
Home » Articles posted by DR ANTHONY MELVIN CRASTO Ph.D (Page 430)
Author Archives: DR ANTHONY MELVIN CRASTO Ph.D
 DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HERE
DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HEREFlag and hits
ORGANIC SPECTROSCOPY

SUBSCRIBE

 Subscribe in a reader
Subscribe in a reader
Enter your email address:
Delivered by FeedBurner
Subscribe to New Drug Approvals by Email![]()

![]()



![]()
![]()





Recent Comments
| shivkr2 on SPSR Excellence Award 2025 – S… | |
| Bonkasaurus on Infigratinib phosphate | |
| PALOVAROTENE | ORGAN… on Palovarotene | |
| Pfizer just purchase… on Temanogrel | |
| Pfizer To Cash In On… on Temanogrel |
ViiV Healthcare presents phase III SAILING study data of dolutegravir vs raltegravir in treatment-experienced adults with HIV-1

Dolutegravir
| Identifiers | |
|---|---|
| CAS number | 1051375-16-6 |
8 TH MATCH 2013
ViiV Healthcare, a global specialist HIV company established in November 2009 by GSK and Pfizer dedicated to delivering advances in treatment and care for people living with HIV, has announced 24-week data from the phase III SAILING (ING111762) study evaluating the investigational integrase inhibitor dolutegravir in patients with HIV-1 who are failing on current therapy, but had not been treated with an integrase inhibitor.
At 24 weeks, 79% of study participants receiving the once-daily dolutegravir regimen were virologically suppressed (HIV-1 RNA <50 c/mL) vs. 70% of participants on the twice-daily raltegravir regimen. This difference in response was statistically significant with a 95% confidence interval for the difference of 3.4% to 15.9% (p=0.003).
The SAILING study was designed to demonstrate non-inferiority of a regimen containing dolutegravir versus raltegravir (both with up to two background agents) and the analysis met this criterion; statistical superiority was concluded as part of a pre-specified testing procedure. These data were presented at the 20th Conference on Retroviruses and Opportunistic Infections (CROI) in Atlanta, Georgia.
Differences in treatment outcome in favour of the dolutegravir arm were driven by greater virologic response: at Week 24, 15% of patients receiving the dolutegravir regimen had virologic non-response vs. 24% of patients receiving the raltegravir regimen. In addition, fewer subjects failed therapy with integrase inhibitor resistance on dolutegravir (n=2) than on raltegravir (n=10, p=0.016).
Overall, the tolerability of dolutegravir (DTG) was similar to that of raltegravir (RAL). At 24 weeks, 2% of subjects on the dolutegravir regimen discontinued due to adverse events (AEs) vs. 4% of subjects on the raltegravir regimen. The rate of drug-related AEs was similar for both arms (DTG 20%, RAL 23%) and commonly reported AEs (defined as events that occurred in more than 10% of subjects) were similar on both arms, namely diarrhoea (20% DTG, 17% RAL) and upper respiratory tract infection (11% DTG, 8% RAL).
“People living with HIV who have developed resistance to more than one antiretroviral drug class face increasingly narrow treatment options and clinical decisions become increasingly complex. We welcome these initial results supporting the efficacy and tolerability of dolutegravir as a potentially useful addition in the management of HIV in treatment-experienced patients.” said John Pottage, chief scientific and medical officer, ViiV Healthcare. “These encouraging data were included as part of the comprehensive clinical data package supporting recent regulatory submissions for dolutegravir and we look forward to receiving the primary analysis at 48 weeks in due course.”
The primary objective of the ongoing double-blind, double-dummy phase III SAILING study is to demonstrate the antiviral activity of once-daily dolutegravir 50mg compared to twice-daily raltegravir 400mg over 48 weeks in HIV-1 infected, antiretroviral-experienced, integrase inhibitor-naïve adults. At baseline, 715 study participants were randomised 1:1 to receive either dolutegravir or raltegravir plus investigator-selected background regimen of no more than 2 agents, one of which was fully active. All subjects had documented genotypic or phenotypic resistance to agents from at least two antiretroviral therapy drug classes, and ongoing virologic replication. Median baseline HIV-1 RNA levels were 4.18 log10 c/mL and median baseline CD4+ cell counts were 200 cells/mm3. The study population included 32% women, 42% were of African American/African heritage, and 46% of study participants were classified as CDC Class C (patients who have one or more AIDS-defining illness). The 48-week primary analysis of this study will be presented at a future scientific meeting.
S/GSK1349572 (dolutegravir, DTG) is an investigational integrase inhibitor currently in development for the treatment of HIV; it does not require an additional pharmacokinetic boosting drug to be added to the regimen. Integrase inhibitors block HIV replication by preventing the viral DNA from integrating into the genetic material of human immune cells (T-cells). This step is essential in the HIV replication cycle and is also responsible for establishing chronic infection.
SAILING is the fourth phase III dolutegravir study reporting in 2012 and 2013. Data from the two studies in treatment-naïve populations, SPRING-2 (ING113086) and SINGLE (ING114467), were announced in April and July of 2012 respectively. Data from VIKING-3 (ING112574) in integrase inhibitor-resistant patients were announced in November 2012. Dolutegravir is not yet approved as a treatment for HIV or any other indication anywhere in the world.
Dolutegravir[1] is an experimental new drug under investigation for the treatment of HIV infection. Dolutegravir is an integrase inhibitor. Also known as S/GSK1349572 or just “572”, the drug is under development by GlaxoSmithKline (GSK). Studies have shown dolutegravir to be effective in patients with resistance to the integrase inhibitor, raltegravir.[2] Clinical trials are underway to support dolutegravir in combination with abacavir and lamivudine, in a new new fixed dose combination called 572-Trii.[3] In February, 2013 the Food and Drug Administration announced that it would fast track dolutegravir’s approval process.[4]
Results from the 96-week comparison with efavirenz, SPRING-1, showed dolutegravir 50mg orally to be effective at reducing HIV viral load and raising CD4 counts in integrase-naive patients. [5]
References
- [1] American Medical Association (AMA), STATEMENT ON A NONPROPRIETARY NAME ADOPTED BY THE USAN COUNCIL (Dolutegravir) Accessed 3 December 2011.
- Dolutegravir (“572”) Holds Up in Heavily Raltegravir-Resistant Patients, Phase 2B Study Finds Nelson Vergel. The Body PRO. Accessed 23 April 2011.
- Shionogi-ViiV Healthcare Starts Phase 3 Trial for “572-Trii” Test positive airwave. The Body PRO. Accessed 23 April 2011.
- “GSK wins priority status for new HIV drug in U.S”. Reuters. 16 February 2013. Retrieved 18 February 2013.
- Horn, Tim. ViiV’s Dolutegravir Continues to Show Well After 96 Weeks, Versus Sustiva, for First-Time Treatment. AIDSmeds.com 7 Mar 2012. Accessed 14 Mar 2012.
sNDA – FDA accepts AMAG Feraheme (Ferumoxytol) sNDA for review

Feraheme (ferumoxytol)
Iron(II,III) oxide
Fe3O4
CUT PASTE OF INFO….
7 MAR 2013
The US Food and Drug Administration (FDA) has accepted for review AMAG Pharmaceuticals’ supplemental new drug application (sNDA) for Feraheme (ferumoxytol) injection for Intravenous (IV) use.
The sNDA filed is to expand the indication for ferumoxytol for the treatment of iron deficiency anemia (IDA) in adult patients with chronic kidney disease (CKD), who have failed or could not take oral iron treatment.
Ferumoxytol is currently indicated for oral use for the treatment of IDA in adult patients with CKD, according to the company.
The sNDA included the data from a global phase III program, which included two phase III clinical trials such as as IDA-301 (placebo comparator) and IDA-302 (active comparator).
The trials, which enrolled 1,400 patients, evaluated the use of ferumoxytol in a broad range of adult IDA patients, all of whom had failed or could not take oral iron treatment.
Both studies achieved the primary efficacy endpoints with statistically significant improvements in hemoglobin from baseline to the 35-day.
The studies, which also included patient-reported outcomes data as pre-specified secondary and exploratory endpoints, found no new safety signals, outside of those described in the current Feraheme (ferumoxytol) label, were observed with ferumoxytol treatment in these studies, claims the company.
In response to the application, the FDA said it will complete the review of Feraheme sNDA by 21 October 2013.
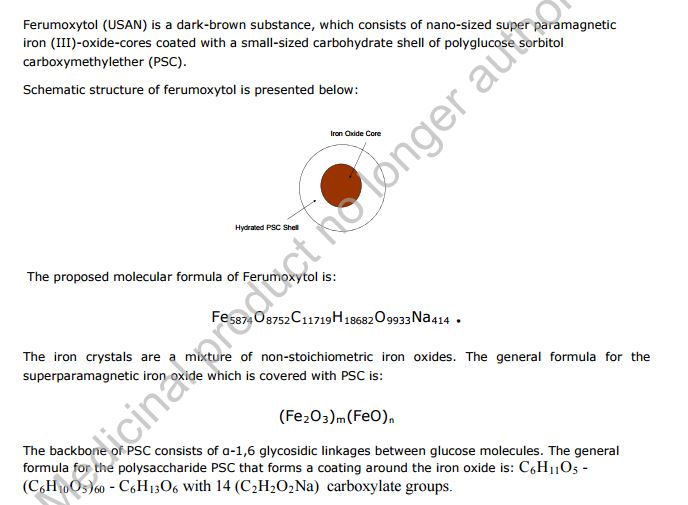
Feraheme, an iron replacement product, is a non-stoichiometric magnetite (superparamagnetic iron oxide) coated with polyglucose sorbitol carboxymethylether. The overall colloidal particle size is 17-31 nm in diameter. The chemical formula of Feraheme is Fe5874O8752-C11719H18682O9933Na414 with an apparent molecular weight of 750 kDa.
Feraheme injection is an aqueous colloidal product that is formulated with mannitol. It is a black to reddish brown liquid, and is provided in single use vials containing 510 mg of elemental iron. Each mL of the sterile colloidal solution of Feraheme injection contains 30 mg of elemental iron and 44 mg of mannitol, and has low bleomycin-detectable iron. The formulation is isotonic with an osmolality of 270-330 mOsm/kg. The product contains no preservatives, and has a pH of 6 to 8.
Ferumoxytol
STRUCTURE SOURCE http://chem.sis.nlm.nih.gov/chemidplus/rn/1309-38-2
Molecular Formulas
-
Fe.O
-
Fe3-O4
Molecular Weight
- 231.531
Ferumoxytol [USAN]
RN: 1309-38-2
Polyglucose sorbitol carboxymethyl ether-coated non-stoichiometric magnetite. Ferumoxytol is a superparamagnetic iron oxide that is coated with a low molecular weight semi-synthetic carbohydrate, polyglucose sorbitol carboxymethyl ether. The iron oxide is a superparamagnetic form of non-stoichiometric magnetite with crystal size of 6.2 to 7.3 nm. In solution, the colloidal particle of ferumoxytol has a Stokes diameter of 18-20 nm. Molecular weight is approximately 308,000
Iron oxide (Fe3O4). It is a black ore of IRON that forms opaque crystals and exerts strong magnetism. The NANOPARTICLES; and MICROSPHERES of its mineral form, magnetite, have many biomedical applications.
Ferumoxytol is the generic ingredient in one branded drug marketed by Amag Pharms Inc and is included in one NDA. There are six patents protecting this compound and one Paragraph IV challenge. Additional information is available in the individual branded drug profile pages.
This ingredient has eleven patent family members in ten countries.
There is one drug master file entry for ferumoxytol. One supplier is listed for this compound.
Phase II
Cas 722492-56-0
Launched – 2009, Anemia, iron deficiency
7228
AMI-7228
Code-7228
A superparamagnetic iron oxide (non-stoichiometric magnetite) coated with a low molecular weight semi-synthetic carbohydrate polyglucose carboxymethyl ether; USAN (OO-74) (Advanced Magnetics, Cambridge, MA, USA)
Other Names
- C 7228
- Code 7228
- Cytogen
- Feraheme
- Rienso
Superparamagnetic iron oxide coated with a low molecular weight semi-synthetic carbohydrate polyglucose sorbitol carboxymethyl ether. The iron oxide is a superparamagnetic form of non-stoichiometric magnetite with crystal size of 6.2 to 7.3 nm. In solution, the colloidal particle has a Stokes diameter of 18-20 nm
CLICK ON IMAGE
CLICK O IMAGE

Feraheme, an iron replacement product, is a non-stoichiometric magnetite (superparamagnetic iron oxide) coated with polyglucose sorbitol carboxymethylether. The overall colloidal particle size is 17-31 nm in diameter. The chemical formula of Feraheme is Fe5874O8752C11719H18682O9933Na414 with an apparent molecular weight of 750 kDa.
Feraheme Injection is an aqueous colloidal product that is formulated with mannitol. It is a black to reddish brown liquid, and is provided in single use vials containing 510 mg of elemental iron. Each mL of the sterile colloidal solution of Feraheme Injection contains 30 mg of elemental iron and 44 mg of mannitol, and has low bleomycin-detectable iron. The formulation is isotonic with an osmolality of 270-330 mOsm/kg. The product contains no preservatives, and has a pH of 6 to 8.
Ferumoxytol is AMAG Pharmaceuticals’ lead investigational compound. In 2007, the company filed a regulatory application seeking approval in the U.S. for use as an intravenous iron replacement therapeutic in patients who may be on dialysis and are suffering from anemic chronic kidney disease (CKD). In 2009, FDA approval was assigned and the product became available on the market. A regulatory application was filed in the E.U. in 2010 for this indication and a positive opinion was received in 2012. Final E.U. approval was obtained in June 2012. In 2012, AMAG Pharmaceuticals submitted a supplemental NDA to the FDA for the treatment of patients with iron-deficiency anemia (IDA) who are not candidates for oral iron, for which they received a complete response letter in January 2014. In 2013, Takeda filed for approval for this indication in the E.U. This application was withdrawn in 2015 due to safety concerns.
In terms of clinical studies, phase II trials are underway at AMAG and at Oregon Health and Science University for use in magnetic resonance angiography (MRA). The National Cancer Institute is also conducting phase II trials for the imaging of primary high-grade brain tumors and/or cerebral metastases from lung or breast cancer. Phase I clinical trials are ongoing at Dana-Farber Cancer Institute for use in magnetic resonance imaging in pediatric and adult patients with malignant sarcoma.
The drug consists of intravenously administered bioavailable iron which allows for more efficient replenishment of the body’s iron stores than oral iron supplements, without their associated common side effects. Ferumoxytol is a blood pool agent, a true intravascular contrast agent that remains in the blood stream for an extended period of time. Based on this quality, the product may be useful as a contrast agent in a wide range of applications in MRI.
In 2008, fast track designation was received in the U.S. as a diagnostic agent for vascular-enhanced magnetic resonance imaging (VE-MRI) to improve the assessment of peripheral arterial disease in patients with known or suspected chronic kidney disease. In 2010, a license, development and commercialization agreement was established between Takeda and AMAG Pharmaceuticals in Asia Pacific countries (excluding Japan, China and Taiwan), Canada, Europe, the Commonwealth of Independent States and Turkey. However, in December 2014, both companies announced the termination of this license agreement. In 2011, orphan drug designation was assigned by the FDA for use in magnetic resonance imaging in brain metastases. This designation was assigned in 2012 for use in magnetic resonance imaging to assess, and monitor treatment of solid tumor malignancies previously diagnosed in pediatric patients (age 16 years and younger).
SFDA

As announced in May 2008, we entered into a development and commercialization agreement with AMAG Pharmaceuticals, Inc. (“AMAG”) (NASDAQ:AMAG), a US biopharmaceutical company, for ferumoxytol, an intravenous iron replacement therapeutic agent being developed to treat iron deficiency anemia in CKD patients and in patients requiring hemodialysis.
Under the terms of the agreement, AMAG granted us exclusive rights to develop and commercialize ferumoxytol in the PRC, initially for CKD, and with an option to expand into additional indications. We will be responsible for the clinical development, registration, and commercialization of ferumoxytol in the PRC. We and AMAG will form a joint steering committee, with equal representation from both parties, to oversee and guide the development and commercialization of ferumoxytol in China. The agreement has an initial duration of 13 years and will be automatically renewed for a set term if minimum sales thresholds are achieved. AMAG will retain all manufacturing rights for ferumoxytol and will provide, under a separate agreement, commercial supply to us at a predetermined supply price.
Ferumoxytol was approved in June 2009 by the U.S. Food and Drug Administration to treat iron deficiency anemia in CKD patients and launched commercially in the U.S. by AMAG in July 2009. Ferumoxytol received marketing approval in Canada in December 2011 and a positive recommendation for approval from the Committee for Medicinal Products for Human Use of the European Medicines Agency in April 2012.
We have submitted the application for a registrational clinical trial for ferumoxytol to SFDA, as announced in January 2010. Once approved by the SFDA, we will commence a multi-center randomized efficacy and safety study in China with approximately 200 CKD patients, measuring the mean change in hemoglobin from baseline at Day 35 after first dose.
https://www.google.com/patents/US20100266644
Ferumoxytol is a newer parenteral iron formulation but limited information is available as to its efficacy and administration. See e.g., Landry et al. (2005) Am J Nephrol 25, 400-410, 408; and Spinowitz et al. (2005) Kidney Intl 68, 1801-1807; U.S. Pat. No. 6,599,498.
Another example of a preferred iron carbohydrate complex for use in the methods described herein is a carboxyalkylated reduced polysaccharide iron oxide complex (e.g., ferumoxytol, described in U.S. Pat. No. 6,599,498).
Another preferred iron carbohydrate complex for use in the methods described herein is a polyglucose sorbitol carboxymethyl ether-coated non-stoichiometric magnetite (e.g., “ferumoxytol”). Ferumoxytol is known in the art to be effective for treating anemia (at single unit doses lower than described herein). See e.g., Spinowitz et al. (2005) Kidney Intl 68, 1801-1807. Ferumoxytol is a superparamagnetic iron oxide that is coated with a low molecular weight semi-synthetic carbohydrate, polyglucose sorbitol carboxymethyl ether. Ferumoxytol and its synthesis are described in U.S. Pat. No. 6,599,498, incorporated herein by reference. Safety, efficacy, and pharmacokinetics of ferumoxytol are as described, for example, in Landry et al. (2005) Am J Nephrol 25, 400-410, 408; and Spinowitz et al. (2005) Kidney Intl 68, 1801-1807.
The iron oxide of ferumoxytol is a superparamagnetic form of non-stoichiometric magnetite with a crystal size of 6.2 to 7.3 nm. Average colloidal particle size can be about 30 nm, as determined by light scattering. Molecular weight is approximately 750 kD. The osmolarity of ferumoxytol is isotonic at 297 mOsm/kg and the pH is neutral. The blood half-life of ferumoxytol is approximately 10-14 hours. It has been previously reported that ferumoxytol can be given by direct intravenous push over 1-5 minutes in doses up to 1,800 mg elemental iron per minute, with maximal total dose up to 420 mg per injection. Landry et al. (2005) Am J Nephrol 25, 400-410, 408.
About Feraheme® (ferumoxytol)/Rienso
In the United States, Feraheme (ferumoxytol) Injection for Intravenous (IV) use is indicated for the treatment of iron deficiency anemia (IDA) in adult patients who have failed oral iron therapy. Feraheme received marketing approval from the FDA on June 30, 2009 for the treatment of IDA in adult chronic kidney disease (CKD) patients and was commercially launched by AMAG in the U.S. shortly thereafter.
Ferumoxytol is protected in the U.S. by five issued patents covering the composition and dosage form of the product. Each issued patent is listed in the FDA’s Orange Book. These patents are set to expire in March 2020; a request for patent term extension has been filed, which, if granted, may extend the patent term to June 2023 for one of the patents.
Ferumoxytol received marketing approval in Canada in December 2011, where it is marketed by Takeda as Feraheme, and in the European Union in June 2012 and Switzerland in August 2012, where it is marketed by Takeda as Rienso.
For additional U.S. product information, including full prescribing information, please visit www.feraheme.com.
AMAG now has five Orange Book-listed patents for ferumoxytol, with patent protection through March 2020, without patent term extension. AMAG has applied for a patent term extension for an Orange Book-listed ferumoxytol patent, which would lengthen that patent term through June 2023.
//////////Ferumoxytol, AMAG Pharmaceuticals, Phase II, 722492-56-0, Launched, 2009, Anemia, iron deficiency, 7228 , AMI-7228 , Code-7228
[Fe](O[Fe]=O)O[Fe]=O
DRUG REVIEW-Calcitonin,Miacalcin

• Molecular weight is 3434.8 g/mol
Generic name: Calcitonin
| Calcitonin-related polypeptide alpha | |||
|---|---|---|---|
 NMR solution structure of salmon calcitonin in SDS micelles.[1] |
Calcitonin (also known as thyrocalcitonin) is a 32-amino acid linear polypeptidehormone that is produced in humans primarily by the parafollicular cells (also known as C-cells) of the thyroid, and in many other animals in the ultimobranchial body.[2] It acts to reduce blood calcium (Ca2+), opposing the effects of parathyroid hormone (PTH).[3] Calcitonin has been found in fish, reptiles, birds, andmammals. Its importance in humans has not been as well established as its importance in other animals, as its function is usually not significant in the regulation of normal calcium homeostasis.[4] It belongs to calcitonin-like protein family.
After the menopausal period for women, bone loss accelerates very quickly which leads to osteoporosis.Miacalcin is a medication that can treat this type of bone disease. Miacalcin is a hormone that is created by the thyroid gland that is responsible in decreasing the calcium and phosphate in the blood and helps in the building of bones. It does not only help in the formation of bones but also strengthens the bones.
Miacalcin is a medication also distributed under the brand names Fortical. Miacalcin is a prescribed medication used in the treatment of patients with bone diseases such as osteoporosis and Paget’s disease. This medication can also be used in treating severe elevated blood calcium levels.
There are two methods of administering Miacalcin, through injection and nasal spray. The standard dosage for patients with post-menopausal osteoporosis and Paget’s disease is at least 100 to 200 units a day injected into the muscle or equivalent or 1 spray for the nasal spray.
Nasal spray should be administered in one nostril everyday on an alternating basis. Patients must never prolong the use of nasal spray than what is prescribed by the doctor.
Patients need to have enough vitamin D and calcium to help optimize the result of the medication.
If you have missed a dose, never take a double dose because this will cause overdose and is fatal. In case of overdose, seek immediate medical attention.
Basically, side effects are rare and mild. They typically do not post severe risks and are not life threatening. Some patients may experience wamble and sometimes emesis. The wamble is only temporary and will eventually disappear as the patient continues with the medication. Injected Miacalcin can cause skin irritation on the area of injection. On some patients, skin rashes and flushing occurs.
For the nasal spray, the most common side effects include nose bleeding, headaches, rhinorrhea and bone pain. It may also cause stomach upset but this is a rare case.
Some patients may have allergic reactions, which may cause chest pains, trouble in breathing, tingling of hands, difficulties in urinating and skin rashes. If any of the symptoms or side effects occur, it is important to seek immediate medical attention.
Before using the medication, discuss with your doctor any other medical ailments that you have that might conflict with the use of the medicine. It would also be necessary to tell your doctor if you are pregnant, breastfeeding our planning to get pregnant before taking the medication.
Also inform your doctor if you are taking any other prescribed medication or over the counter medicine before taking Miacalcin. Never discontinue using the medication without consulting with your doctor first.
As a prescribed medication it should not be shared to anyone else. Proper storage of the medication should be maintained.
Calcitonin is a polypeptide hormone secreted by the parafollicular cells of the thyroid gland in mammals and by the ultimobranchial gland of birds and fish.
Miacalcin® (calcitonin-salmon) Injection, Synthetic is a synthetic polypeptide of 32 amino acids in the same linear sequence that is found in calcitonin of salmon origin. This is shown by the following graphic formula:
 |
It is provided in sterile solution for subcutaneous or intramuscular injection. Each milliliter contains: calcitonin-salmon 200 I.U., acetic acid, USP, 2.25 mg; phenol, USP, 5.0 mg; sodium acetate trihydrate, USP, 2.0 mg; sodium chloride, USP, 7.5 mg; water for injection, USP, qs to 1.0 mL.
The activity of Miacalcin Injection is stated in International Units based on bioassay in comparison with the International Reference Preparation of calcitonin-salmon for Bioassay, distributed by the National Institute for Biological Standards and Control, Holly Hill, London.

PDB 2glhAndreotti G, Méndez BL, Amodeo P, Morelli MA, Nakamuta H, Motta A (August 2006). “Structural determinants of salmon calcitonin bioactivity: the role of the Leu-based amphipathic alpha-helix”. J. Biol. Chem. 281 (34): 24193–203.doi:10.1074/jbc.M603528200. PMID 16766525.
NDA FDA-Nuvo reports FDA response to PENNSAID 2% , diclofenac sodium topical solution, 2% w/w

DICLOFENAC

PENNSAID 2%
7 MAR 2013
The US Food and Drug Administration (FDA) has issued a Complete Response Letter (CRL) to Nuvo Research’s US licensing partner, Mallinckrodt, following the review of Mallinckrodt’s New Drug Application (NDA) for diclofenac sodium topical solution, 2% w/w (PENNSAID 2%).
FDA in the letter mentioned that it requires Mallinckrodt’s complete pharmacokinetic study comparing PENNSAID 2% to original PENNSAID 1.5%.
FDA denied to review the similar pharmacokinetic studies submitted by Mallinckrodt with the NDA, as the reserve samples were not retained at the clinical site.
Pharmacokinetic studies are standard studies conducted during a drug development program to identify the total exposure or the amount of drug that reaches the blood stream after a patient receives both single and multiple doses of the product.
Mallinckrodt has suggested Nuvo that it expects to complete the study and submit the results to the FDA in the third quarter of 2013, and that it anticipates the FDA will provide a formal response to the filing within 6 months thereafter.
Nuvo’s Pain Group president Dr. Bradley Galer said with the new FDA’s letter the firm was disappointed that PENNSAID 2% will not be approved in this review cycle.
“We are pleased that the FDA has outlined a clear pathway to approval that we believe can be completed in a relatively short time frame,” Galer added.
“Upon approval, PENNSAID 2% will be the first and only topical NSAID in the U.S. featuring twice per day dosing and a metered dose pump bottle.”
Takeda Submits Marketing Authorisation Application for Vedolizumab in Moderately to Severely Active Ulcerative Colitis and Crohn’s Disease in the European Union

March 7, 2013
Pharmaceutical Company Limited (“Takeda”) today announced that a Marketing Authorisation Application (MAA) has been submitted to The European Medicines Agency (EMA) for vedolizumab, an investigational, gut-selective humanized monoclonal antibody for the treatment of adults with moderately to severely active ulcerative colitis (UC) and Crohn’s disease (CD), the two most common types of inflammatory bowel disease (IBD). If approved, vedolizumab would be the first and only gut-selective biologic agent for UC and CD on the market.
“Ulcerative colitis and Crohn’s disease are chronic debilitating diseases with important unmet medical needs, often affecting young people in the prime of their lives,” said Asit Parikh, M.D., Ph.D., vice president, general medicine, Takeda. “We are encouraged by the findings of GEMINI, the vedolizumab Phase 3 clinical development program, which studied approximately 3,000 patients in nearly 40 countries, making it the largest IBD clinical trial program conducted to date.”
Nearly four million people worldwide are affected by IBD, with UC affecting more than 500,000 people and CD affecting approximately 230,000 people in the EU. Crohn’s disease and ulcerative colitis are chronic diseases that cause inflammation of the lining of the digestive tract. Inflammation caused by CD can involve varying areas of the digestive tract, while UC impacts the colon only. CD and UC can be both painful and debilitating, which may sometimes lead to serious complications and can significantly impact the quality of life for patients.
The MAA submission was supported by Phase 3 clinical studies, GEMINI I, GEMINI II, GEMINI III and GEMINI LTS (Long-term Safety), which are part of the GEMINI Studies™, a four-study clinical research program to investigate the efficacy and safety of vedolizumab on clinical response and remission in moderately to severely active CD and UC patients, who had failed at least one conventional or anti-TNFα therapy.
“With a targeted mechanism of action, vedolizumab has clinical promise as a potential treatment option for people with moderate to severely active CD and UC,” said Paul Rutgeerts, M.D., Ph.D., F.R.C.P., professor of medicine, Catholic University of Leuven, Belgium. “While there is no known cure, there is a need for new CD and UC treatment options, in an effort to provide patients with additional choices for managing their disease, reducing symptoms and achieving remission.”
About Crohn’s disease and ulcerative colitis
Crohn’s disease (CD) and ulcerative colitis (UC) are the two most common forms of inflammatory bowel disease (IBD), which is marked by inflammation in the lining of the GI tract. CD can impact any part of the digestive tract, and common symptoms may include abdominal pain, diarrhea, rectal bleeding, weight loss, and/or fever. UC impacts the large intestine only, which includes the colon and the rectum. The most common symptoms of UC include abdominal discomfort and blood or pus in diarrhea. There is no known cause for CD or UC, although many researchers believe that the interaction of an outside agent, such as a virus or bacteria, with the body’s immune system may trigger them. No cure exists for CD or UC; the aim of IBD treatments is to induce and maintain remission, or achieve extended periods of time when patients do not experience symptoms.
About vedolizumab
Vedolizumab was developed for the treatment of CD and UC, as a gut-selective, humanized monoclonal antibody that specifically antagonizes the alpha4beta7 (α4β7) integrin, which is expressed on a subset of circulating white blood cells. These cells have been shown to play a role in mediating the inflammatory process in CD and UC. α4β7 binds with a specific adhesion molecule primarily expressed in the intestinal tract. Therefore, vedolizumab, by preventing this interaction, has a gut selective effect.
About Takeda Pharmaceutical Company Limited
Located in Osaka, Japan, Takeda is a research-based global company with its main focus on pharmaceuticals. As the largest pharmaceutical company in Japan and one of the global leaders of the industry, Takeda is committed to strive towards better health for patients worldwide through leading innovation in medicine. Additional information about Takeda is available through its corporate website, http://www.takeda.com.
Vedolizumab is a monoclonal antibody being developed by Millennium Pharmaceuticals, Inc. for the treatment of ulcerative colitis and Crohn’s disease.It binds to integrin α4β7(LPAM-1, lymphocyte Peyer’s patch adhesion molecule 1).[1][2]
The molecule was first identified by Dr. Andrew Lazarovits [1][2] as the murine MLN0002 homologue. His discovery of the mouse equivalent of this antibody—originally applied to anti-rejection strategies in kidney transplantation—was published in the journal Nature in 1996. The drug was then licensed to Millennium Pharmaceuticals of Boston for further development.
As of October 2009, vedolizumab is undergoing Phase III trials.[3] Clinical trials indicate that Vedolizumab was found safe and highly effective for inducing and maintaining clinical remission in patients with moderate to severe ulcerative colitis [3]. Dr. Brian Faegan, head researcher, reported an absence of any instances of progressive multifocal leukoencephalopathy (PML), which is a particularly important finding [4]. It looks like it will be an effective abiologic agent without some of the toxicity issues previously seen with anti-TNF drugs .
It is widely believed now that “vedolizumab can be used either as a first-line treatment or in case of anti-TNF failure”
- Statement On A Nonproprietary Name Adopted By The USAN Council – Vedolizumab, American Medical Association.
- Soler, D; Chapman, T; Yang, LL; Wyant, T; Egan, R; Fedyk, ER (2009). “The binding specificity and selective antagonism of vedolizumab, an anti-alpha4beta7 integrin therapeutic antibody in development for inflammatory bowel diseases”. The Journal of Pharmacology and Experimental Therapeutics 330 (3): 864–75. doi:10.1124/jpet.109.153973. PMID 19509315.
- ClinicalTrials.gov NCT00790933 Study of Vedolizumab (MLN0002) in Patients With Moderate to Severe Crohn’s Disease (GEMINI II)

Phase 3-Trius Therapeutics will soon be reporting data from its second phase III trial of Tedizolid
Tedizolid
(5R)-3-{3-fluoro-4-[6-(2-methyl-2H-tetrazol-5-yl)pyridin-3-yl]phenyl}-5-(hydroxymethyl)-1,3-oxazolidin-2-one
- Molecular Formula: C17H15FN6O3
- Average mass: 370.337799
856866-72-3 cas no
Torezolid (also known as TR-701 and now tedizolid[1]) is an oxazolidinone drug being developed by Trius Therapeutics (originator Dong-A Pharmaceuticals) for complicated skin and skin-structure infections (cSSSI), including those caused by Methicillin-resistantStaphylococcus aureus (MRSA).[2]
As of July 2012, tedizolid had completed one phase III trial, with another one under way. [3]Both trials compare a six-day regimen of tedizolid 200mg once-daily against a ten-day regimen of Zyvox (linezolid) 600mg twice-daily.
The prodrug of tedizolid is called “TR-701”, while the active ingredient is called “TR-700”.[4][5]

March 5 2013
Trius Therapeutics will soon be reporting data from its second phase III trial (ESTABLILSH-2) and the recently announced publication of the data from its first phase III trial (ESTABLISH-1) in the Journal of the American Medical Association (JAMA)
- “Trius grows as lead antibiotic moves forward”. 31 Oct 2011.
- “Trius Completes Enrollment In Phase 2 Clinical Trial Evaluating Torezolid (TR-701) In Patients With Complicated Skin And Skin Structure Infections”. Jan 2009.
- http://clinicaltrials.gov/ct2/results?flds=Xf&flds=a&flds=b&term=tedizolid&phase=2&fund=2&show_flds=Y
- PMID 19528279 In vitro activity of TR-700, the active ingredient of the antibacterial prodrug TR-701, a novel oxazolidinone antibacterial agent.
- PMID 19218276 TR-700 in vitro activity against and resistance mutation frequencies among Gram-positive pathogens.
Phase 1-Sangamo Presents New Clinical Data at CROI 2013 Demonstrating Persistent Immune System Improvements After Treatment With ZFN Therapeutic(R) SB-728-T

The gene therapy diminished the levels of virus and eradicated in patients having naturally occurring mutation of gene, found a preliminary trail of HIV treatment. The first phase of very small trail tested the SB-728-T gene treatment that is intended to interrupt theCCR5 gene used by HIV to contaminate immune system cells.
The first clinical trial using zinc-finger nucleases to provide long-term resistance to HIV-1 infection has been given the go-ahead by the US Food and Drug Administration. Sangamo BioSciences of Richmond, California, and its clinical partner, the University of Pennsylvania, have begun enrolling the first 12 people in a phase 1 clinical trial to evaluate SB-728-T, a novel zinc-finger DNA-binding nuclease that permanently disrupts the CCR5 gene on CD4+ T cells (Nat. Biotechnol. 26, 808–816, 2008
Data Demonstrate that SB-728-T Possesses Necessary Immunologic Properties to Support a ‘Functional Cure’ for HIV/AIDS
RICHMOND, Calif., March 6, 2013
Sangamo BioSciences, Inc. announced new data from its program to develop a ‘functional cure’ for HIV/AIDS in two presentations at the 20th Conference on Retroviruses and Opportunistic Infections (CROI), held in Atlanta from March 3 to 6, 2013.
The first presentation described data from the SB-728-T Phase 1 study (SB-728-902, Cohorts 1-3) demonstrating that SB-728-T treatment of HIV-infected subjects leads to durable reconstitution of the immune system driven by increases in total CD4+ central memory T-cells (TCM) and CCR5-protected TCM. TCM are long-lived, self-renewing cells that have the ability to remember and react against foreign antigens including HIV. The data also showed that certain cell surface marker and gene expression profiles may predict which patients will likely respond best to SB-728-T treatment.
About Sangamo
Sangamo BioSciences, Inc. is focused on research and development of novel DNA-binding proteins for therapeutic gene regulation and genome editing. The Company has ongoing Phase 2 clinical trials to evaluate the safety and efficacy of a novel ZFP Therapeutic® for the treatment of HIV/AIDS. Sangamo’s other therapeutic programs are focused on monogenic diseases, including hemophilia, Huntington’s disease and hemoglobinopathies such as beta-thalassemia and sickle cell anemia. Sangamo’s core competencies enable the engineering of a class of DNA-binding proteins known as zinc finger DNA-binding proteins (ZFPs). Engineering of ZFPs that recognize a specific DNA sequence enables the creation of sequence-specific ZFP Nucleases (ZFNs) for gene modification and ZFP transcription factors (ZFP TFs) that can control gene expression and, consequently, cell function. Sangamo has entered into a strategic collaboration with Shire AG to develop therapeutics for hemophilia, Huntington’s disease and other monogenic diseases and has established strategic partnerships with companies in non-therapeutic applications of its technology including Dow AgroSciences and Sigma-Aldrich Corporation. For more information about Sangamo, visit the company’s website atwww.sangamo.com.
Phase III Study of Oral Laquinimod for Relapsing-Remitting Multiple Sclerosis

Laquinimod
5-chloro-N-ethyl-4-hydroxy-1-methyl-2-oxo-
N-phenyl-1,2-dihydroquinoline-3-carboxamide
Laquinimod is an experimental immunomodulator developed by Active Biotech and Teva. It is currently being investigated as an oral treatment for multiple sclerosis (MS).
Laquinimod is the successor of Active Biotech’s failed experimental immunomodulator linomide.[1]
The compound has been investigated in two Phase II trials using successive magnetic resonance scans (MRI). Laquinimod seems to be able to reduce the MS disease activity on MRI.[2][3] However, the response to a given dose was discrepant between both studies.[4]
Phase III studies for MS started in December 2007.[5] In 2011, Teva announced its clinical trials involving laquinimod had failed, being unable to significantly reduce relapses into MS among patients beyond a placebo.[6] However, the final results of above mentioned phase III trial proved oral laquinimod administered once daily slowed the progression of disability and reduced the rate of relapse in patients with relapsing–remitting multiple sclerosis [7]
Mar 6, 2013 –
CONCERTO Study Enrolling Patients Globally to Evaluate Impact of Laquinimod on Disability Progression
Teva Pharmaceutical Industries Ltd. and Active Biotech announced today enrollment of the first patient in the CONCERTO study – the third Phase III placebo-controlled study designed to evaluate the efficacy, safety and tolerability of once-daily oral laquinimod in patients with relapsing-remitting multiple sclerosis (RRMS). The primary outcome measure of CONCERTO will be confirmed disability progression as measured by the Expanded Disability Status Scale (EDSS).
“Previous Phase III studies in more than 2,400 people with RRMS suggest a unique profile of laquinimod, directly affecting the neurodegenerative processes that lead to disability progression, the main concern in the treatment of RRMS,” said CONCERTO principal investigator, Dr. Timothy Vollmer, Professor of Neurology, University of Colorado Denver, Medical Director of the Rocky Mountain Multiple Sclerosis Center, and Co-Director of the RMMSC at Anschutz. “We are currently enrolling patients in this third pivotal study to further examine the clinical benefits of laquinimod on disability progression, the primary endpoint of the CONCERTO trial, and brain atrophy, at both the previously studied 0.6 mg dose, and now a higher 1.2 mg dose.”
The multinational, randomized, double blind placebo-controlled study will aim to enroll approximately 1,800 patients at more than 300 sites globally (http://clinicaltrials.gov/show/NCT01707992). Along with the primary endpoint of time to confirmed disability progression, the study will also examine the impact of laquinimod on endpoints such as percent change in brain volume and other clinical and MRI markers of disease activity.
“For nearly 30 years, Teva has been focused on improving the lives of people with multiple sclerosis by delivering innovative treatment options that address this complex disease,” said Dr. Michael Hayden, President of Global R&D and Chief Scientific Officer at Teva Pharmaceutical Industries Ltd. “The CONCERTO study demonstrates our commitment to collaborating with MS communities worldwide to further develop laquinimod and address unmet patient needs.”
ABOUT LAQUINIMOD
Laquinimod is an oral, once-daily CNS-active immunomodulator with a novel mechanism of action being developed for the treatment of MS. In animal models laquinimod crosses the blood brain barrier to potentially have a direct effect on resident CNS inflammation and neurodegeneration. The global Phase III clinical development program evaluating oral laquinimod in MS includes two pivotal studies, ALLEGRO and BRAVO.
In addition to the MS clinical studies, laquinimod is currently in clinical development for Crohn’s disease and Lupus.
ABOUT CONCERTO
CONCERTO is a multinational, multicenter, randomized, double-blind, parallel-group, placebo-controlled study followed by an active treatment phase, to evaluate the efficacy, safety and tolerability of two doses of oral administration of laquinimod 0.6 mg/day or 1.2 mg/day in subjects with RRMS. This third Phase III laquinimod study will evaluate laquinimod in approximately 1,800 patients for up to 24 months, after which patients will continue to an active treatment period with laquinimod for an additional 24 months. The primary outcome measure will be time to confirmed disability progression as measured by the Expanded Disability Status Scale (EDSS). The study will also examine the impact of laquinimod on endpoints such as percent change in brain volume, as well as other clinical and MRI markers of disease activity.
ABOUT MULTIPLE SCLEROSIS
MS is the leading cause of neurological disability in young adults. It is estimated that more than 400,000 people in the United States are affected by the disease and that two million people may be affected worldwide. Multiple sclerosis is a degenerative disease of the central nervous system in which inflammation and axonal damage and loss result in the development of progressive disability.
ABOUT TEVA
Teva Pharmaceutical Industries Ltd. (NYSE: TEVA) is a leading global pharmaceutical company, committed to increasing access to high-quality healthcare by developing, producing and marketing affordable generic drugs as well as innovative and specialty pharmaceuticals and active pharmaceutical ingredients. Headquartered in Israel, Teva is the world’s leading generic drug maker, with a global product portfolio of more than 1,000 molecules and a direct presence in about 60 countries. Teva’s branded businesses focus on CNS, oncology, pain, respiratory and women’s health therapeutic areas as well as biologics. Teva currently employs approximately 46,000 people around the world and reached $20.3 billion in net revenues in 2012.
ABOUT ACTIVE BIOTECH
Active Biotech AB is a biotechnology company with focus on autoimmune/inflammatory diseases and cancer. Projects in or entering pivotal phase are laquinimod, an orally administered small molecule with unique immunomodulatory properties for the treatment of multiple sclerosis, TASQ for prostate cancer as well as ANYARA for use in cancer targeted therapy, primarily of renal cell cancer. In addition, laquinimod is in Phase II development for Crohn’s and Lupus. Further projects in clinical development comprise the two orally administered compounds, 57-57 for SLE & Systemic Sclerosis and RhuDex(TM) for RA. Please visit http://www.activebiotech.com for more information.
- Tan IL, Lycklama à Nijeholt GJ, Polman CH et al. (April 2000). “Linomide in the treatment of multiple sclerosis: MRI results from prematurely terminated phase-III trials”. Mult Scler 6 (2): 99–104. PMID 10773855.
- Comi G, Pulizzi A, Rovaris M et al. (June 2008). “Effect of laquinimod on MRI-monitored disease activity in patients with relapsing-remitting multiple sclerosis: a multicentre, randomised, double-blind, placebo-controlled phase IIb study”. Lancet 371 (9630): 2085–2092. doi:10.1016/S0140-6736(08)60918-6. PMID 18572078.
- Polman C, Barkhof F, Sandberg-Wollheim M et al. (March 2005). “Treatment with laquinimod reduces development of active MRI lesions in relapsing MS”. Neurology 64 (6): 987–91. doi:10.1212/01.WNL.0000154520.48391.69. PMID 15781813.
- Keegan BM, Weinshenker BG (June 2008). “Laquinimod, a new oral drug for multiple sclerosis”. Lancet 371 (9630): 2059–2060. doi:10.1016/S0140-6736(08)60894-6. PMID 18572062.
- ClinicalTrials.gov NCT00509145 Safety and Efficacy of Orally Administered Laquinimod Versus Placebo for Treatment of Relapsing Remitting Multiple Sclerosis (RRMS) (ALLEGRO)
- Kresege, Naomi (1 August 2011). “Teva’s Copaxone Successor Fails in Latest Clinical Trial”. Bloomberg. http://www.bloomberg.com/news/2011-08-01/teva-s-oral-multiple-sclerosis-drug-fails-to-meet-goal-of-clinical-trial.html. Retrieved 2 August 2011. “Teva Pharmaceutical Industries Ltd. (TEVA)’s experimental multiple sclerosis pill failed to reduce relapses more than placebo in a clinical trial, dealing a blow to the company’s effort to find a successor to an older drug.”
- (Comi et al. N Engl J Med 2012;366:1000).

