturer of health and beauty products.Early 1980s:Perrigo family ownership ends with the sale of the company to management.
- 1986:
- Company is sold to Grow Group, Inc. for $45 million.
- 1988:
- Grow Group sells the company back to management for $106 million.
- 1991:
- Perrigo is taken public.
- 1997:
- Controlling stake in Mexican pharmaceutical firm Química y Farmacia, S.A. de C.V. is acquired.
- 1998:
- Perrigo posts a net loss of $51.6 million thanks to a restructuring of its personal care business.
- 1999:
- The personal care business is divested to focus the company on OTC drugs and nutritional products.
- 2001:
- Perrigo acquires Wrafton Laboratories Ltd., a U.K. maker of store brand pharmaceuticals.
Executive Management
Joseph C. Papa
President, Chief Executive Officer and Chairman
 |
Mr. Papa joined the Company in October 2006 as President and Chief Executive Officer. Mr. Papa was elected as a director in November 2006 and, subsequently, was appointed as Chairman of the Board of Directors in October 2007. Previously, Mr. Papa served from December 2004 to October 2006 as Chairman and Chief Executive Officer of the Pharmaceutical and Technologies Services segment of Cardinal Health, Inc. Prior to that position, he served as President and Chief Operating Officer of Watson Pharmaceuticals, Inc. from November 2001 to November 2004. Additionally, Mr. Papa has held management positions at DuPont Pharmaceuticals, Pharmacia Corporation, G.D. Searle & Company and Novartis AG. Mr. Papa is a director of Smith & Nephew, a developer of advanced orthopedic medical devices. |
Judy L. Brown
Executive Vice President and Chief Financial Officer
 |
Ms. Brown was named Executive Vice President and Chief Financial Officer in July 2006. She served as Vice President and Corporate Controller from September 2004 to July 2006. Previously, Ms. Brown held various senior positions in finance and operations at Whirlpool Corporation from 1998 to August 2004. Ms. Brown is a director of Belden Corporation, a NYSE traded company, that designs, manufactures and markets cable, connectivity and networking products in markets including industrial automation, enterprise, transportation, infrastructure and consumer electronics. |
Tom Farrington
Senior Vice President and Chief Information Officer
 |
Mr. Farrington was named Senior Vice President and Chief Information Officer in October 2006. He formerly served as Chief Information Officer for F. Dohmen Co. in addition to serving as a division President for JASCORP LLC from March 2003 to October 2006. Prior to that position, Mr. Farrington held various senior positions in information technology and finance at Dell, Inc. from 1999 to 2003. |
John T. Hendrickson
Executive Vice President, Global Operations and Supply Chain
 |
Mr. Hendrickson was named Executive Vice President, Global Operations and Supply Chain in March 2007. He served as Executive Vice President and General Manager, Perrigo Consumer Healthcare from August 2003 to March 2007. He served as Executive Vice President of Operations from October 1999 to August 2003. |
Scott Jamison
Executive Vice President, General Manager of Nutritionals
 |
Mr. Jamison was named Executive Vice President, General Manager of Nutritionals in January 2011. Before the Company acquired PBM in fiscal 2010, Mr. Jamison had served as PBM’s Executive Vice President and General Counsel since the formation of PBM in 1997 and was a key member of the executive team throughout the evolution and growth of PBM. In addition to his legal responsibilities, Mr. Jamison has held senior leadership responsibilities in operations and sales, as well as in new business and product development. |
Todd W. Kingma
Executive Vice President, General Counsel and Secretary
 |
Mr. Kingma was named Executive Vice President in May 2006. He served as Vice President, General Counsel and Secretary from August 2003 to May 2006. Previously, Mr. Kingma held various positions at Pharmacia Corporation from 1991 through August 2003. His last position with Pharmacia Corporation was Vice President and Associate General Counsel, Global Specialty Operations |
Sharon Kochan
Executive Vice President and General Manager, International
 |
Mr. Kochan was named Executive Vice President and General Manager, International in August 2012. He served as Executive Vice President, General Manager of Rx Pharmaceuticals from March 2007 to August 2012 and as Senior Vice President of Business Development and Strategy from March 2005 to March 2007. Mr. Kochan was Vice President, Business Development of Agis Industries (1983) Ltd. from July 2001 until the acquisition of Agis by the Company in March 2005. |
Jeff Needham
Executive Vice President, General Manager of Consumer Healthcare
 |
Mr. Needham was named Executive Vice President, General Manager of Consumer Healthcare in October 2009. He served as Senior Vice President of Commercial Business Development from March 2005 through October 2009. Previously, he served as Senior Vice President of International from November 2004 to March 2005. He served as Managing Director of Perrigo’s U.K. operations from May 2002 to November 2004 and as Vice President of Marketing from 1993 to 2002. |
Jatin Shah
Senior Vice President and Chief Scientific Officer
 |
Dr. Shah was named Senior Vice President and Chief Scientific Officer in June 2005. He served as Vice President of Research and Development for Rx products from February 2004 to June 2005. Previously, Dr. Shah held various senior positions in Research and Development at Mayne Pharma (known previously as Faulding Pharmaceuticals) from June 1996 to January 2004. |
Mike Stewart
Senior Vice President, Global Human Resources
 |
Mr. Stewart was named Senior Vice President, Global Human Resources in September 2004. He served as Vice President, Human Resources from July 1993 to September 2004. Mr. Stewart began his employment with the Company in August 1981. |
Louis Yu
Executive Vice President, Global Quality and Compliance
 |
Dr. Yu joined the Company in November 2006 as Senior Vice President, Global Quality and Compliance. Previously, Dr. Yu served from October 2005 to October 2006 as Vice President, Quality at CV Therapeutics Inc. Prior to that position, he served as Global Head of Quality & Compliance for Forest Laboratories, Inc. from April 1999 to October 2005. He served as the Vice President, Quality & Compliance for Solvay Pharmaceuticals between October 1996 and March 1999. Currently, he is associated with the University of Wisconsin, serving as Adjunct Professor, Extension Services in Pharmacy, School of Pharmacy. |
Douglas Boothe
Executive Vice President and General Manager, Perrigo Pharmaceuticals
 |
Mr. Boothe joined Perrigo in January 2013 as Executive Vice President and General Manager, Perrigo Pharmaceuticals. Previously, Mr. Boothe served as Chief Executive Officer of Actavis Inc. from August 2008 to December 2013 and as Executive Vice President and Chief Operating Officer from 2006 to 2008. Prior to that position, Mr. Boothe held various senior positions in strategic planning and business development for Alpharma Inc., Pharmacia Corporation and Xerox Corporation. |

 DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO