
Home » Antivirals
Category Archives: Antivirals
 DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HERE
DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HEREFlag and hits
ORGANIC SPECTROSCOPY

SUBSCRIBE

 Subscribe in a reader
Subscribe in a reader
Enter your email address:
Delivered by FeedBurner
Subscribe to New Drug Approvals by Email![]()

![]()



![]()
![]()





Recent Comments
| shivkr2 on SPSR Excellence Award 2025 – S… | |
| Bonkasaurus on Infigratinib phosphate | |
| PALOVAROTENE | ORGAN… on Palovarotene | |
| Pfizer just purchase… on Temanogrel | |
| Pfizer To Cash In On… on Temanogrel |
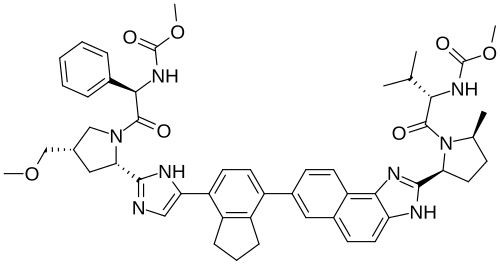
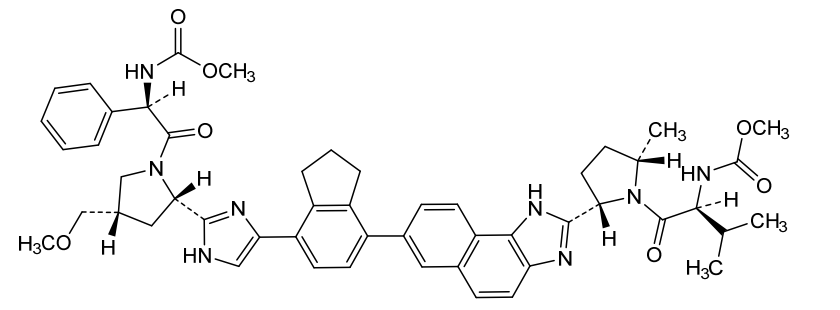
Netanasvir

Netanasvir
CAS 2007900-70-9
MF C51H58N8O7 MW895.1 g/mol
methyl N-[(1R)-2-[(2S,4S)-2-[5-[7-[2-[(2S,5S)-1-[(2S)-2-(methoxycarbonylamino)-3-methylbutanoyl]-5-methylpyrrolidin-2-yl]-3H-benzo[e]benzimidazol-7-yl]-2,3-dihydro-1H-inden-4-yl]-1H-imidazol-2-yl]-4-(methoxymethyl)pyrrolidin-1-yl]-2-oxo-1-phenylethyl]carbamate
- Carbamic acid, N-[(1R)-2-[(2S,4S)-2-[5-[2,3-dihydro-7-[2-[(2S,5S)-1-[(2S)-2-[(methoxycarbonyl)amino]-3-methyl-1-oxobutyl]-5-methyl-2-pyrrolidinyl]-1H-naphth[1,2-d]imidazol-7-yl]-1H-inden-4-yl]-1H-imidazol-2-yl]-4-(methoxymethyl)-1-pyrrolidinyl]-2-oxo-1-phenylethyl]-, methyl ester
- Methyl ((S)-1-((2S,5S)-2-(7-(7-(2-((2S,4S)-1-((R)-2-((methoxycarbonyl)amino)-2-phenylacetyl)-4-(methoxymethyl)pyrrolidin-2-yl)-1H-imidazol-5-yl)-2,3-dihydro-1H-inden-4-yl)-1H-naphtho[1,2-d]imidazol-2-yl)-5-methylpyrrolidin-1-yl)-3-methyl-1-oxobutan-2-yl)carbamate
- methyl {(2S)-1-[(12S,15S,52S,54S,7R)-7-[(methoxycarbonyl)amino]-54-(methoxymethyl)-15-methyl-6-oxo-32,33-dihydro-21H,31H,41H-2(2,7)-naphtho[1,2-d]imidazola-4(4,2)-imidazola-1(2),5(2,1)-dipyrrolidina-3(4,7)-indena-8(1)-benzenaoctaphan-11-yl]-3-methyl-1-oxobutan-2-yl}carbamate
- Methyl N-[(1R)-2-[(2S,4S)-2-[5-[2,3-dihydro-7-[2-[(2S,5S)-1-[(2S)-2-[(methoxycarbonyl)amino]-3-methyl-1-oxobutyl]-5-methyl-2-pyrrolidinyl]-1H-naphth[1,2-d]imidazol-7-yl]-1H-inden-4-yl]-1H-imidazol-2-yl]-4-(methoxymethyl)-1-pyrrolidinyl]-2-oxo-1-phenylethyl]carbamate

antiviral, Dongweizhuo, HCV, Antaitavir Hasophate, HEC 74647 PA, 4Y7YD32BYY
Netanasvir (commonly prescribed as netanasvir phosphate) is a direct-acting antiviral medication primarily used to treat chronic hepatitis C virus (HCV) infection. It was approved by the China National Medical Products Administration (NMPA) under the trade name Dongweizhuo.
Key Clinical Information
- Mechanism of Action: It acts as a potent and selective NS5A inhibitor. By targeting the HCV NS5A protein, it successfully blocks viral RNA replication, virion assembly, and viral clearance mechanisms.
- Combination Therapy: It is exclusively indicated for use in combination with encofosbuvir (an NS5B polymerase inhibitor).
- Target Genotypes: The combination regimen effectively treats adult patients with chronic HCV genotypes 1, 2, 3, or 6.
- Patient Profiles: It is suitable for patients who are either treatment-naïve or have been previously treated with interferon, with or without compensated liver cirrhosis.
- Administration & Elimination: Taken orally, the drug demonstrates high metabolic stability, with feces serving as its primary elimination pathway
- OriginatorSunshine Lake Pharma
- ClassAntivirals
- Mechanism of ActionHepatitis C virus NS 5 protein inhibitors
- RegisteredHepatitis C
- 08 Feb 2025Registered for Hepatitis C (Combination therapy, Treatment-experienced) in China (PO)
- 08 Feb 2025Registered for Hepatitis C (Combination therapy, Treatment-naive) in China (PO)
- 31 Dec 2023NMPA, China accepts NDA for netanasvir for Hepatitis C for review
Netanasvir is an antiviral drug used to treat hepatitis C virus (HCV).[1] In China, netansavir is approved for use in combination with encofosbuvir for the treatment of adult patients with chronic HCV genotypes 1, 2, 3, or 6, who are either treatment-naive or have been previously treated with interferon.[2]
PAT
Compounds as hepatitis c virus inhibitors and pharmaceutical uses thereof
Publication Number: WO-2016141890-A1
Priority Date: 2015-03-12
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2016141890&_cid=P22-MRH62L-18160-1
ADVERTISEMENT
ANAX LABORATORIES
WEBSITE https://www.anaxlab.com/
Discovery Solutions, Supporting the chemistry needs of clients in the Medical, Analytical and Bio Sciences
Development Solutions, Developing from Lab scale to PR&D, Kilo Scale-ups and Commercial Scales
SEE MORE………Integrated Solutions, Manufacturing Solutions, Products,
Can’t Find? Let’s Connect

Phone : +91 897704 2010 / +91 9177075735, Email : info@anaxlab.com
#MedicinalChemistry, #DrugDiscovery, #OrganicSynthesis, #ChemicalLibrary, #BuildingBlocks, #SARStudies, #ChemistryInnovation, #medchem, #Drugdevelopment, #Biotech, #Biotechnology, #AnaxLaboratories, #Pharma



AS ON FEB2026 4.574 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT

join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE

join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com

References
- “Netanasvir phosphate – Sunshine Lake Pharma”. Adis Insight. Springer Nature Switzerland AG.
- “Netanasvir Phosphate Capsules Approved for Marketing by China NMPA”. National Medical Products Administration. 2025-06-11.
 | |
| Clinical data | |
|---|---|
| Trade names | 东卫卓; Dongweizhuo |
| Legal status | |
| Legal status | Rx in China |
| Identifiers | |
| IUPAC name | |
| CAS Number | 2007900-70-9 |
| PubChem CID | 122535557 |
| UNII | 4Y7YD32BYY |
| Chemical and physical data | |
| Formula | C51H58N8O7 |
| Molar mass | 895.074 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| SMILES | |
| InChI | |
//////////netanasvir, anax labs, APPROVALS 2025, CHINA 2025, antiviral, Dongweizhuo, HCV, Antaitavir Hasophate, HEC 74647 PA, 4Y7YD32BYY
Bulevirtide-gmod
Bulevirtide-gmod
CAS 2012558-47-1.
MF C248H355N65O72 MW 5399 g/mol
FDA 2026, APPROVALS 2026, 5/22/2026, Hepcludex, WKM56H3TLB
To treat chronic hepatitis delta virus infection in adults without cirrhosis or with compensated cirrhosis
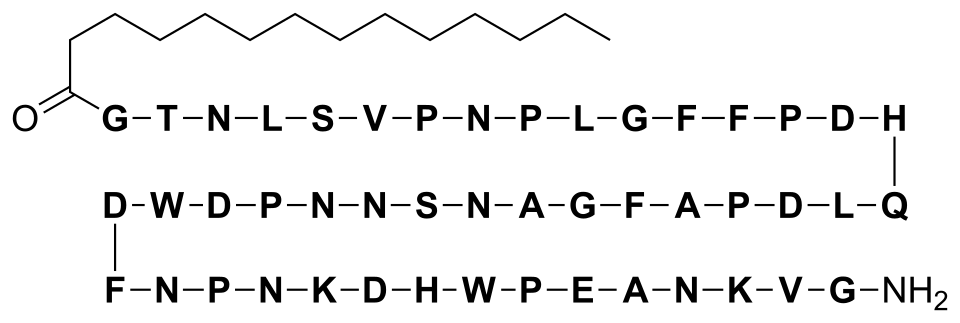
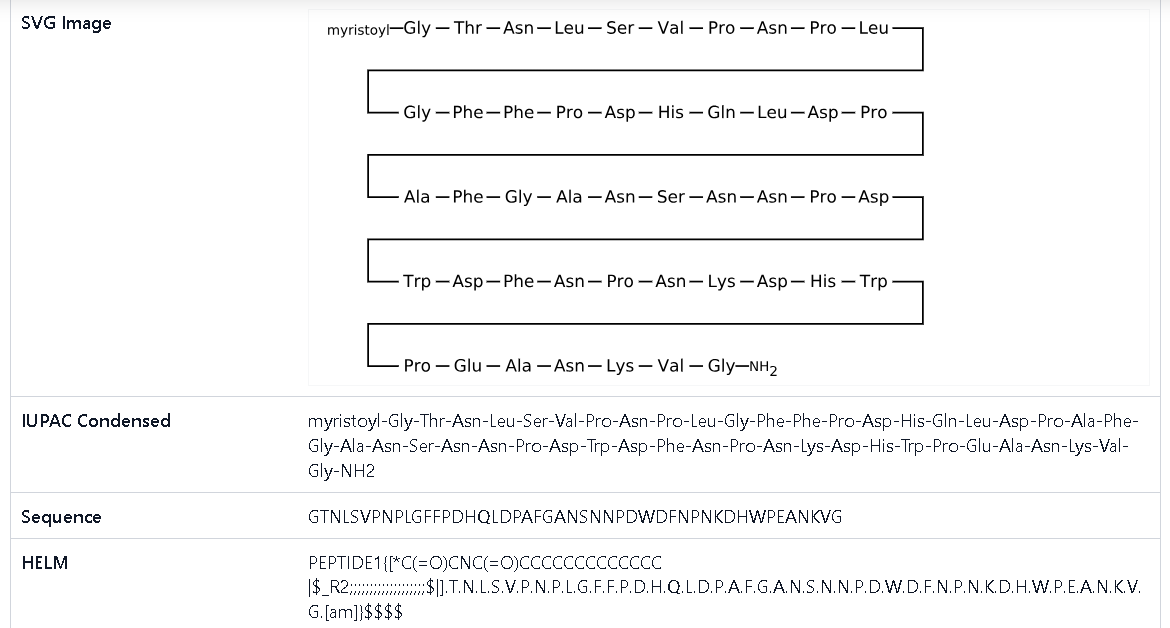
N-myristoyl-glycyl-L-threonyl-L-asparagyl-L-leucyl-L-seryl-L-valyl-L-prolyl-L-asparagyl-L-prolyl-L-leucyl-glycyl-L-phenylalanyl-L-phenylalanyl-L-prolyl-L-alpha-aspartyl-L-histidyl-L-glutaminyl-L-leucyl-L-alpha-aspartyl-L-prolyl-L-alanyl-L-phenylalanyl-glycyl-L-alanyl-L-asparagyl-L-seryl-L-asparagyl-L-asparagyl-L-prolyl-L-alpha-aspartyl-L-tryptophyl-L-alpha-aspartyl-L-phenylalanyl-L-asparagyl-L-prolyl-L-asparagyl-L-lysyl-L-alpha-aspartyl-L-histidyl-L-tryptophyl-L-prolyl-L-alpha-glutamyl-L-alanyl-L-asparagyl-L-lysyl-L-valyl-glycinamide
(4S)-4-[[(2S)-1-[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-6-amino-2-[[(2S)-4-amino-2-[[(2S)-1-[(2S)-4-amino-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-1-[(2S)-4-amino-2-[[(2S)-4-amino-2-[[(2S)-2-[[(2S)-4-amino-2-[[(2S)-2-[[2-[[(2S)-2-[[(2S)-2-[[(2S)-1-[(2S)-2-[[(2S)-2-[[(2S)-5-amino-2-[[(2S)-2-[[(2S)-2-[[(2S)-1-[(2S)-2-[[(2S)-2-[[2-[[(2S)-2-[[(2S)-1-[(2S)-4-amino-2-[[(2S)-1-[(2S)-2-[[(2S)-2-[[(2S)-2-[[(2S)-4-amino-2-[[(2S,3R)-3-hydroxy-2-[[2-(tetradecanoylamino)acetyl]amino]butanoyl]amino]-4-oxobutanoyl]amino]-4-methylpentanoyl]amino]-3-hydroxypropanoyl]amino]-3-methylbutanoyl]pyrrolidine-2-carbonyl]amino]-4-oxobutanoyl]pyrrolidine-2-carbonyl]amino]-4-methylpentanoyl]amino]acetyl]amino]-3-phenylpropanoyl]amino]-3-phenylpropanoyl]pyrrolidine-2-carbonyl]amino]-3-carboxypropanoyl]amino]-3-(1H-imidazol-4-yl)propanoyl]amino]-5-oxopentanoyl]amino]-4-methylpentanoyl]amino]-3-carboxypropanoyl]pyrrolidine-2-carbonyl]amino]propanoyl]amino]-3-phenylpropanoyl]amino]acetyl]amino]propanoyl]amino]-4-oxobutanoyl]amino]-3-hydroxypropanoyl]amino]-4-oxobutanoyl]amino]-4-oxobutanoyl]pyrrolidine-2-carbonyl]amino]-3-carboxypropanoyl]amino]-3-(1H-indol-3-yl)propanoyl]amino]-3-carboxypropanoyl]amino]-3-phenylpropanoyl]amino]-4-oxobutanoyl]pyrrolidine-2-carbonyl]amino]-4-oxobutanoyl]amino]hexanoyl]amino]-3-carboxypropanoyl]amino]-3-(1H-imidazol-4-yl)propanoyl]amino]-3-(1H-indol-3-yl)propanoyl]pyrrolidine-2-carbonyl]amino]-5-[[(2S)-1-[[(2S)-4-amino-1-[[(2S)-6-amino-1-[[(2S)-1-[(2-amino-2-oxoethyl)amino]-3-methyl-1-oxobutan-2-yl]amino]-1-oxohexan-2-yl]amino]-1,4-dioxobutan-2-yl]amino]-1-oxopropan-2-yl]amino]-5-oxopentanoic acid
Bulevirtide-gmod, sold under the brand name Hepcludex, is the first and only FDA-approved medication for treating chronic hepatitis delta virus (HDV) infection in adults. Developed by Gilead Sciences, it received accelerated approval from the U.S. Food and Drug Administration (FDA) on May 22, 2026, filling a critical gap for patients with this severe viral liver disease.
Indication and Clinical Use
- Target Patient Profile: Approved for adults with chronic HDV who have compensated cirrhosis or no cirrhosis.
- The Clinical Need: HDV only occurs as a co-infection in individuals who already have Hepatitis B (HBV). It is considered the most aggressive form of viral hepatitis, often accelerating liver scarring (fibrosis), liver failure, and liver cancer.
- Basis of Approval: The FDA granted accelerated approval based on Phase 3 MYR301 study data, which demonstrated a significant reduction in viral HDV RNA and the normalization of alanine aminotransferase (ALT) liver enzymes.
Mechanism of Action
Bulevirtide-gmod is a first-in-class entry inhibitor. It works by binding to and blocking the sodium taurocholate co-transporting polypeptide (NTCP) receptor on liver cells. Because HDV and HBV rely on this specific receptor to enter hepatocytes, the drug successfully disrupts the viral life cycle and prevents the virus from spreading to healthy liver cells.
Dosage and Administration
- Form: Supplied as a lyophilized powder for injection.
- Dose: The recommended dose is 8.5 mg once daily.
- Administration: Delivered via subcutaneous injection (under the skin).
Safety and Side Effects
- Boxed Warning: The drug carries a prominent warning regarding the risk of severe acute exacerbations of hepatitis D and B if treatment is discontinued. Stopping the medication can cause severe, life-threatening viral flares, requiring close medical monitoring for at least 6 months post-treatment.
- Common Side Effects: The most frequent adverse reactions of patients) include:
- Injection site reactions
- Headache
- Abdominal pain
- Fatigue
- Pruritus (itching)
Bulevirtide, sold under the brand name Hepcludex, is an antiviral medication used for the treatment of chronic hepatitis D (in the presence of hepatitis B).[8]
The most common side effects include raised levels of bile salts in the blood and reactions at the site of injection.[8]
Bulevirtide works by attaching to and blocking a receptor (target) through which the hepatitis delta and hepatitis B viruses enter liver cells.[8] By blocking the entry of the virus into the cells, it limits the ability of HDV to replicate and its effects in the body, reducing symptoms of the disease.[8]
Bulevirtide was approved for medical use in the European Union in July 2020,[8] and in Canada in August 2025.[5]
Medical uses
Bulevirtide is indicated for the treatment of chronic hepatitis delta virus (HDV) infection in plasma (or serum) HDV-RNA positive adult patients with compensated liver disease.[8][10]
Pharmacology
Mechanism of action
Bulevirtide binds and inactivates the sodium/bile acid cotransporter, blocking both hepatitis B and hepatitis D viruses from entering hepatocytes.[11]
The hepatitis B virus uses its surface lipopeptide pre-S1 for docking to mature liver cells via their sodium/bile acid cotransporter (NTCP) and subsequently entering the cells. Myrcludex B is a synthetic N-acylated pre-S1[12][13] that can also dock to NTCP, blocking the virus’s entry mechanism.[14]
Bulevirtide is also effective against hepatitis D because the hepatitis D virus uses the same entry receptor as the hepatitis B virus and is only effective in the presence of a hepatitis B virus infection.[14]
Pre-clinical data in mice suggests that pharmacological inhibition of NTCP-mediated bile salt uptake may also be effective to lower hepatic bile salt accumulation in cholestatic conditions. This reduces hepatocellular damage.[15] An increased ratio of phospholipid to bile salts seen in bile upon NTCP inhibition may further contribute to the protective effect as bile salts are less toxic in presence of phospholipids.[16]
Structural formula
Bulevirtide is a 47-amino acid peptide with the following sequence:[17]
CH3(CH2)12CO–Gly–Thr–Asn–Leu–Ser–Val–Pro-Asn-Pro-Leu-Gly-Phe-Phe-Pro-Asp–His–Gln-Leu-Asp-Pro-Ala-Phe-Gly-Ala-Asn-Ser-Asn-Asn-Pro-Asp-Trp-Asp-Phe-Asn-Pro-Asn-Lys-Asp-His-Trp-Pro-Glu-Ala-Asn-Lys-Val-Gly-NH2 (C13H27CO-GTNLSVPNPLGFFPDHQLDPAFGANSNNPDWDFNPNKDHWPEANKVG-NH2)
SYN
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2024073572&_cid=P11-MPNG4J-82875-1
PATENTS
- Therapy of atherosclerosis, primary biliary cirrhosis and nrlp3 inflammasome-associated disease by htcp inhibitorsPublication Number: EP-3392267-A1Priority Date: 2017-04-18
- Therapy of atherosclerosis, primary biliary cirrhosis and nrlp3 inflammasome-associated disease by htcp inhibitorsPublication Number: US-2018296634-A1Priority Date: 2017-04-18
- Therapy of atherosclerosis, primary biliary cirrhosis and nrlp3 inflammasome-associated disease by htcp inhibitorsPublication Number: US-2021196786-A1Priority Date: 2017-04-18
- Therapy of atherosclerosis, primary biliary cirrhosis and NRLP3 inflammasome-associated disease by HTCP inhibitorsPublication Number: US-10925925-B2Priority Date: 2017-04-18Grant Date: 2021-02-23
- Combination therapy of hbv and hdv infectionPublication Number: EP-3204030-B1Priority Date: 2014-10-07Grant Date: 2022-04-27
- Combination therapy of hbv and hdv infectionPublication Number: EP-4098273-A1Priority Date: 2014-10-07
- Combination therapy of hbv and hdv infectionPublication Number: US-2022040178-A1Priority Date: 2014-10-07
ADVERTISEMENT
ANAX LABORATORIES
WEBSITE https://www.anaxlab.com/
Discovery Solutions, Supporting the chemistry needs of clients in the Medical, Analytical and Bio Sciences
Development Solutions, Developing from Lab scale to PR&D, Kilo Scale-ups and Commercial Scales
SEE MORE………Integrated Solutions, Manufacturing Solutions, Products,
Can’t Find? Let’s Connect
Phone : +91 897704 2010 / +91 9177075735, Email : info@anaxlab.com
#MedicinalChemistry, #DrugDiscovery, #OrganicSynthesis, #ChemicalLibrary, #BuildingBlocks, #SARStudies, #ChemistryInnovation, #medchem, #Drugdevelopment, #Biotech, #Biotechnology, #AnaxLaboratories, #Pharma
AS ON FEB2026 4.574 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
References
References
- Deterding K, Wedemeyer H (2019). “Beyond Pegylated Interferon-Alpha: New Treatments for Hepatitis Delta”. AIDS Reviews. 21 (3): 126–134. doi:10.24875/AIDSRev.19000080. PMID 31532397. S2CID 202674681.
- “Hepcludex (bulevirtide acetate)”. Therapeutic Goods Administration (TGA). 12 August 2024. Retrieved 12 October 2024.
- “Therapeutic Goods (Poisons Standard—June 2024) Instrument 2024”. Federal Register of Legislation. 30 May 2024. Retrieved 10 June 2024.
- “Hepcludex (Gilead Sciences Pty Ltd)”. Therapeutic Goods Administration (TGA). 13 September 2024. Retrieved 15 September 2024.
- “Hepcludex Product information”. Health Canada. 8 August 2025. Retrieved 20 August 2025.
- “Summary Basis of Decision for Hepcludex”. Drug and Health Products Portal. 29 September 2025. Retrieved 12 October 2025.
- “Hepcludex 2 mg powder for solution for injection – Summary of Product Characteristics (SmPC)”. (emc). 30 March 2022. Retrieved 1 July 2022.
- “Hepcludex EPAR”. European Medicines Agency (EMA). 26 May 2020. Retrieved 12 August 2020. Text was copied from this source which is copyright European Medicines Agency. Reproduction is authorized provided the source is acknowledged.
- “Hepcludex Product information”. Union Register of medicinal products. Retrieved 3 March 2023.
- “Summary of opinion: Hepcludex” (PDF). European Medicines Agency (EMA). 28 May 2020.
- Francisco EM (29 May 2020). “Hepcludex”. European Medicines Agency (EMA). Archived from the original on 15 June 2020. Retrieved 6 August 2020.
- Volz T, Allweiss L, Ben MBarek M, Warlich M, Lohse AW, Pollok JM, et al. (May 2013). “The entry inhibitor Myrcludex-B efficiently blocks intrahepatic virus spreading in humanized mice previously infected with hepatitis B virus”. Journal of Hepatology. 58 (5): 861–867. doi:10.1016/j.jhep.2012.12.008. PMID 23246506.
- Abbas Z, Abbas M (August 2015). “Management of hepatitis delta: Need for novel therapeutic options”. World Journal of Gastroenterology. 21 (32): 9461–9465. doi:10.3748/wjg.v21.i32.9461. PMC 4548107. PMID 26327754.
- Spreitzer H (14 September 2015). “Neue Wirkstoffe – Myrcludex B”. Österreichische Apothekerzeitung (in German) (19/2015): 12.
- Na+ -taurocholate cotransporting polypeptide inhibition has hepatoprotective effects in cholestasis in mice. Slijepcevic D, Roscam Abbing RLP, Fuchs CD, Haazen LCM, Beuers U, Trauner M, Oude Elferink RPJ, van de Graaf SFJ. Hepatology. 2018 Sep;68(3):1057-1069. doi: 10.1002/hep.29888
- Roscam Abbing RL, Slijepcevic D, Donkers JM, Havinga R, Duijst S, Paulusma CC, et al. (January 2020). “Blocking Sodium-Taurocholate Cotransporting Polypeptide Stimulates Biliary Cholesterol and Phospholipid Secretion in Mice”. Hepatology. 71 (1): 247–258. doi:10.1002/hep.30792. PMC 7003915. PMID 31136002.
- Sauter M, Blank A, Stoll F, Lutz N, Haefeli WE, Burhenne J (September 2021). “Intact plasma quantification of the large therapeutic lipopeptide bulevirtide”. Analytical and Bioanalytical Chemistry. 413 (22): 5645–5654. doi:10.1007/s00216-021-03384-7. PMC 8410713. PMID 34018034.
| Clinical data | |
|---|---|
| Pronunciation | /bjuːˈlɛvɪrtaɪd/ byoo-LEH-vir-tyde |
| Trade names | Hepcludex |
| Other names | MyrB, Myrcludex-B[1] |
| License data | US DailyMed: Bulevirtide |
| Pregnancy category | AU: B1[2] |
| Routes of administration | Subcutaneous |
| ATC code | J05AX28 (WHO) |
| Legal status | |
| Legal status | AU: S4 (Prescription only)[3][4][2]CA: ℞-only[5][6]UK: POM (Prescription only)[7]EU: Rx-only[8][9] |
| Identifiers | |
| CAS Number | 2012558-47-1 |
| DrugBank | DB15248 |
| ChemSpider | 129157549 |
| UNII | WKM56H3TLB |
| KEGG | D11877as salt: D11878 |
| ChEMBL | ChEMBL4297711 |
| Chemical and physical data | |
| Formula | C248H355N65O72 |
| Molar mass | 5398.951 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| SMILES | |
| InChI | |
/////////Bulevirtide-gmod, ANAX LABS, FDA 2026, APPROVALS 2026, Hepcludex, WKM56H3TLB, ANTIVIRALS
Encofosbuvir
Encofosbuvir, Yiqibuvir
CAS 2232134-77-7
MF C30H42FN4O13PS MW 748.7 g/mol
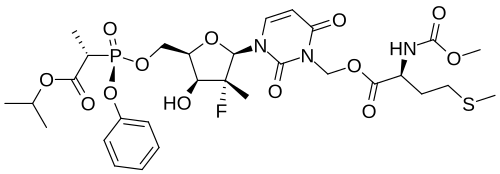
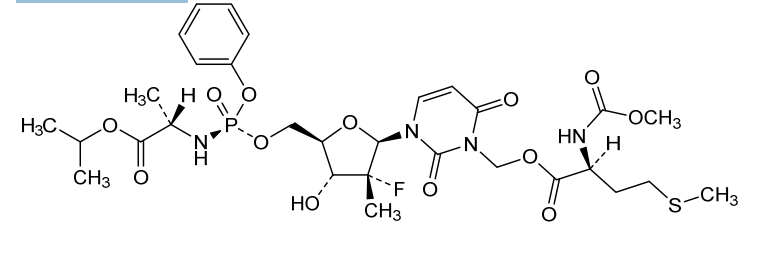
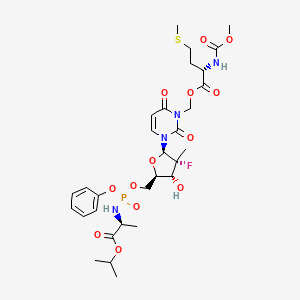
- L-Alanine, O3-[N-(methoxycarbonyl)-L-methionyl]-[P(S),2’R]-2′-deoxy-2′-fluoro-3-(hydroxymethyl)-2′-methyl-P-phenyl-5′-uridylyl-, 1-methylethyl ester
- O3-[N-(Methoxycarbonyl)-L-methionyl]-[P(S),2’R]-2′-deoxy-2′-fluoro-3-(hydroxymethyl)-2′-methyl-P-phenyl-5′-uridylyl-L-alanine 1-methylethyl ester
[3-[(2R,3R,4R,5R)-3-fluoro-4-hydroxy-3-methyl-5-[[[[(2S)-1-oxo-1-propan-2-yloxypropan-2-yl]amino]-phenoxyphosphoryl]oxymethyl]oxolan-2-yl]-2,6-dioxopyrimidin-1-yl]methyl (2S)-2-(methoxycarbonylamino)-4-methylsulfanylbutanoate

antiviral, HEC 110114; Yiqibuvir, CHINA 2025, APPROVALS 2025, 82E4Q8WQV7
Encofosbuvir is a novel, oral small-molecule direct-acting antiviral (DAA) drug used to treat the hepatitis C virus (HCV). Approved by China’s National Medical Products Administration (NMPA) in March 2025, it serves as a core component of a domestic, pan-genotypic treatment regimen.
🔬 Mechanism of Action
Encofosbuvir works by targeting the machinery the virus needs to replicate itself:
- Target Enzyme: It functions as an HCV NS5B RNA-dependent RNA polymerase inhibitor.
- Viral Suppression: By selectively binding to this polymerase, it blocks the synthesis of viral RNA, effectively halting the replication and spread of the hepatitis C virus in mammals
Clinical Indications and Usage
According to the official regulatory updates from the China NMPA, encofosbuvir is prescribed under specific clinical parameters:
- Combination Therapy: It must be used in combination with netanasvir (specifically netanasvir phosphate capsules).
- Target Genotypes: The regimen is highly effective across multiple viral strains, covering HCV genotypes 1, 2, 3, and 6.
- Patient Profile: It is indicated for adult patients who are treatment-naïve (never treated before) or who have been previously treated with interferon. It is safe for use in patients with or without compensated liver cirrhosis.
The drug is classified as a Class 1 innovative drug, representing a milestone in self-developed, domestic intellectual property:
- Developers: It was jointly developed and brought to market by Sunshine Lake Pharma (a subsidiary of HEC Pharm) and YiChang HEC ChangJiang Pharmaceutical Co., Ltd.
- Dosage Form: It is distributed commercially as 0.3g tablets.
- Therapeutic Context: This medication expands the developer’s innovative hepatitis C pipeline, building upon their previously approved portfolio like emitasvir phosphate
- OriginatorHEC Pharm; Sunshine Lake Pharma
- DeveloperSunshine Lake Pharma
- ClassAntivirals
- Mechanism of ActionHepatitis C virus NS 5 protein inhibitors
- RegisteredHepatitis C
- 27 Mar 2025Registered for Hepatitis C (Combination therapy, Treatment-naive) in China (PO)
- 08 Feb 2025Preregistered for Hepatitis C (Combination therapy, Treatment-experienced) in China (PO)
- 08 Feb 2025Registered for Hepatitis C (Combination therapy, Treatment-experienced) in China (PO)
Encofosbuvir is an antiviral drug used to treat hepatitis C virus (HCV). In China, encofosbuvir is approved for use in combination with netanasvir for the treatment of adult patients with chronic HCV genotypes 1, 2, 3, or 6, who are either treatment-naive or have been previously treated with interferon.[1]
SYN
[0515](S)-(3-((2R,3R,4R,5R)-3-fluoro-4-hydroxy-5-((((S)-(((S)-1-isopropoxy-1-oxopropyl-2-yl)amino)(phenoxy)phosphoryl)oxy)methyl)-3-methyltetrahydrofuran-2-yl)-2,6-dioxo-2,3-dihydropyrimidin-1(6H)-yl)methyl-2-((methoxycarbonyl)amino)-4-(methylthio)butyrate
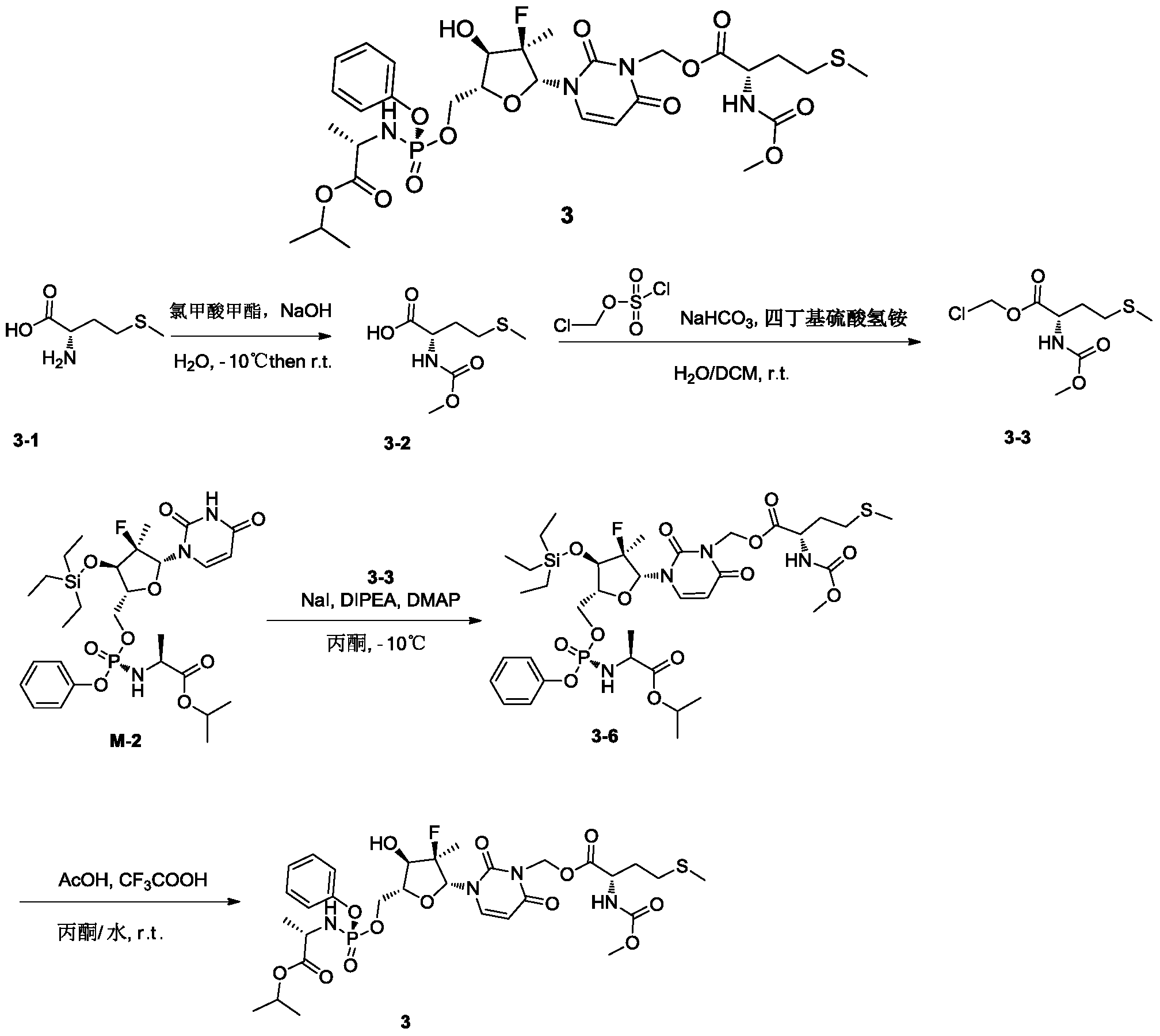
[0531]4) Synthesis of compound 3
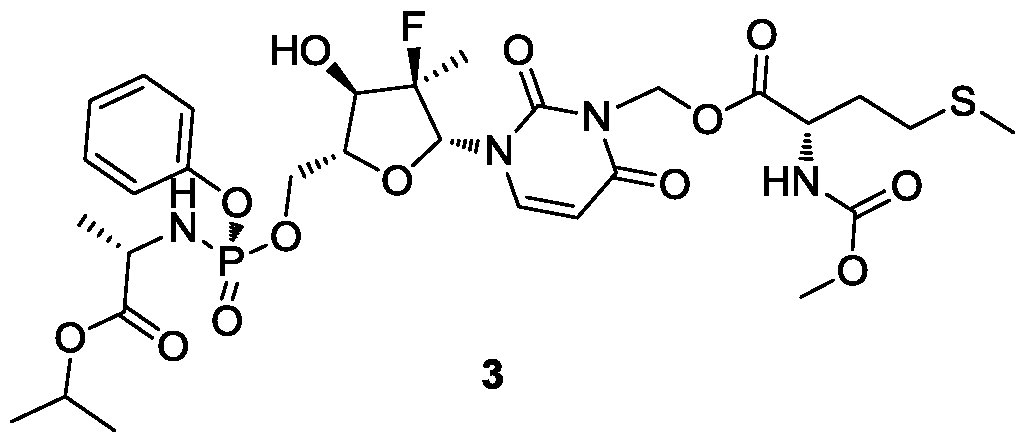
Compound 3-6 (3.63 g, 4.2 mmol, 1 eq) was dissolved in acetone (12 mL), and water (9 mL), trifluoroacetic acid (3 mL), and glacial acetic acid (12 mL) were added sequentially at room temperature, followed by a reaction time of 2 hours. After the reaction was monitored by TLC until complete, 30 mL of dichloromethane was added to the reaction solution, stirred thoroughly, and allowed to stand for phase separation. The organic phase was washed sequentially with water (10 mL × 3), saturated sodium chloride (10 mL), dried over anhydrous sodium sulfate, and the solvent was removed under reduced pressure. The solution was purified by column chromatography using DCM:MeOH = 50:1 as the eluent, yielding 2.8 g of a white foamy solid.
[0534]MS-ESI: m/z 748.8[M+1] +;
[0535]
1H NMR(400MHz,CDCl 3)δ7.49(d,J=8.2Hz,1H),7.34(d,J=7.6Hz,2H),7.24–7.16(m,3H),6.19(d,J=17.3Hz,1H),6.07–5.94(m,2H),5.75(d,J=8.3Hz,1H),5.41(d,J=7.4Hz,1H),5.07–4.95(m,1H),4.58–4.39(m,3H),4.12(d,J=8.6Hz,1H),4.02–3.80(m,4H),3.67(s,3H),2.52(t,J=7.5Hz,2H),2.14–1.90(m,5H),1.37(dd,J=18.4,14.3Hz,6H),1.24(d,J=6.3Hz,6H)。
ANAX LABORATORIES
WEBSITE https://www.anaxlab.com/
Discovery Solutions, Supporting the chemistry needs of clients in the Medical, Analytical and Bio Sciences
Development Solutions, Developing from Lab scale to PR&D, Kilo Scale-ups and Commercial Scales
SEE MORE………Integrated Solutions, Manufacturing Solutions, Products,
Can’t Find? Let’s Connect
Phone : +91 897704 2010 / +91 9177075735, Email : info@anaxlab.com
#MedicinalChemistry, #DrugDiscovery, #OrganicSynthesis, #ChemicalLibrary, #BuildingBlocks, #SARStudies, #ChemistryInnovation, #medchem, #Drugdevelopment, #Biotech, #Biotechnology, #AnaxLaboratories, #Pharma
AS ON FEB2026 4.574 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
References
“Netanasvir Phosphate Capsules Approved for Marketing by China NMPA”. National Medical Products Administration. 2025-06-11.
| Clinical data | |
|---|---|
| Trade names | 英强布韦 |
| Legal status | |
| Legal status | Rx in China |
| Identifiers | |
| IUPAC name | |
| CAS Number | 2232134-77-7 |
| PubChem CID | 141522644 |
| UNII | 82E4Q8WQV7 |
| Chemical and physical data | |
| Formula | C30H42FN4O13PS |
| Molar mass | 748.71 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| SMILES | |
| InChI | |
//////////encofosbuvir, anax labs, antiviral, HEC 110114; Yiqibuvir, CHINA 2025, APPROVALS 2025, 82E4Q8WQV7
Suricapavir
Suricapavir
CAS 2417270-21-2
MF C41H29ClF9N9O4S MF950.2 g/mol
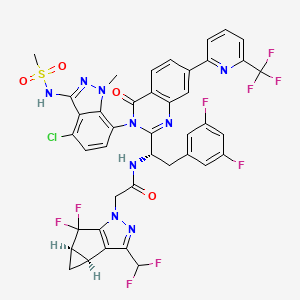
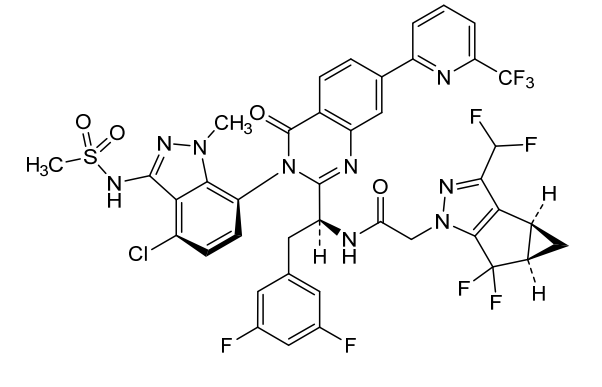
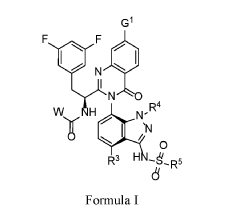
N-[(1S)-1-[3-[4-chloro-3-(methanesulfonamido)-1-methylindazol-7-yl]-4-oxo-7-[6-(trifluoromethyl)-2-pyridinyl]quinazolin-2-yl]-2-(3,5-difluorophenyl)ethyl]-2-[(2S,4R)-9-(difluoromethyl)-5,5-difluoro-7,8-diazatricyclo[4.3.0.02,4]nona-1(6),8-dien-7-yl]acetamide
N-[(1S)-1-[3-[4-chloro-3-(methanesulfonamido)-1-methyl-indazol-7-yl]-4-oxo-7-[6-(trifluoromethyl)-2-pyridyl]quinazolin-2-yl]-2-(3,5-difluorophenyl)ethyl]-2-[(2S,4R)-9-(difluoromethyl)-5,5-difluoro-7,8-diazatricyclo[4.3.0.02,4]nona-1(6),8-dien-7-yl]acetamide
N-[(1S)-1-{(3P)-3-[4-chloro-3-(methanesulfonamido)-1-methyl-1Hindazol-7-yl]-4-oxo-7-[6-(trifluoromethyl)pyridin-2-yl]-3,4-
dihydroquinazolin-2-yl}-2-(3,5-difluorophenyl)ethyl]-2-[(3bS,4aR)-3-
(difluoromethyl)-5,5-difluoro-3b,4,4a,5-tetrahydro-1Hcyclopropa[3,4]cyclopenta[1,2-c]pyrazol-1-yl]acetamide
inhibitor of viral replication, antiviral, ZZ799EX5KN
tructurally resembles:
- Lenacapavir-type macroheterocyclic capsid inhibitors (Gilead class)
PAT
Preparation of Example 59: N-((S)-1-((3P)-3-(4-chloro-1-methyl-3-(methylsulfonamido)-1H-indazol-7-yl)-4-oxo-7-(6-(trifluoromethyl)pyridin-2-yl)-3,4-dihydroquinazolin-2-yl)-2- (3,5-difluorophenyl)ethyl)-2-((3bS,4aR)-3-(difluoromethyl)-5,5-difluoro-3b,4,4a,5- tetrahydro-1H-cyclopropa[3,4]cyclopenta[1,2-c]pyrazol-1-yl)acetamide.
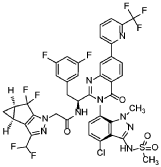
The title compound was prepared according to General Procedure D using 2-chloro-6-(trifluoromethyl)pyridine as the coupling partner. The experiment afforded the title compound, N-((S)-1-((3P)-3-(4-chloro-1-methyl-3-(methylsulfonamido)-1H-indazol-7-yl)-4-oxo-7-(6-(trifluoromethyl)pyridin-2-yl)-3,4-dihydroquinazolin-2-yl)-2-(3,5-difluorophenyl)ethyl)-2-((3bS,4aR)-3-(difluoromethyl)-5,5-difluoro-3b,4,4a,5-tetrahydro-1H-cyclopropa[3,4]cyclopenta[1,2-c]pyrazol-1-yl)acetamide. The sample was analyzed using LCMS Method F: retention time = 1.51 min.; observed ion = 948.4 (M-H).1H NMR (METHANOL-d4, 500 MHz) Shift 8.66 (s, 1H), 8.4-8.4 (m, 3H), 8.22 (t, 1H, J=7.9 Hz), 7.88 (d, 1H, J=7.7 Hz), 7.28 (br d, 1H, J=8.0 Hz), 7.20 (d, 1H, J=7.7 Hz), 6.7-6.8 (m, 1H), 6.61 (dd, 2H, J=2.2, 8.2 Hz), 6.67 (br t, 2H, J=54.7 Hz), 4.5-4.6 (m, 2H), 3.61 (s, 3H), 3.4-3.5 (m, 1H), 3.2-3.2 (m, 3H), 3.1-3.2 (m, 1H), 2.41 (br dd, 2H, J=3.7, 7.3 Hz), 1.34 (br d, 1H, J=5.4 Hz), 0.99 (br dd, 1H, J=1.9, 3.7 Hz)
PAT
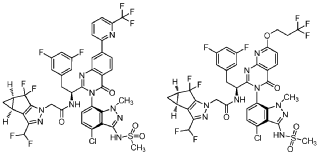
WO 2020/084492 and WO 2020/254985 disclose certain Capsid Inhibitor compounds including the two compounds shown below which will be referred to in this application as the compounds of Formula la and Formula lb.
PAT
- Inhibitors of human immunodeficiency virus replicationPublication Number: WO-2023062559-A1Priority Date: 2021-10-13
- Inhibitors of human immunodeficiency virus replicationPublication Number: US-2023149408-A1Priority Date: 2020-04-15
- Inhibitors of human immunodeficiency virus replicationPublication Number: WO-2021209900-A1Priority Date: 2020-04-15
- Pharmaceutical compositions comprising cabotegravirPublication Number: US-2023045509-A1Priority Date: 2019-12-09
- Inhibitors of human immunodeficiency virus replicationPublication Number: US-11541055-B2Priority Date: 2018-10-24Grant Date: 2023-01-03
- Inhibitors of human immunodeficiency virus replicationPublication Number: US-2020360384-A1Priority Date: 2018-10-24
- Inhibitors of human immunodeficiency virus replicationPublication Number: EP-3870577-B1Priority Date: 2018-10-24Grant Date: 2025-03-19
ADVERTISEMENT
ANAX LABORATORIES
WEBSITE https://www.anaxlab.com/
Discovery Solutions, Supporting the chemistry needs of clients in the Medical, Analytical and Bio Sciences
Development Solutions, Developing from Lab scale to PR&D, Kilo Scale-ups and Commercial Scales
SEE MORE………Integrated Solutions, Manufacturing Solutions, Products,
Can’t Find? Let’s Connect

Phone : +91 897704 2010 / +91 9177075735, Email : info@anaxlab.com
#MedicinalChemistry, #DrugDiscovery, #OrganicSynthesis, #ChemicalLibrary, #BuildingBlocks, #SARStudies, #ChemistryInnovation, #medchem, #Drugdevelopment, #Biotech, #Biotechnology, #AnaxLaboratories, #Pharma
AS ON FEB2026 4.574 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
///////////////suricapavir, ANAX, inhibitor of viral replication, antiviral, ZZ799EX5KN
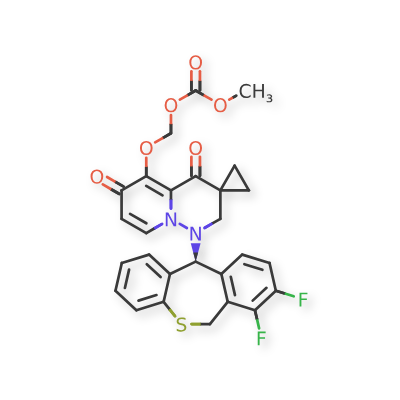
Pixavir marboxil
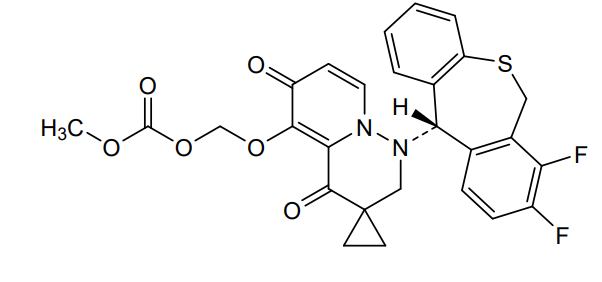
Pixavir marboxil
CAS 2365473-17-0
MF C27H22F2N2O6S MW540.535
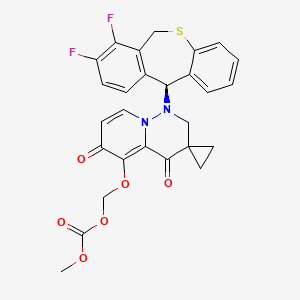
(1-((11S)-7,8-DIFLUORO-6,11-DIHYDROBENZO(C)(1)BENZOTHIEPIN-11-YL)-4,6-DIOXOSPIRO(2H-PYRIDO(1,2-B)PYRIDAZINE-3,1′-CYCLOPROPANE)-5-YL)OXYMETHYL METHYL CARBONATE
({1′-[(11S)-7,8-difluoro-6,11-dihydrodibenzo[b,e]thiepin-11-yl]-4′,6′-dioxo1′,2′,4′,6′-tetrahydrospiro[cyclopropane-1,3′-pyrido[1,2-b]pyridazin]-5′-yl}oxy)methyl methyl carbonate
antiviral, TG 1000, Yi Li Kang, SV42843XSX, Cap-dependent endonuclease-IN-1, Influenza virus infections, TaiGen Biotechnology
- OriginatorTaiGen Biotechnology
- Class3-ring heterocyclic compounds; Antivirals; Benzene derivatives; Carbonates; Cyclopropanes; Dibenzothiepins; Esters; Ethers; Fluorobenzenes; Organic sulfur compounds; Pyridazines; Pyridones; Small molecules; Spiro compounds
- Mechanism of ActionEndonuclease inhibitors; Virus replication inhibitors
- MarketedInfluenza virus infections
- 27 Feb 2026Launched for Influenza virus infections (In adults, In adolescents) in China (PO), prior to February 2026 (TaiGen Biotechnology pipeline, February 2026)
- 26 Jan 2026Pixavir marboxil licensed to Boryung Biopharma for commercialization in South Korea
- 16 Dec 2025Chemical structure information added.
Pixavir marboxil (also known as TG-1000) is an investigational antiviral drug designed to treat and inhibit influenza virus infections. It belongs to a class of compounds known as cap-dependent endonuclease (CEN) inhibitors, which target a key viral enzyme necessary for influenza virus replication.
Mechanism of Action
- Blocks viral replication: Pixavir marboxil works by inhibiting the influenza virus’s cap-dependent endonuclease, a part of the viral RNA polymerase complex the virus needs to “snatch” capped RNA fragments from host cell mRNA. Without this process, the virus cannot efficiently produce its own viral proteins or replicate.
What Viruses It Targets
Pixavir marboxil has shown activity against:
- Influenza A viruses
- Influenza B viruses
- Certain drug-resistant influenza strains
This broad spectrum makes it useful for seasonal flu and potentially strains less responsive to older antiviral drugs
Clinical Development & Approval Status
Phase Trials & Results
- Completed Phase III: Clinical trials in adults and adolescents (age ≥12) showed that a single dose shortened time to symptom relief compared to placebo (e.g., median ~60.9 h vs ~87.9 h).
- Symptom relief benefits: The data indicated statistically significant improvement in flu symptoms and faster viral inactivation in treated patients versus placebo.
- Pediatric Formulation: China’s health authority approved pediatric Phase III studies for Pixavir (children <12), indicating further development for younger patients.
Regulatory Filings
- NDA (New Drug Application): Pixavir marboxil has been submitted for approval to the National Medical Products Administration (NMPA) in mainland China based on Phase III results.
- Generic Name Approved: The drug has been officially recognized with the generic name “Pixavir marboxil,” moving it closer to commercialization.
Pixavir marboxil is a small molecule drug. The usage of the INN stem ‘-xavir’ in the name indicates that Pixavir marboxil is a influenza CAP-dependent endonuclease inhibitor. Pixavir marboxil has a monoisotopic molecular weight of 540.12 Da.
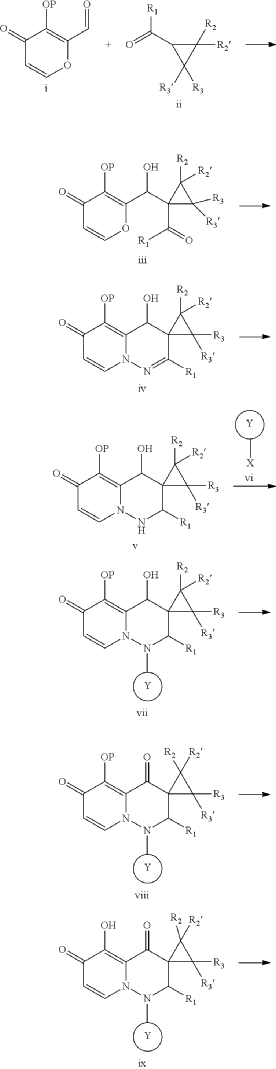
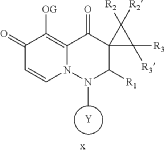
SYN
PAT
- Cap-dependent endonuclease inhibitorsPublication Number: US-10596171-B2Patent Family: AU-2019209426-A1; AU-2019209426-B2; BR-112020014810-A2; CA-3078391-A1; CA-3078391-C; CL-2020001919-A1; CN-110300753-A; CN-110300753-B; CO-2020006411-A2; EA-202090658-A1; EP-3743424-A1; EP-3743424-A4; IL-274199-A; IL-274199-B; JO-P20200159-A1; JP-2021512146-A; JP-6994121-B2; KR-102432975-B1; KR-20200086385-A; MX-2020007722-A; MY-197875-A; NZ-763248-A; PE-20211240-A1; PH-12020550921-A1; SG-11202003014V-A; TW-201938166-A; TW-I714951-B; US-10596171-B2; US-2019224198-A1; WO-2019144089-A1; ZA-202002037-BPriority Date: 2018-01-22Grant Date: 2020-03-24Inventor(s): LIN CHU-CHUNG; CHEN HUNG-CHUAN; CHIANG CHIAYN; YEN CHI-FENG; HSU MING-CHUAssignee(s): TAIGEN BIOTECHNOLOGY CO LTD; HSU MING CHUClassification: A61K31/5025; A61P31/16Abstract: Provided is a compound of Formula (I) below, or a pharmaceutically acceptable salt, metabolite, or prodrug thereof: n nwherein: A 1 is CR 4 or N; A 2 is CR 5 R 6 or NR 7 ; A 3 is CR 5 ′R 6 ′ or NR 7 ′; each of R 1 , R 2 , R 2 ′, R 3 , R 3 ′, R 4 , R 5 , R 5 ′, R 6 , R 6 ′, R 7 , and R 7 ′, independently, is hydrogen, deuterium, halogen, cyano, hydroxyl, carboxyl, amino, formyl, nitro, C 1-6 alkyl, C 2-6 alkenyl, C 2-6 alkynyl, C 1-6 alkoxy, C 2-6 alkenyloxy, C 1-6 alkylcarbonyl, C 1-6 alkyloxycarbonyl, C 1-6 alkylamine, C 3-20 carbocyclyl, or C 3-20 heterocyclyl; or R 5 and R 6 , R 5 ′ and R 6 ′, or R 5 and R 5 ′, together with the adjacent atom to which they are each attached, form C 3-10 carbocyclyl or C 3-10 heterocyclyl. Further provided are a method of using the above-described compound, or the pharmaceutically acceptable salt, metabolite, or prodrug thereof for treating influenza and a pharmaceutical composition containing same.Linked Compounds: 274Linked Substances: 411
- Cap-dependent endonuclease inhibitorsPublication Number: US-2019224198-A1Priority Date: 2018-01-22Linked Compounds: 275Linked Substances: 411
AS ON FEB2026 4.574 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
////////////pixavir marboxil, antiviral, TG 1000, Yi Li Kang, SV42843XSX, Cap-dependent endonuclease-IN-1, Influenza virus infections, TaiGen Biotechnology
Dezecapavir