EP 1073639; JP 2002513006; US 6077851; WO 9955678
5-Chloroisatoic anhydride (I) is alkylated with iodomethane and NaH to afford (II). Subsequent condensation of anhydride (II) with the malonic monoamide (III) in the presence of NaH in hot DMA furnishes the target quinoline carboxamide.
…

Reaction of 2-amino-6-chlorobenzoic acid (I) with phosgene and NaHCO3 in dioxane gives 5-chloroisatoic anhydride (II), which is methylated by means of iodomethane and NaH in DMF to yield 5-chloro-1-methylisatoic anhydride (III). Finally, anhydride (III) is condensed with the malonic monoamide (IV) by means of NaH in hot dimethylacetamide. Alternatively, condensation of anhydride (III) with ethoxy malonyl chloride (V) by means of NaOMe and triethylamine in dichloromethane affords 5-chloro-4-hydroxy-1-methyl-2-oxo-1,2-dihydroquinoline-3- carboxylic acid ethyl ester (VI), which is finally condensed with N-ethylaniline (VII) in refluxing toluene. Alternatively, ester (VI) is hydrolyzed by means of concentrated HCl in hot Ac2O to give the carboxylic acid (VIII), which is finally condensed with N-ethylaniline (VII) by means of SOCl2 and TEA in dichloromethane
Phase 1-Lorus Therapeutics Announces Allowance of Chinese Patent for Anticancer Drug LOR-253
has a fluoro gp
WO-2004016086, feb2004
2,4,5-Trisubstituted imidazoles and their use as anti-microbial agents
WO-2006126177, nov 2006
WO-2010102393, sept 2010
Description of LOR-253, LT253: LOR-253 HCl is the hydrochloride salt of a small molecule inhibitor of human metal-regulatory transcription factor 1 (MTF-1) with potential antitumor activity. MTF-1 inhibitor LOR-253 inhibits MTF-1 activity and thereby induces the expression of MTF-1 dependent tumor suppressor factor Kruppel like factor 4 (KLF4). This subsequently leads to the downregulation of cyclin D1, blocking cell cycle progression and proliferation. This agent also causes decreased expression of genes involved in tumor hypoxia and angiogenesis.

http://clinicaltrials.gov/ct2/show/NCT01281592
ClinicalTrials.gov Identifier: NCT01281592
Lorus Therapeutics
This is an open-label, phase 1 study to determine the maximum tolerated dose (MTD) or appropriate target dose if MTD not reached to identify the recommended phase 2 dose of LOR-253 HCl in patients with advanced or metastatic solid tumours.
March 5, 2013) – Lorus Therapeutics Inc. (“Lorus”), a biopharmaceutical company specializing in the discovery, research and development of pharmaceutical products and technologies for the management of cancer, today announced that Lorus’ patent for its lead small molecule anticancer drug LOR-253 has been allowed in China. The patent provides Lorus with exclusive rights to LOR-253 in China until 2026.
The Chinese patent provides composition of matter protection for LOR-253 and for use in the manufacture of therapies for the treatment of cancer. The patent covers a wide range of cancers, including leukemia, melanoma, as well as non-small cell lung, colon, prostate, and breast tumors. This patent extends the Company’s international patent portfolio which includes similar protection for LOR-253 in the United States, Canada, and Australia. Applications are pending in Europe and Japan.
“This increased patent protection for our anticancer therapies supports our business discussions with potential partners,” said Dr. Aiping Young, Lorus’ President and CEO. “This Chinese patent is an important addition to our global IP portfolio for LOR-253, and demonstrates our commitment to the development of innovative cancer therapies intended for significant markets.”
LOR-253 is currently in a clinical study at Memorial Sloan Kettering Cancer Center and MD Anderson Cancer Center evaluating tumor biomarkers in biopsy-suitable patients with advanced or metastatic solid tumors.
About LOR-253
LOR-253 represents a new class of anticancer agent, which we believe may offer a competitive advantage over conventional drugs. This drug candidate has shown selective and potent antitumor activity in preclinical investigations with a variety of human cancers, including colon cancer and non-small cell lung cancer, and has demonstrated an excellent therapeutic window due to its low toxicity. LOR-253 is a first-in-class small molecule that has been optimized to induce the novel tumor suppressor Krüppel-like factor 4 (KLF4), leading to cancer cell cycle arrest and apoptosis as well as inhibition of metastasis.
About Lorus
Lorus is a biopharmaceutical company focused on the discovery, research and development of novel therapeutics in cancer. Lorus’ goal is to capitalize on its research, preclinical, clinical and regulatory expertise by developing new drug candidates that can be used, either alone, or in combination with other drugs, to successfully manage cancer. The Company also has expertise in antimicrobial drug discovery. Lorus Therapeutics Inc. is listed on the Toronto Stock Exchange under the symbol LOR.
PHASE1,Progenics Pharmaceuticals’ Novel Small Molecule Drugs Targeting PSMA Successfully Visualize Prostate Cancer, 123-I-MIP-1095

Name: 123-I-MIP-1095
Synonym: 123-I-MIP-1095; [123I]-MIP-1095; iodine I 123 IMP-1095; 2-(3-{l-carboxy-5-[3-(4-iodo-phenyl)-ureido]-pentyl}-ureido)-pentanedioic acid.; [123I]-(S)-2-(3-((S)-1-carboxy-5-(3-(4-iodophenyl)ureido)pentyl)ureido)pentanedioic acid
IUPAC/Chemical name:
2-(3-(1-carboxy-5-(3-(4-iodophenyl)ureido)pentyl)ureido)pentanedioic acid
Chemical Formula: C19H25123IN4O8
Exact Mass: 560.07284
Molecular Weight: 560.33
123-I-MIP-1095
An iodine 123-radiolabled small molecule that exhibits high affinity for prostate-specific membrane antigen (PSMA) with potential use in molecular imaging. 123-I-MIP-1095, a radiolabeled glutamate-urea-lysine analogue, selectively binds PSMA, which allows imaging of PSMA-expressing prostate cancer cells with gamma scintigraph. PSMA is a transmembrane glycoprotein highly expressed by malignant prostate epithelial cells and vascular endothelial cells of various solid tumors.
![]()
| Synonym: | iodine I 123 IMP-1095 | ||
| Chemical structure: | 2-(3-{l-carboxy-5-[3-(4-iodo-phenyl)-ureido]-pentyl}-ureido)-pentanedioic acid | ||
March 5, 2013
Progenics Pharmaceuticals, Inc. (Nasdaq:PGNX) reported positive clinical data from a study of two novel radiolabeled small molecules targeting prostate-specific membrane antigen (PSMA). The imaging agents — 123I-MIP-1072 and 123I-MIP-1095 — had a high sensitivity of lesion detection in bone, tissue and the prostate gland with minimal retention in non-target tissue. The research was published as the cover article in the March issue of The Journal of Nuclear Medicine.
“Existing imaging techniques are limited in their ability to diagnose and stage prostate cancer,” said John J. Babich, Ph.D., senior author of the article “First-in-Man Evaluation of Two High-Affinity PSMA-Avid Small Molecules for Imaging Prostate Cancer.” “The approach described in this paper has the potential to assess disease status more accurately. It could help clinicians select optimal treatments and lead to better patient outcomes.”
Separate phase 1 studies were conducted under an exploratory investigational new drug (IND) application to measure the potential effectiveness of the small molecules in diagnosing and staging prostate cancer. In the first study, seven patients with documented prostate cancer were administered doses of 123I-MIP-1072 and 123I-MIP-1095, two weeks apart. In the second study, six healthy volunteers received 123I-MIP-1072 only. Whole body planar imaging and single photon emission computed tomography (SPECT)/computed tomography (CT) were performed for each group, and pharmacokinetics, tissue distribution, excretion, safety and organ radiation dose were analyzed.
Based on the data reported, Progenics is conductinga global, multi-center phase 2 trial investigating a next generation radiolabeled small molecule targeting PSMA, MIP-1404.
Mark R. Baker, chief executive officer of Progenics, said, “We recently acquired all of the rights to the compounds described in this Journal of Nuclear Medicine paper, as well as to the phase 2 stage imaging agent MIP-1404, through Progenics’ acquisition of Molecular Insight Pharmaceuticals. It is gratifying to see this expansion of our oncology pipeline demonstrating progress so soon.”
Robert J. Israel, M.D., Progenics’ senior vice president of medical affairs and clinical research, said, “We believe that MIP-1404 has excellent potential as a diagnostic radiopharmaceutical. Results to date from the study compounds and MIP-1404 show PSMA as a robust target for prostate cancer molecular imaging, and that a radiolabeled small molecule, which binds PSMA with high affinity, has the potential to detect prostate cancer throughout the body. Cancer treatment guidelines call for imaging prostate cancer with conventional bone scans or MRI. A more accurate method of imaging prostate cancer could be of great value.”
Mr. Baker further added, “Thought leaders in prostate cancer care are focused on avoiding unnecessary surgery and other invasive procedures due to the complications associated with them. Clinicians generally prefer “watchful waiting” when the cancer appears to be indolent. At the same time, some therapeutics to treat aggressive prostate cancer have recently been approved or are under development, such as Progenics’ own PSMA ADC, which currently is in phase 2 testing. Patients and their physicians would benefit from feedback on how therapeutic agents are impacting the course of cancer, and guidance on how and when to use therapeutic agents. It is clear that an improved way to visualize prostate cancer, with a high degree of specificity and sensitivity, would better inform both “watchful waiting” and the treatment of aggressive disease. We believe that data from the ongoing phase 2 trial of MIP-1404 will demonstrate its capabilities to assist prostate cancer patients and their physicians in making these critical decisions.”
About Prostate Cancer
Prostate cancer is the most common form of cancer affecting men in the United States and is the second leading cause of cancer deaths among men each year. The American Cancer Society estimates that in 2013, 238,590 new cases of prostate cancer will be diagnosed and approximately 29,720 American men will die from the disease. Accurate diagnosis and staging of prostate cancer is critical to determining appropriate patient management.
About Progenics
Progenics Pharmaceuticals, Inc. is discovering and developing innovative medicines for oncology, with a pipeline that includes product candidates in preclinical through late-stage development. Progenics’ first commercial product, Relistor® (methylnaltrexone bromide) for opioid-induced constipation, is marketed and in further development by Salix Pharmaceuticals, Ltd. for markets worldwide other than Japan, where Ono Pharmaceutical Co., Ltd. holds an exclusive license for the subcutaneous formulation. For additional information, please visit http://www.progenics.com.