Dezecapavir
CAS 2570323-59-8
MF C37H29ClF9N9O5S MW918.19
1H-Cyclopropa[3,4]cyclopenta[1,2-c]pyrazole-1-acetamide, N-[(1S)-1-[(3S)-3-[4-chloro-1-methyl-3-[(methylsulfonyl)amino]-1H-indazol-7-yl]-3,4-dihydro-4-oxo-7-(3,3,3-trifluoropropoxy)pyrido[2,3-d]pyrimidin-2-yl]-2-(3,5-difluorophenyl)ethyl]-3-(difluoromethyl)-5,5-difluoro-3b,4,4a,5-tetrahydro-, (3bS,4aR)-
N-[(1S)-1-[(3P)-3-[4-chloro-3-(methanesulfonamido)-1-methyl-1H-indazol-7-yl]-4-oxo-7-(3,3,3-
trifluoropropoxy)-3,4-dihydropyrido[2,3-d]pyrimidin-2-yl]-2-(3,5-difluorophenyl)ethyl]-2-[(3bS,4aR)-3-
(difluoromethyl)-5,5-difluoro-3b,4,4a,5-tetrahydro-1Hcyclopropa[3,4]cyclopenta[1,2-c]pyrazol-1-
yl]acetamide
inhibitor of viral replication, antiviral, SEK9LN2LSM, VH 4011499, VH4011499, VH-4011499, VH 499, GSK2838232, GSK 2838232
Dezecapavir is a potent experimental antiviral compound, specifically a novel HIV-1 capsid inhibitor, developed to block HIV replication by targeting the virus’s capsid protein, showing high effectiveness in lab settings (low nM range EC50) and representing a new class of drugs for HIV treatment, potentially for long-acting injectable therapies. It’s a complex molecule with a unique structure designed to disrupt the HIV capsid assembly, halting the virus’s life cycle early on.
Key Characteristics:
- Mechanism: Inhibits HIV-1 capsid assembly, a crucial step in the viral lifecycle.
- Potency: Very effective in cell cultures, with a low nanomolar EC50 (effective concentration).
- Class: Belongs to a new class of antivirals, distinct from integrase or reverse transcriptase inhibitors, offering a novel approach to HIV treatment.
- Development: Under investigation, often mentioned as a potential candidate for long-acting injectable (LAI) treatments due to its potency.
What it does:
Dezecapavir binds to the HIV capsid, preventing the virus from uncoating and maturing, thereby stopping new infections from forming.
Significance:
It represents a promising new option for HIV treatment, especially in the context of growing resistance to existing drugs, and could be part of future long-acting regimens.
SYN
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2020254985&_cid=P20-MKHOOT-76990-1

Preparation of Example 1: N-((S)-l-((3P)-3-(4-chloro-l-methyl-3-(methylsulfonamido)-lH- indazol-7-yl)-4-oxo-7-(3,3,3-trifluoropropoxy)-3,4-dihydropyrido[2,3-d]pyrimidin-2-yl)-2-(3,5- difluorophenyl)ethyl)-2-((3bSr4aR)-3-(difluoromethyl)-5r5-difluoro-3br4r4ar5-tetrahydro-lH- cyciopropa[3, 4]cydopenta[ l,2-c]pyrazoi-l-yi)acetamide

A solution of diisopropyl (E)-diazene-l,2-dicarboxylate (“DIAD”, 0.125 ml, 0.637 mmol) in THF (0.2 mL) was added dropwise to a mixture of N-(l-((3P)-3-(4-chloro-3-(N-(4-methoxybenzyl)methylsulfonamido)-l-methyl-lH-indazol-7-yl)-7-hydroxy-4-oxo-3,4-dihydropyrido[2,3-d]pyrimidin-2-yl)-2-(3,5-difluorophenyl)ethyl)-2-((3bS,4aR)-3-(difluoromethyl)-5,5-difluoro-3b,4,4a,5-tetrahydro-lH-cyclopropa[3,4]cyclopenta[l,2-c]pyrazol-l-yl)acetamide (0.2 g, 0.212 mmol)), 3,3,3-trifluoropropan-l-ol (0.073 g, 0.637 mmol) and triphenylphosphine (0.178 g, 0.679 mmol) in Tetrahydrofuran (2.1 mL) at rt. The reaction mixture was stirred for 18 h at rt and then was concentrated in vacuo. The residue was purified on silica gel (24 g RediSep Gold column) using a gradient of 0-60 % ethyl acetate in hexanes over 15 CV, and then holding at 60 % ethyl acetate in hexanes for 5 CV. Fractions containing the pure product were pooled and then concentrated to give a yellow solid. This solid was taken up in DCM (1 mL):TFA (0.5 mL); the solution was cooled to 0 °C; and to the solution was added triflic acid (0.057 mL, 0.637 mmol). The mixture was stirred for 1 h and then concentrated in vacuo. The residue was taken up in ethyl acetate; washed with 1 N
NaOH; washed with 0.5M citric acid; dried over Na2SC>4; filtered; and then was concentrated in vacuo. The residue was subjected to silica gel chromatography (24 g RediSep Gold column) using 0-60 % ethyl acetate in hexanes over 20 CV, then at 60 % ethyl acetate for 10 CV. Fractions containing the pure product were pooled and then concentrated in vacuoto give N-(l-((6P)-3-(4-chloro-l-methyl-3-(methylsulfonamido)-lH-indazol-7-yl)-4-oxo-7-(3,3,3-trifluoropropoxy)-3,4-dihydropyrido[2,3-d]pyrimidin-2-yl)-2-(3,5-difluorophenyl)ethyl)-2-((3bS,4aR)-3-(difluoromethyl)-5,5-difluoro-3b,4,4a,5-tetrahydro-lH-cyclopropa[3,4]cyclopenta[l,2-c]pyrazol-l-yl)acetamide (0.078 g, 0.081 mmol, 38.0 % yield) as a brown solid. *H NMR (500 MHz, METHANOL-d^ d ppm 8.46 – 8.53 (m, 1 H) 7.28 – 7.34 (m, 1 H) 7.19 – 7.24 (m, 1 H) 7.03 – 7.09 (m, 1 H) 6.53 – 6.81 (m, 4 H) 4.80 (dd, J=5.96, 2.98Hz, 3 H) 4.49 – 4.62 (m, 2 H) 3.58 – 3.62 (m, 3 H) 3.40 – 3.49 (m, 1 H) 3.22 – 3.24 (m, 3 H) 3.06 – 3.14 (m, 1 H) 2.80 – 2.89 (m, 2 H) 2.37 – 2.44 (m, 2 H) 1.32 – 1.37 (m, 1 H) 0.96 – 1.01 (m, 1 H). LCMS Analysis Method: Column = Acquity UPLC BEH C18, 2.1 x 100 mm, 1.7 pm particles; Injection Volume = 5.00 pL; Flowrate = 0.80 mL/min; Solvent A = 95:5
WatenMeCN w/ 0.1% v/v formic acid; Solvent B = 5:95 WatenMeCN w/ 0.1% v/v formic acid;
Elution profile = Start %B: 0, End %B: 100, Gradient Time: 3.5 min. then hold at 100% B for 1 min.; Detection wavelength 1 = 220 nm, wavelength 2 = 254 nm. LCMS retention time = 3.097 min; m/z = 918.05 [M+l]+.



PAT
- Pyrido[2,3-d]pyrimidine derivatives as inhibitors of human immunodeficiency virus replicationPublication Number: US-2021323967-A1Priority Date: 2019-06-19
- Pyrido[2,3-d]pyrimidine derivatives as inhibitors of human immunodeficiency virus replicationPublication Number: US-2025019383-A1Priority Date: 2019-06-19
- Pyrido[2,3-D]pyrimidine derivatives as inhibitors of human immunodeficiency virus replicationPublication Number: KR-20220024608-APriority Date: 2019-06-19
- Pyrido[2,3-d]pyrimidine derivatives as inhibitors of human immunodeficiency virus replicationPublication Number: EP-3986561-A1Priority Date: 2019-06-19
- Pyrido[2,3-d]pyrimidine derivatives as inhibitors of human immunodeficiency virus replicationPublication Number: EP-3986561-B1Priority Date: 2019-06-19Grant Date: 2024-02-14
- Pyrido [2,3-d]pyrimidine derivatives as inhibitors of human immunodeficiency virus replicationPublication Number: US-12129255-B2Priority Date: 2019-06-19Grant Date: 2024-10-29
- Pyrido[2,3-d]pyrimidine derivatives as inhibitors of human immunodeficiency virus replicationPublication Number: WO-2020254985-A1Priority Date: 2019-06-19
- Inhibitors of human immunodeficiency virus replicationPublication Number: EP-4415685-A1Priority Date: 2021-10-13
- Inhibitors of human immunodeficiency virus replicationPublication Number: WO-2023062559-A1Priority Date: 2021-10-13
- Inhibitors of human immunodeficiency virus replicationPublication Number: US-2024423985-A1Priority Date: 2021-10-13
- Inhibitors of human immunodeficiency virus replicationPublication Number: US-2023149408-A1Priority Date: 2020-04-15
- Pharmaceutical compositions comprising cabotegravirPublication Number: US-2023045509-A1Priority Date: 2019-12-09
ADVERTISEMENT
BLUE JET HEALTHCARE LTD, https://bluejethealthcare.com
Looking for a Reliable SNAC Manufacturer? Let’s Talk.
At Blue Jet Healthcare Ltd, we specialize in the scalable, high-purity production of SNAC—a critical excipient powering the next generation of oral peptide therapeutics.
With increasing demand for SNAC across global pharma pipelines, choosing the right manufacturing partner is essential. Quality, timelines, and consistency matter.

Phone No. +91 (22) 22075307 / +91 (22) 22071691
Business Development/ Contract Manufacturing: marketing1@bluejethealthcare.com, madhu.gautam71@gmail.com

AS ON OCT2025 4.511 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
……
ADVERTISEMENT
ANAX LABORATORIES
WEBSITE https://www.anaxlab.com/
Discovery Solutions, Supporting the chemistry needs of clients in the Medical, Analytical and Bio Sciences
Development Solutions, Developing from Lab scale to PR&D, Kilo Scale-ups and Commercial Scales
SEE MORE………Integrated Solutions, Manufacturing Solutions, Products,
Can’t Find? Let’s Connect

Phone : +91 897704 2010 / +91 9177075735, Email : info@anaxlab.com
NEXT
ADVERTISEMENT
Advect Process Systems Ltd.
ADVECT PROCESS SYSTEMS CANADA LTD
51 Beechwood Rd., Cambridge, ON Canada N1S 3S1
Call Now +1 306 850 6737, Mail Now, ask@advectprocess.com
ADVERTISEMENT
BLUE JET HEALTHCARE LTD, https://bluejethealthcare.com
Looking for a Reliable SNAC Manufacturer? Let’s Talk.
At Blue Jet Healthcare Ltd, we specialize in the scalable, high-purity production of SNAC—a critical excipient powering the next generation of oral peptide therapeutics.
With increasing demand for SNAC across global pharma pipelines, choosing the right manufacturing partner is essential. Quality, timelines, and consistency matter.

Phone No. +91 (22) 22075307 / +91 (22) 22071691
Business Development/ Contract Manufacturing: marketing1@bluejethealthcare.com, madhu.gautam71@gmail.com
//////////dezecapavir, inhibitor of viral replication, antiviral, SEK9LN2LSM, VH 4011499, VH4011499, VH-4011499, VH 499, GSK2838232, GSK 2838232
Limnetrelvir



Limnetrelvir
CAS 2923500-04-1
MF C27H23F4N5O4 MW 557.50
N-[(3R)-1-[4-cyano-2-(morpholine-4-carbonyl)-6-(trifluoromethyl)phenyl]pyrrolidin-3-yl]-8-fluoro-2-oxo-1H-quinoline-4-carboxamide
N-{(3R)-1-[4-cyano-2-(morpholine-4-carbonyl)-6-
(trifluoromethyl)phenyl]pyrrolidin-3-yl}-8-fluoro-2-oxo1,2-dihydroquinoline-4-carboxamide
antiviral, ABBV-903, ABBV 903, 4TPS988XGG
Limnetrelvir (ABBV-903) is a MPro inhibitor. Limnetrelvir could be used in antiviral research.
SYN

Example 1 – Synthesis of Compound (2) (R)-N-(1-(4-cyano-2-(morpholine-4-carbonyl)-6-(trifluoromethyl)phenyl)pyrrolidin-3-yl)-8-fluoro-2-oxo-1,2-dihydroquinoline-4-carboxamide

Compound 2F – Synthesis of 8-fluoro-2-oxo-1,2-dihydroquinoline-4-carboxylic acid

[00035] A suspension of 7-fluoroindoline-2,3-dione (55 g, 333 mmol), malonic acid (41.6 g, 400 mmol) and sodium acetate (68.3 g, 833 mmol) in acetic acid (500 mL) was heated at 112 °C overnight. The reaction mixture was cooled to room temperature and poured into cold 0.4 M aqueous HCl (2200 mL). The precipitate was collected by filtration and rinsed thoroughly with ice-cold water (~250 mL) followed by methyl tert-butyl ether (~100 mL) and then concentrated twice from acetonitrile with high vacuum. The materials were largely dissolved into 1 M aqueous NaOH (370 mL) and filtered through diatomaceous earth with a 0.1 M aqueous NaOH (50 mL) rinse. Then the filtrate was washed thrice with dichloromethane (3 x 200 mL) which removed the color. After this aqueous layer was filtered again through diatomaceous earth, it was acidified by the dropwise addition of concentrated aqueous HCl (33 mL, ~0.4 moles). The material was collected by filtration. After prolonged drying under heat and vacuum, the material was treated with water (1 L) and the mixture was made acidic by the addition of a small amount of 1 M aqueous HCl. The suspension was heated to 80 °C and then allowed to slowly cool to room temperature. The resulting material was collected by filtration, washed with 0.01 M aqueous HCl (150 mL) and dried under vacuum at 80 °C to provide the title compound (2F).1H NMR (500 MHz, DMSO-d6) δ ppm 14.00 (bs, 1H), 12.07 (bs, 1H), 8.00 (dd, J = 8.2, 1.2 Hz, 1H), 7.49 (ddd, J = 11.0, 8.1, 1.2 Hz, 1H), 7.23 (ddd, J = 8.2, 8.1, 5.2 Hz, 1H), 6.95 (s, 1H); 13C NMR (101 MHz, DMSO-d6, 90 °C) δ ppm 165.75 – 165.73 (m), 160.30, 148.75 (d, J = 246.0 Hz), 140.85 – 140.80 (m), 128.11 (d, J = 13.7 Hz), 123.85, 121.60 – 121.53 (m), 121.53 – 121.43 (m), 117.70 – 117.65 (m), 115.33 (d, J = 17.2 Hz); 19F NMR (376 MHz, DMSO-d6, 90 °C) δ ppm -130.47 (dd, J = 10.9, 5.3 Hz); MS (APCI, M+H+) m/z 208.
Compound 2G – Synthesis of (R)-N-(1-(4-cyano-2-(morpholine-4-carbonyl)-6-(trifluoromethyl)phenyl)pyrrolidin-3-yl)-8-fluoro-2-oxo-1,2-dihydroquinoline-4-carboxamide (2)

00036] To a mixture of Compound 2F (29.84 g, 144 mmol) in anhydrous N,N-dimethylformamide (360 mL) was added DMTMM (4-(4,6-dimethoxy-1,3,5-triazin-2-yl)-4-
methylmorpholinium chloride) (43.17 g, 156 mmol) over twelve minutes at room temperature. After the suspension had been stirred forty minutes, it was added over eight minutes to a suspension of Compound 2E (≤120 mmol) and N-methylmorpholine (16 mL, 146 mmol) in N,N-dimethylformamide (120 mL) with a N,N-dimethylformamide (20 mL) rinse. After forty minutes, the reaction mixture was added to rapidly stirred 0.1 M aqueous K2HPO4 (2.5 L) and extracted four times with 4:1 isopropyl acetate / heptanes then once with isopropyl acetate alone. The product, which had begun to precipitate out from the combined extracts, was separated by decantation and filtration, then washed with dichloromethane. The remaining aqueous phase was extracted twice more with isopropyl acetate and all the organic extracts were combined, then washed with additional 0.1 M aqueous K2HPO4 followed by water, dried (Na2SO4), and filtered. The filtrate was concentrated with the dichloromethane wash of the material collected above. The residue was concentrated, dissolved in acetonitrile / CH2Cl2, filtered, and purified by chromatography on silica (20 to 100% acetonitrile / CH2Cl2). The collected fractions were concentrated to a small volume, and stirred in ethyl acetate overnight.
[00037] The suspension was heated at 70 °C for twenty minutes, then allowed to slowly cool to room temperature. Methyl tert-butyl ether was stirred in, the suspension was cooled to 0 °C, and the purified product was collected by filtration with rinses of 1:1 ethyl acetate / methyl tert-butyl ether followed by methyl tert-butyl ether before being dried under vacuum with heat. The material obtained previously from the early extracts were also stirred in ethyl acetate, heated at 70 °C, then allowed to slowly cool to room temperature. Methyl tert-butyl ether was stirred in, the suspension was cooled to 0 °C, and the purified product was collected by filtration with rinses of 1:1 ethyl acetate / methyl tert-butyl ether rinse followed by methyl tert-butyl ether. The material was dried overnight under vacuum to provide the title compound (2).1H NMR (500 MHz, DMSO-d6) δ ppm 11.96 (s, 1H), 9.03 – 8.84 (m, 1H), 8.21 – 8.18 (m, 1H), 7.98 – 7.93 (m, 1H), 7.56 – 7.50 (m, 1H), 7.49 – 7.43 (m, 1H), 7.21 – 7.15 (m, 1H), 6.66 – 6.59 (m, 1H), 4.51 – 4.40 (m, 1H), 3.73 – 3.55 (m, 6H), 3.54 – 3.22 (m, 6H), 2.29 – 2.18 (m, 1H), 2.07 – 1.95 (m, 1H); 1H NMR (400 MHz, DMSO-d6, 90 °C) δ ppm 11.47 (bs, 1H), 8.77 – 8.47 (m, 1H), 8.09 (d, J = 2.1 Hz, 1H), 7.88 (d, J = 2.1 Hz, 1H), 7.54 (dd, J = 8.1, 1.2 Hz, 1H), 7.39 (ddd, J = 11.0, 8.1, 1.2 Hz, 1H), 7.15 (ddd, J = 8.1, 8.1, 5.1 Hz, 1H), 6.60 (s, 1H), 4.54 – 4.43 (m, 1H), 3.74 – 3.20 (m, 12H), 2.31 – 2.21 (m, 1H), 2.06 – 1.96 (m, 1H); 13C NMR (101 MHz, DMSO-d6, 90 °C) δ
ppm 166.61, 165.97, 161.31, 149.59 (d, J = 246.3 Hz), 148.95, 146.10 – 146.03 (m), 136.00, 135.65, 133.13 (q, J = 6.1 Hz), 128.84 – 128.63 (m), 123.76 (q, J = 273.7 Hz), 122.19, 122.16, 122.12, 121.60, 118.99 – 118.91 (m), 117.75, 116.17 (d, J = 17.3 Hz), 105.57, 66.04, 57.95, 51.06, 50.35, 47.74, 42.35, 31.54; 19F NMR (376 MHz, DMSO-d6) δ ppm -57.54 – -58.10 (m), -130.02 – -130.15 (m); 19F NMR (376 MHz, DMSO-d6, 90 °C) δ ppm -58.37 – -58.97 (m), -130.96 (dd, J = 11.0, 5.1 Hz). MS (APCI, M+H+) m/z 558.






PAT
- Pyrrolidine Main Protease Inhibitors as Antiviral AgentsPublication Number: US-2024158368-A1Priority Date: 2022-10-14
- Pyrrolidine main protease inhibitors as antiviral agentsPublication Number: WO-2024081351-A1Priority Date: 2022-10-14
AS ON OCT2025 4.511 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
……
/////////limnetrelvir, antiviral, ABBV-903, ABBV 903, 4TPS988XGG
Iscartrelvir



Iscartrelvir
CAS 2921711-74-0
MF 2921711-74-0, 526.4 g/mol
N-{(1S,2R)-2-[4-bromo-2-(methylcarbamoyl)-6-nitroanilino]cyclohexyl}isoquinoline-4-carboxamide
antiviral, WU-04, WU 04, W2LTV65R5E
Iscartrelvir is an investigational new drug developed by the Westlake University for the treatment of COVID-19. It targets the SARS-CoV-2 3CL protease, which is crucial for the replication of the virus responsible for COVID-19.[1][2]
Iscartrelvir is a small molecule drug. The usage of the INN stem ‘-trelvir’ in the name indicates that Iscartrelvir is a antiviral 3CL protease inhibitor. Iscartrelvir has a monoisotopic molecular weight of 525.1 Da.
PAT
WO2022150962A1
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2022150962&_cid=P11-MJKTXT-76321-1

SYN
https://patentscope.wipo.int/search/en/detail.jsf?docId=CN331401594&_cid=P11-MJKTO7-65334-1
PAT
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2024243841&_cid=P11-MJKTO7-65334-1
N-((1S,2R)-2-((4-bromo-2-(methylcarbamoyl)-6-nitrophenyl)amino)cyclohexyl)isoquinoline-4-carboxamide, and its structure is as follows:

Example 1: Preparation of Compound 1
[0189]A free, amorphous compound 1, a yellow solid, was prepared according to the method disclosed in paragraphs [00121]-[00128] of WO2022150962A1, and was used in the following examples. The specific synthetic steps are shown in steps a to d:

The reagents and conditions for steps a to d are further described below: (a) 1-[bis(dimethylamino)methylene]-1H-1,2,3-triazolo[4,5-b]pyridinium 3-oxide hexafluorophosphate (HATU), N,N-diisopropylethylamine (DIPEA), CH₂Cl₂
or
dichloromethane (DCM), 0°C, 2 h; (b) DIPEA, dimethylformamide (DMF), 80°C, 16 h; (c) 3M ethyl hydrochloride (HCl·EA), CH₂Cl₂ , 1
h ; (d ) HATU, DIPEA, DMF, room temperature, 12 h.
[0191]Step a: Synthesis of N-methyl-5-bromo-2-fluoro-3-nitrobenzamide (I-1)
[0192]A solution of 5-bromo-2-fluoro-3-nitrobenzoic acid (0.8 g, 3.80 mmol) in dichloromethane (20 mL) was stirred at 0 °C. Then, HATU (2.0 g, 5.25 mmol), DIPEA (1.88 mL, 11.4 mmol), and methylamine hydrochloride (0.31 g, 4.5 mmol) were added to the reaction mixture. The mixture was stirred at 0 °C for 2 hours until it became clear. The mixture was extracted three times with dichloromethane, and the combined organic layers were washed with a saturated brine solution. The organic phase was then dried over anhydrous Na₂SO₄ and concentrated
under vacuum. Finally, the mixture was purified by chromatography to give compound I-1 (0.8 g, 76% yield) as a yellow solid.
[0193]Step b: Synthesis of tert-butyl 2-((4-bromo-2-(methylcarbamoyl)-6-nitrophenyl)amino)cyclohexyl)carbamate (I-2)
[0194]A solution of compound I-1 (0.8 g, 2.9 mmol) in 15 mL of DMF was stirred at room temperature. Then, tert-butyl ((1S,2R)-2-aminocyclohexyl)carbamate (0.75 g, 3.5 mmol) (the corresponding stereoisomer of this reagent can be used to synthesize the stereoisomer of compound I-2) and DIPEA (1.44 mL, 8.7 mmol) were added to the reaction mixture. The mixture was heated to 80 °C and stirred for 16 hours. The mixture was extracted three times with ethyl acetate, and the combined organic layers were washed with saturated salt solution. The organic phase was then dried over anhydrous Na₂SO₄ and concentrated under vacuum to give compound
I -2 as a yellow solid, requiring no further purification.

Step c: Synthesis of 2-(2-aminocyclohexyl)amino)-5-bromo-N-methyl-3-nitrobenzamide hydrochloride (I-3)
[0196]A solution of compound I-2 (90 mg, 0.19 mmol) (or the corresponding stereoisomer) in anhydrous dichloromethane (6 mL) was stirred at room temperature. Then, HCl (4 mL, 3 M in ethyl acetate) was added. The mixture was stirred at room temperature for 2 hours. The mixture was concentrated under vacuum to give compound I-3 as a yellow solid, requiring no further purification.
[0197]Step d: Synthesis of N-((1S,2R)-2-((4-bromo-2-(methylcarbamoyl)-6-nitrophenyl)amino)cyclohexyl)isoquinoline-4-carboxamide
[0198]At room temperature, a solution of the corresponding isoquinoline-4-carboxylic acid (1 equivalent) and HATU (1.5 equivalent) in anhydrous DMF (6 mL) was stirred. Then, compound I-3 and DIPEA (5.0 equivalent) were added. The mixture was stirred overnight at room temperature. The mixture was extracted three times with ethyl acetate, and the combined organic layers were washed with saturated brine. The organic phase was then dried over anhydrous Na₂SO₄ and
concentrated under vacuum. Finally, the mixture was purified by chromatography to give compound 1 as a free amorphous solid in yellow form.
PAT
- Aromatic ring-containing pyridone amide compoundsPublication Number: CN-119100980-APriority Date: 2023-06-07
- Crystal of viral protease inhibitor and usePublication Number: WO-2024243841-A1Priority Date: 2023-05-31
- Protease inhibitors, their preparation and usePublication Number: CN-113072497-BPriority Date: 2021-01-12Grant Date: 2023-04-14
- Protease inhibitors, their preparation and usePublication Number: CN-113072497-APriority Date: 2021-01-12
- Protease inhibitors, their preparation and usePublication Number: CN-116751164-APriority Date: 2021-01-12
AS ON OCT2025 4.511 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
……
| Clinical data | |
|---|---|
| Other names | WPV01; WU-04 |
| Identifiers | |
| IUPAC name | |
| CAS Number | 2921711-74-0 |
| PubChem CID | 156774920 |
| ChemSpider | 129307041 |
| UNII | W2LTV65R5E |
| PDB ligand | J7R (PDBe, RCSB PDB) |
| Chemical and physical data | |
| Formula | C24H24BrN5O4 |
| Molar mass | 526.391 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| SMILES | |
| InChI | |
References
- Yang L, Wang Z (September 2023). “Bench-to-bedside: Innovation of small molecule anti-SARS-CoV-2 drugs in China”. European Journal of Medicinal Chemistry. 257 115503. doi:10.1016/j.ejmech.2023.115503. PMC 10193775. PMID 37229831.
- Hou N, Shuai L, Zhang L, Xie X, Tang K, Zhu Y, et al. (February 2023). “Development of Highly Potent Noncovalent Inhibitors of SARS-CoV-2 3CLpro”. ACS Central Science. 9 (2): 217–227. doi:10.1021/acscentsci.2c01359. PMC 9885526. PMID 36844503.
- Resistance mechanisms of SARS-CoV-2 3CLpro to the non-covalent inhibitor WU-04Publication Name: Cell DiscoveryPublication Date: 2024-04-09PMCID: PMC11003996PMID: 38594245DOI: 10.1038/s41421-024-00673-0
- Identification of Ebselen derivatives as novel SARS-CoV-2 main protease inhibitors: Design, synthesis, biological evaluation, and structure-activity relationships explorationPublication Name: Bioorganic & Medicinal ChemistryPublication Date: 2023-12-15PMID: 37972434DOI: 10.1016/j.bmc.2023.117531
- The molecular mechanism of non-covalent inhibitor WU-04 targeting SARS-CoV-2 3CLpro and computational evaluation of its effectiveness against mainstream coronavirusesPublication Name: Physical chemistry chemical physics : PCCPPublication Date: 2023-09-13PMID: 37655706DOI: 10.1039/d3cp03828a
- Bench-to-bedside: Innovation of small molecule anti-SARS-CoV-2 drugs in ChinaPublication Name: European Journal of Medicinal ChemistryPublication Date: 2023-09-05PMCID: PMC10193775PMID: 37229831DOI: 10.1016/j.ejmech.2023.115503
- Development of Highly Potent Noncovalent Inhibitors of SARS-CoV-2 3CLproPublication Name: ACS Central SciencePublication Date: 2023-01-25PMCID: PMC9885526PMID: 36844503DOI: 10.1021/acscentsci.2c01359
////////iscartrelvir, antiviral, WU-04, WU 04, W2LTV65R5E
Odentegravir
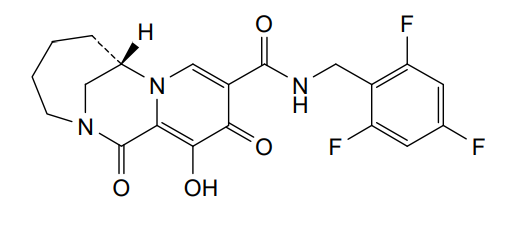

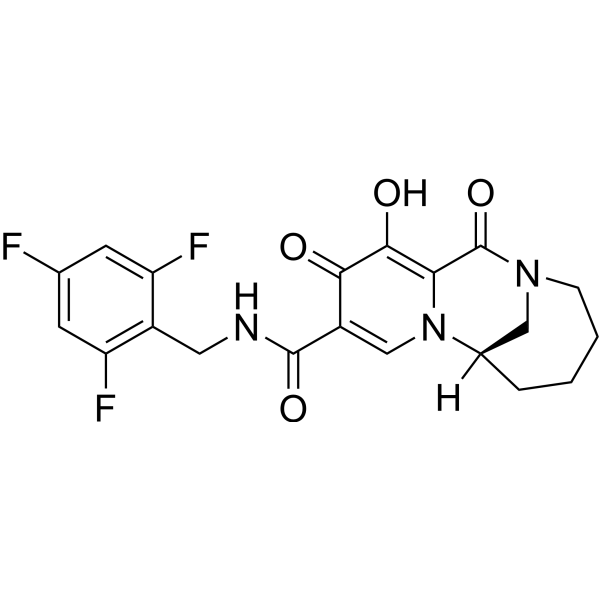
Odentegravir
CAS 2495436-99-0
MF C20H18F3N3O4 MW421.4 g/mol
(7S)-12-hydroxy-1,11-dioxo-N-[(2,4,6-trifluorophenyl)methyl]-1,4,5,6,7,11-hexahydro-3H-2,7-
methanopyrido [1,2-a][1,4]diazonine-10-carboxamide
(7S)-1,4,5,6,7,11-HEXAHYDRO-12-HYDROXY-1,11-DIOXO-N-((2,4,6-TRIFLUOROPHENYL)METHYL)-3H-2,7-METHANOPYRIDO(1,2-A)(1,4)DIAZONINE-10-CARBOXAMIDE
(7S)-12-HYDROXY-1,11-DIOXO-N-((2,4,6-TRIFLUOROPHENYL)METHYL)-1,4,5,6,7,11-HEXAHYDRO-3H-2,7-METHANOPYRIDO(1,2-A)(1,4)DIAZONINE-10-CARBOXAMIDE
3H-2,7-METHANOPYRIDO(1,2-A)(1,4)DIAZONINE-10-CARBOXAMIDE, 1,4,5,6,7,11-HEXAHYDRO-12-HYDROXY-1,11-DIOXO-N-((2,4,6-TRIFLUOROPHENYL)METHYL)-, (7S)-
antiviral, H8B26JZ4A4, orb2664247
Odentegravir is a small molecule drug classified as a
HIV integrase inhibitor, indicated by the “-tegravir” stem in its name. It is a chemical compound with the molecular formula
has been used in research for its antiviral properties.
- Drug Class: HIV integrase inhibitor
- Chemical Formula:
C20H18F3N3O4cap C sub 20 cap H sub 18 cap F sub 3 cap N sub 3 cap O sub 4𝐶20𝐻18𝐹3𝑁3𝑂4
- Molecular Weight:
421.12421.12421.12 Da (monoisotopic)
- Classification: Small molecule drug
SYN
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2020197991&_cid=P12-MHY8KB-06018-1
Example 23: Preparation of racemic-12-hydroxy-1,11-dioxo-N-(2,4,6-trifluorobenzyl)-1,4,5,6,7,11-hexahydro-3H-2,7-methanopyrido[1,2-a][1,4]diazonine-10-carboxamide (26), (7R)-12-hydroxy-1,11-dioxo-N-(2,4,6-trifluorobenzyl)-1,4,5,6,7,11-hexahydro-3H-2,7-
methanopyrido[1,2-a][1,4]diazonine-10-carboxamide (26-1) and (7S)-12-hydroxy-1,11-dioxo-N-(2,4,6-trifluorobenzyl)-1,4,5,6,7,11-hexahydro-3H-2,7-methanopyrido[1,2-a][1,4]diazonine-10-carboxamide (26-2):

Synthesis of 12-Hydroxy-1,11-dioxo-N-(2,4,6-trifluorobenzyl)-1,4,5,6,7,11-hexahydro-3H-2,7-methanopyrido[1,2-a][1,4]diazonine-10-carboxamide (26):
[0335] 12-(Benzyloxy)-1,11-dioxo-1,4,5,6,7,11-hexahydro-3H-2,7-methanopyrido[1,2-a][1,4]diazonine-10-carboxylic acid (57 mg, 0.155 mmol) was dissolved in DCM (2 mL) with (2,4,6-trifluorophenyl)methanamine (27 mg, 0.17 mmol) and triethylamine (60 mg, 0.464 mmol). HATU (60 mg, 0.186 mmol) was added and the mixture was stirred at room
temperature. After overnight reaction, the reaction was concentrated to dryness, purified by silicon gel chromatography to obtain compound 12-(benzyloxy)-1,11-dioxo-N-(2,4,6-trifluorobenzyl)-1,4,5,6,7,11-hexahydro-3H-2,7-methanopyrido[1,2-a][1,4]diazonine-10-carboxamide (26a) MS (m/z) 512.06 [M+H]+.
[0336] Compound 12-(benzyloxy)-1,11-dioxo-N-(2,4,6-trifluorobenzyl)-1,4,5,6,7,11-hexahydro-3H-2,7-methanopyrido[1,2-a][1,4]diazonine-10-carboxamide (26a) (7 mg, 0.014 mmol) was dissloved in Tolune (1 mL), then followed by the addition of TFA (1 mL). The resulting mixture was stirred at rt for overnight. The solvent was removed under vacuo an the residue was purifed by HPLC to obtain the title compound (26). MS (m/z) 422.091 [M+H]+.1H NMR (400 MHz, DMSO-d6) d 10.39 (t, J = 5.8 Hz, 1H), 8.45 (s, 1H), 7.24 – 7.11 (m, 2H), 4.72 (dd, J = 5.9, 2.9 Hz, 1H), 4.54 (dd, J = 6.0, 2.4 Hz, 2H), 4.11 (d, J = 13.3 Hz, 1H), 3.88 – 3.79 (m, 1H), 3.64 (dd, J = 14.7, 1.9 Hz, 1H), 3.05 (dq, J = 9.5, 3.4 Hz, 1H), 2.06 – 1.91 (m, 1H), 1.89 – 1.74 (m, 3H), 1.61 (d, J = 7.7 Hz, 1H), 1.11 (d, J = 12.7 Hz, 1H).
Synthesis of (7S)-12-hydroxy-1,11-dioxo-N-(2,4,6-trifluorobenzyl)-1,4,5,6,7,11-hexahydro-3H-2,7-methanopyrido[1,2-a][1,4]diazonine-10-carboxamide (26-2) and (7R)-12-hydroxy-1,11-dioxo-N-(2,4,6-trifluorobenzyl)-1,4,5,6,7,11-hexahydro-3H-2,7-methanopyrido[1,2-a][1,4]diazonine-10-carboxamide (26-1):
[0337] Racemic 12-(benzyloxy)-1,11-dioxo-N-(2,4,6-trifluorobenzyl)-1,4,5,6,7,11-hexahydro-3H-2,7-methanopyrido[1,2-a][1,4]diazonine-10-carboxamide (26a) was separated by chiral HPLC separation (SFC chromatography on an IB 4.6X100mm 5mic column using MeOH(20) as co-solvent) to obtain compounds (7R)-12-(Benzyloxy)-1,11-dioxo-N-(2,4,6-trifluorobenzyl)-1,4,5,6,7,11-hexahydro-3H-2,7-methanopyrido[1,2-a][1,4]diazonine-10-carboxamide (26a-1) and (7S)-12-(benzyloxy)-1,11-dioxo-N-(2,4,6-trifluorobenzyl)-1,4,5,6,7,11-hexahydro-3H-2,7-methanopyrido[1,2-a][1,4]diazonine-10-carboxamide (26a-2)
[0338] Compound (7S)-12-(benzyloxy)-1,11-dioxo-N-(2,4,6-trifluorobenzyl)-1,4,5,6,7,11-hexahydro-3H-2,7-methanopyrido[1,2-a][1,4]diazonine-10-carboxamide (26a-2) (20 mg, 0.039 mmol) was dissloved in Tolune (1 mL), then followed by the addition of TFA (1 mL). The resulting mixture was stireed at rt for overnight. The solvent was removed under vacuo an the residue was purifed by HPLC to obtain the title compound (26-2). (MS (m/z) 422.123 [M+H]+. 1H NMR (400 MHz, DMSO-d6) d 10.59 (s, 1H), 10.39 (d, J = 5.9 Hz, 1H), 8.45 (s, 1H), 7.18 (t, J = 8.6 Hz, 2H), 4.72 (s, 1H), 4.59 – 4.48 (m, 2H), 4.11 (d, J = 13.2 Hz, 1H), 3.85 (d, J = 14.6 Hz, 1H), 3.69 – 3.59 (m, 1H), 3.05 (ddd, J = 11.3, 6.7, 3.6 Hz, 1H), 1.97 (m, 1H), 1.87 – 1.71 (m, 3H), 1.67 – 1.55 (m, 1H), 1.10 (m, 1H).
[0339] Compound (7R)-12-(benzyloxy)-1,11-dioxo-N-(2,4,6-trifluorobenzyl)-1,4,5,6,7,11-hexahydro-3H-2,7-methanopyrido[1,2-a][1,4]diazonine-10-carboxamide (26a-1) ((20 mg, 0.039 mmol) was dissloved in Tolune (1 mL), then followed by the addition of TFA (1 mL). The resulting mixture was stireed at rt for overnight. The solvent was removed under vacuo an the residue was purifed by HPLC to obtain the title compound (26-1). MS (m/z) 422.116 [M+H]+. 1H NMR (400 MHz, DMSO-d6) d 10.58 (s, 1H), 10.39 (t, J = 5.8 Hz, 1H), 8.45 (s, 1H), 7.18 (dd, J = 9.2, 8.0 Hz, 2H), 4.73 (s, 1H), 4.58 – 4.49 (m, 2H), 4.11 (d, J = 13.3 Hz, 1H), 3.85 (d, J = 14.6 Hz, 1H), 3.65 (d, J = 14.2 Hz, 1H), 3.10 – 3.00 (m, 1H), 1.96 (m, 1H), 1.82 (d, J = 12.2 Hz, 3H), 1.61 (d, J = 7.4 Hz, 1H), 1.18 – 1.05 (m, 1H).
SYN
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2023196875&_cid=P12-MHY8FJ-02517-1
PAT
- Bridged tricyclic carbamoylpyridone compounds and their pharmaceutical usesPublication Number: JP-2025013503-APriority Date: 2019-03-22
- Bridged tricyclic carbamoylpyridone compounds and their pharmaceutical usesPublication Number: KR-102714084-B1Priority Date: 2019-03-22Grant Date: 2024-10-08
- Bridged tricyclic carbamoylpyridone compounds and their pharmaceutical usePublication Number: KR-20240151256-APriority Date: 2019-03-22
- Bridged Tricyclic Carbamoylpyridone Compounds and Their Pharmaceutical UsePublication Number: ES-2927041-T3Priority Date: 2019-03-22Grant Date: 2022-11-03
- Bridged tricyclic carbamoylpyridone compounds and their pharmaceutical usePublication Number: US-11548902-B1Priority Date: 2019-03-22Grant Date: 2023-01-10
- Bridged tricyclic carbamoylpyridone compounds and their pharmaceutical usePublication Number: US-2023027019-A1Priority Date: 2019-03-22
- Bridged tricyclic carbamoylpyridone compounds and their pharmaceutical usePublication Number: AU-2020245350-B2Priority Date: 2019-03-22Grant Date: 2023-04-20
- Bridged tricyclic carbamoylpyridone compounds and their pharmaceutical usePublication Number: US-2023203061-A1Priority Date: 2019-03-22
- Bridged tricyclic carbamoylpyridone compounds and their pharmaceutical usePublication Number: US-11084832-B2Priority Date: 2019-03-22Grant Date: 2021-08-10
- Bridged tricyclic carbamoylpyridone compounds and their pharmaceutical usePublication Number: AU-2020245350-A1Priority Date: 2019-03-22
- Bridged tricyclic carbamoylpyridone compounds and their pharmaceutical usePublication Number: EP-3938047-A1Priority Date: 2019-03-22
- Bridged tricyclic carbamoylpyridone compounds and their pharmaceutical usePublication Number: EP-3938047-B1Priority Date: 2019-03-22Grant Date: 2022-06-22
- Bridged tricyclic carbamoylpyridone compounds and their pharmaceutical usePublication Number: EP-4122537-A1Priority Date: 2019-03-22
- Bridged tricyclic carbamoylpyridone compounds and uses thereofPublication Number: US-2023339971-A1Priority Date: 2022-04-06
- Bridged tricyclic carbamoylpyridone compounds and uses thereofPublication Number: US-2023339972-A1Priority Date: 2022-04-06
- Bridged tricyclic carbamoylpyridone compounds and uses thereofPublication Number: WO-2023196875-A1Priority Date: 2022-04-06
- Bridged tricyclic carbamoylpyridone compounds and their pharmaceutical usePublication Number: US-2020317689-A1Priority Date: 2019-03-22
- Bridged tricyclic carbamoylpyridone compounds and their pharmaceutical usePublication Number: WO-2020197991-A1Priority Date: 2019-03-22
AS ON OCT2025 4.511 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
……
//////Odentegravir, antiviral, H8B26JZ4A4, orb2664247
Tixagevimab
| (Heavy chain) QMQLVQSGPE VKKPGTSVKV SCKASGFTFM SSAVQWVRQA RGQRLEWIGW IVIGSGNTNY AQKFQERVTI TRDMSTSTAY MELSSLRSED TAVYYCAAPY CSSISCNDGF DIWGQGTMVT VSSASTKGPS VFPLAPSSKS TSGGTAALGC LVKDYFPEPV TVSWNSGALT SGVHTFPAVL QSSGLYSLSS VVTVPSSSLG TQTYICNVNH KPSNTKVDKR VEPKSCDKTH TCPPCPAPEF EGGPSVFLFP PKPKDTLYIT REPEVTCVVV DVSHEDPEVK FNWYVDGVEV HNAKTKPREE QYNSTYRVVS VLTVLHQDWL NGKEYKCKVS NKALPASIEK TISKAKGQPR EPQVYTLPPS REEMTKNQVS LTCLVKGFYP SDIAVEWESN GQPENNYKTT PPVLDSDGSF FLYSKLTVDK SRWQQGNVFS CSVMHEALHN HYTQKSLSLS PGK (Light chain) EIVLTQSPGT LSLSPGERAT LSCRASQSVS SSYLAWYQQK PGQAPRLLIY GASSRATGIP DRFSGSGSGT DFTLTISRLE PEDFAVYYCQ HYGSSRGWTF GQGTKVEIKR TVAAPSVFIF PPSDEQLKSG TASVVCLLNN FYPREAKVQW KVDNALQSGN SQESVTEQDS KDSTYSLSST LTLSKADYEK HKVYACEVTH QGLSSPVTKS FNRGEC (Disulfide bridge: H22-H96, H101-H106, H150-H206, H216-L216, H232-H’232, H235-H’235, H267-H327, H373-H431, H’22-H’96, H’101-H’106, H’150-H’206, H’226-L’216, H’267-H’327, H’373-H’431, L23-L89, L136-L196, L’23-L’89, L’136-L’196) |
Tixagevimab
FDA 2021, 2021/12/8
ANTI VIRAL, CORONA VIRUS, PEPTIDE
Monoclonal antibody
Treatment and prevention of SARS-CoV-2 infection
| Formula | C6488H10034N1746O2038S50 |
|---|---|
| CAS | 2420564-02-7 |
| Mol weight | 146704.817 |
- 2196
- AZD-8895
- AZD8895
- COV2-2196
- Tixagevimab
- Tixagevimab [INN]
- UNII-F0LZ415Z3B
- WHO 11776
- OriginatorVanderbilt University
- DeveloperAstraZeneca; INSERM; National Institute of Allergy and Infectious Diseases
- ClassAntivirals; Monoclonal antibodies
- Mechanism of ActionVirus internalisation inhibitors
- RegisteredCOVID 2019 infections
- 24 Dec 2021Pharmacodynamics data from a preclinical trial in COVID-2019 infections released by AstraZeneca
- 16 Dec 2021Pharmacodynamics data from a preclinical trial in COVID-2019 infections released by AstraZeneca
- 10 Dec 2021Registered for COVID-2019 infections (In the elderly, Prevention, In adults) in USA (IM) – Emergency Use Authorization
Tixagevimab/cilgavimab is a combination of two human monoclonal antibodies, tixagevimab (AZD8895) and cilgavimab (AZD1061) targeted against the surface spike protein of SARS-CoV-2[4][5] used to prevent COVID-19. It is being developed by British-Swedish multinational pharmaceutical and biotechnology company AstraZeneca.[6][7] It is co-packaged and given as two separate consecutive intramuscular injections (one injection per monoclonal antibody, given in immediate succession).[2]
/////////////////////////////////////////////////////////////////////

AS ON DEC2021 3,491,869 VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE

join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@amcrasto
/////////////////////////////////////////////////////////////////////////////
Development
In 2020, researchers at Vanderbilt University Medical Center discovered particularly potent monoclonal antibodies, isolated from COVID-19 patients infected with a SARS-CoV-2 circulating at that time. Initially designated COV2-2196 and COV2-2130, antibody engineering was used to transfer their SARS-CoV-2 binding specificity to IgG scaffolds that would last longer in the body, and these engineered antibodies were named AZD8895 and AZD1061, respectively (and the combination was called AZD7442).[8]
To evaluate the antibodies’ potential as monoclonal antibody based prophylaxis (prevention), the ‘Provent’ clinical trial enrolled 5,000 high risk but not yet infected individuals and monitored them for 15 months.[9][10] The trial reported that those receiving the cocktail showed a 77% reduction in symptomatic COVID-19 and that there were no severe cases or deaths. AstraZeneca also found that the antibody cocktail “neutralizes recent emergent SARS-CoV-2 viral variants, including the Delta variant“.[7]
In contrast to pre-exposure prophylaxis, the Storm Chaser study of already-exposed people (post-exposure prophylaxis) did not meet its primary endpoint, which was prevention of symptomatic COVID-19 in people already exposed. AZD7442 was administered to 1,000 volunteers who had recently been exposed to COVID.[9]
Regulatory review
In October 2021, the Committee for Medicinal Products for Human Use (CHMP) of the European Medicines Agency (EMA) started a rolling review of tixagevimab/cilgavimab, which is being developed by AstraZeneca AB, for the prevention of COVID-19 in adults.[11]
Also in October 2021, AstraZeneca requested Emergency Use Authorization for tixagevimab/cilgavimab to prevent COVID-19 from the U.S. Food and Drug Administration (FDA).[12][13]
Emergency use authorization
On 14 November 2021, Bahrain granted emergency use authorization.[14]
On 8 December 2021, the U.S. Food and Drug Administration (FDA) granted emergency use authorization of this combination to prevent COVID-19 (before exposure) in people with weakened immunity or who cannot be fully vaccinated due to a history of severe reaction to coronavirus vaccines.[15] The FDA issued an emergency use authorization (EUA) for AstraZeneca’s Evusheld (tixagevimab co-packaged with cilgavimab and administered together) for the pre-exposure prophylaxis (prevention) of COVID-19 in certain people aged 12 years of age and older weighing at least 40 kilograms (88 lb).[2] The product is only authorized for those individuals who are not currently infected with the SARS-CoV-2 virus and who have not recently been exposed to an individual infected with SARS-CoV-2.[2]
References
- ^ “Evusheld- azd7442 kit”. DailyMed. Retrieved 4 January 2022.
- ^ Jump up to:a b c d “Coronavirus (COVID-19) Update: FDA Authorizes New Long-Acting Monoclonal Antibodies for Pre-exposure Prevention of COVID-19 in Certain Individuals”. U.S. Food and Drug Administration (FDA) (Press release). 8 December 2021. Retrieved 9 December 2021.
 This article incorporates text from this source, which is in the public domain.
This article incorporates text from this source, which is in the public domain. - ^ O’Shaughnessy, Jacqueline A. (20 December 2021). “Re: Emergency Use Authorization 104” (PDF). Food and Drug Administration. Letter to AstraZeneca Pharmaceuticals LP | Attention: Stacey Cromer Berman, PhD. Archived from the original on 29 December 2021. Retrieved 18 January 2022.
- ^ “IUPHAR/BPS Guide to PHARMACOLOGY”. IUPHAR. 27 December 2021. Retrieved 27 December 2021.
- ^ “IUPHAR/BPS Guide to PHARMACOLOGY”. IUPHAR. 27 December 2021. Retrieved 27 December 2021.
- ^ Ray, Siladitya (21 August 2021). “AstraZeneca’s Covid-19 Antibody Therapy Effective In Preventing Symptoms Among High-Risk Groups, Trial Finds”. Forbes. ISSN 0015-6914. Archived from the original on 21 August 2021. Retrieved 18 January 2022.
- ^ Jump up to:a b Goriainoff, Anthony O. (20 August 2021). “AstraZeneca Says AZD7442 Antibody Phase 3 Trial Met Primary Endpoint in Preventing Covid-19”. MarketWatch. Archived from the original on 21 August 2021. Retrieved 18 January 2022.
- ^ Dong J, Zost SJ, Greaney AJ, Starr TN, Dingens AS, Chen EC, et al. (October 2021). “Genetic and structural basis for SARS-CoV-2 variant neutralization by a two-antibody cocktail”. Nature Microbiology. 6 (10): 1233–1244. doi:10.1038/s41564-021-00972-2. ISSN 2058-5276. PMC 8543371. PMID 34548634.
- ^ Jump up to:a b Haridy, Rich (23 August 2021). “”Game-changing” antibody cocktail prevents COVID-19 in the chronically ill”. New Atlas. Retrieved 23 August 2021.
- ^ “AZD7442 PROVENT Phase III prophylaxis trial met primary endpoint in preventing COVID-19”. AstraZeneca (Press release). 20 August 2021. Retrieved 15 October 2021.
- ^ “EMA starts rolling review of Evusheld (tixagevimab and cilgavimab)”. European Medicines Agency. 14 October 2021. Retrieved 15 October 2021.
- ^ “AZD7442 request for Emergency Use Authorization for COVID-19 prophylaxis filed in US”. AstraZeneca US (Press release). 5 October 2021. Retrieved 15 October 2021.
- ^ “AZD7442 request for Emergency Use Authorization for COVID-19 prophylaxis filed in US”. AstraZeneca (Press release). 5 October 2021. Retrieved 15 October 2021.
- ^ Abd-Alaziz, Moaz; Elhamy, Ahmad (14 November 2021). Macfie, Nick (ed.). “Bahrain authorizes AstraZeneca’s anti-COVID drug for emergency use”. Reuters. Archived from the original on 23 November 2021. Retrieved 18 January 2022.
- ^ Mishra, Manas; Satija, Bhanvi (8 December 2021). Dasgupta, Shounak (ed.). “U.S. FDA authorizes use of AstraZeneca COVID-19 antibody cocktail”. Reuters. Archived from the original on 13 January 2022. Retrieved 18 January 2022.
External links
“Tixagevimab”. Drug Information Portal. U.S. National Library of Medicine.
- “Cilgavimab”. Drug Information Portal. U.S. National Library of Medicine.
- Clinical trial number NCT04625972 for “Phase III Double-blind, Placebo-controlled Study of AZD7442 for Post-exposure Prophylaxis of COVID-19 in Adults (STORM CHASER)” at ClinicalTrials.gov
- Clinical trial number NCT04625725 for “Phase III Double-blind, Placebo-controlled Study of AZD7442 for Pre-exposure Prophylaxis of COVID-19 in Adult. (PROVENT)” at ClinicalTrials.gov
| Tixagevimab (teal, right) and cilgavimab (purple, left) binding the spike protein RBD. From PDB: 7L7E. | |
| Combination of | |
|---|---|
| Tixagevimab | Monoclonal antibody |
| Cilgavimab | Monoclonal antibody |
| Clinical data | |
| Trade names | Evusheld |
| Other names | AZD7442 |
| License data | US DailyMed: Tixagevimab |
| Routes of administration | Intramuscular |
| ATC code | J06BD03 (WHO) |
| Legal status | |
| Legal status | US: ℞-only via emergency use authorization[1][2][3] |
| Identifiers | |
| KEGG | D12262 |
| Clinical data | |
|---|---|
| Drug class | Antiviral |
| ATC code | None |
| Identifiers | |
| CAS Number | 2420564-02-7 |
| DrugBank | DB16394 |
| UNII | F0LZ415Z3B |
| KEGG | D11993 |
| Chemical and physical data | |
| Formula | C6488H10034N1746O2038S50 |
| Molar mass | 146706.82 g·mol−1 |
| Clinical data | |
|---|---|
| Drug class | Antiviral |
| ATC code | None |
| Identifiers | |
| CAS Number | 2420563-99-9 |
| DrugBank | DB16393 |
| UNII | 1KUR4BN70F |
| KEGG | D11994 |
| Chemical and physical data | |
| Formula | C6626H10218N1750O2078S44 |
| Molar mass | 149053.44 g·mol−1 |
/////////////////Tixagevimab, ANTI VIRAL, CORONA VIRUS, PEPTIDE, Monoclonal antibody, SARS-CoV-2 , WHO 11776, 2196, AZD-8895, AZD 8895, COV2-2196, COVID 19
NEW DRUG APPROVALS
ONE TIME
$10.00

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}