
 DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HERE
DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HEREFlag and hits
ORGANIC SPECTROSCOPY

SUBSCRIBE

 Subscribe in a reader
Subscribe in a reader
Enter your email address:
Delivered by FeedBurner
Subscribe to New Drug Approvals by Email![]()

![]()



![]()
![]()





Recent Comments
| shivkr2 on SPSR Excellence Award 2025 – S… | |
| Bonkasaurus on Infigratinib phosphate | |
| PALOVAROTENE | ORGAN… on Palovarotene | |
| Pfizer just purchase… on Temanogrel | |
| Pfizer To Cash In On… on Temanogrel |
BENZGALANTAMINE


BENZGALANTAMINE
CAS 224169-27-1
Benzgalantamine gluconate, 1542321-58-3
- 6H-Benzofuro[3a,3,2-ef][2]benzazepin-6-ol, 4a,5,9,10,11,12-hexahydro-3-methoxy-11-methyl-, benzoate (ester), (4aS,6R,8aS)- (9CI)
- Alpha 1062
- GLN 1062
- Memogain
6h-benzofuro(3a,3,2-ef)(2)benzazepin-6-ol, 4a,5,9,10,11,12-hexahydro-3-methoxy-11-methyl-, benzoate (ester), (4as,6r,8as)-
| Formula | C24H25NO4 |
|---|---|
| Molar mass | 391.467 g·mol−1 |


External IDs GLN-1062 gluconate
UNIILN7PMJ4P57
CAS Number1542321-58-3
WeightAverage: 587.622
Monoisotopic: 587.236661015
Chemical FormulaC30H37NO11
Benzgalantamine, sold under the brand name Zunveyl, is a medication used for the treatment of mild to moderate dementia of the Alzheimer’s type.[1] It is a cholinesterase inhibitor.[1] Benzgalantamine is a prodrug of galantamine.[1]
The most common side effects include nausea, vomiting, diarrhea, dizziness, headache, and decreased appetite.[1]
Benzgalantamine was approved for medical use in the United States in July 2024.[1][2][3]
compounds that, in addition to enhancing the sensitivity to acetylcholine and choline, and to their agonists, of neuronal cholinergic receptors, and/or acting as cholinesterase inhibitors and/or neuroprotective agents, have enhanced blood-brain barrier permeability in comparison to their parent compounds. The compounds are derived (either formally by their chemical structure or directly by chemical synthesis) from natural compounds belonging to the class of amaryllidaceae alkaloids e.g., Galantamine, Narwedine and Lycoramine, or from metabolites of said compounds. The compounds of the present invention can either interact as such with their target molecules, or they can act as “pro-drugs”, in the sense that after reaching their target regions in the body, they are converted by hydrolysis or enzymatic attack to the original parent compound and react as such with their target molecules, or both. The compounds of this disclosure may be used as medicaments for the treatment of human brain diseases associated with a cholinergic deficit, including the neurodegenerative diseases Alzheimer’s and Parkinson’s disease and the neurological/psychiatric diseases vascular dementia, schizophrenia and epilepsy. Galantamine derivatives disclosed herein have higher efficacy and lower levels of adverse side effects in comparison to galantamine, in treatment of human brain diseases.
Benzgalantamine is a prodrug of galantamine. Gastrointestinal adverse effects are the most frequently reported side effects in patients undergoing treatment with cholinesterase inhibitors, including galantamine, and are often a reason for treatment discontinuation.2 As a prodrug, benzagalantamine remains inert as it passes through the stomach, thereby avoiding many of the gastrointestinal effects associated with peripheral cholinesterase inhibition.4
Benzgalantamine was approved by the FDA in July 2024 for the treatment of mild-to-moderate dementia in Alzheimer’s patients.3,4
SCHEME


US20090253654
https://patentscope.wipo.int/search/en/detail.jsf?docId=US42863485&_cid=P12-M8ZQT3-74791-1

| O-Benzoyl-galantamine(=(4aS,6R,8aS)-4a,5,9,10,11,12-Hexahydro-3-methoxy-11-methyl-6H-benzofuro[3a,3,2-ef][2]benzazepin-6-ol, benzoate (ester)); yield: 78% |
| O-3,4-Dichlorobenzoyl-galantamine(=(4aS,6R,8aS)-4a,5,9,10,11,12-Hexahydro-3-methoxy-11-methyl-6H-benzofuro[3a,3,2-ef][2]benzazepin-6-ol, 3,4-dichlorobenzoate (ester)); off-white solid; mp. 69-70° C. |
WO2009127218
US20220220121
https://patentscope.wipo.int/search/en/detail.jsf?docId=US368470159&_cid=P12-M8ZR8V-88578-1
Experiment 1
The gluconate salt of Alpha-1062 was created according to the following previously established general scheme:

AND
US20090253654
Medical uses
Benzgalantamine is indicated for the treatment of mild to moderate dementia of the Alzheimer’s type in adults.[1][2]
Side effects
The most common side effects include nausea, vomiting, diarrhea, dizziness, headache, and decreased appetite.[1]
Society and culture
Legal status
Benzgalantamine was approved for medical use in the United States in July 2024.[1][2]
Names
Benzgalantamine is the international nonproprietary name.[4]
References
- ^ Jump up to:a b c d e f g h i “Zunveyl- benzgalantamine tablet, delayed release”. DailyMed. 8 August 2024. Retrieved 15 August 2024.
- ^ Jump up to:a b c https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2024/218549Orig1s000ltr.pdf
- ^ “Alpha Cognition’s Oral Therapy Zunveyl Receives FDA Approval to Treat Alzheimer’s Disease” (Press release). Alpha Cognition. 29 July 2024. Archived from the original on 4 August 2024. Retrieved 4 August 2024 – via Business Wire.
- ^ World Health Organization (2022). “International nonproprietary names for pharmaceutical substances (INN): recommended INN: list 88”. WHO Drug Information. 36 (3). hdl:10665/363551.
- Baakman AC, ‘t Hart E, Kay DG, Stevens J, Klaassen ES, Maelicke A, Groeneveld GJ: First in human study with a prodrug of galantamine: Improved benefit-risk ratio? Alzheimers Dement (N Y). 2016 Jan 20;2(1):13-22. doi: 10.1016/j.trci.2015.12.003. eCollection 2016 Jan. [Article]
- Bakker C, van der Aart J, Hart EP, Klaassen ES, Bergmann KR, van Esdonk MJ, Kay DG, Groeneveld GJ: Safety, pharmacokinetics, and pharmacodynamics of Gln-1062, a prodrug of galantamine. Alzheimers Dement (N Y). 2020 Oct 13;6(1):e12093. doi: 10.1002/trc2.12093. eCollection 2020. [Article]
- FDA Approved Drug Products: Zunveyl (benzgalantamine) delayed-release tablets for oral use [Link]
- Fierce Pharma: Alpha Cognition’s delayed-release Alzheimer’s drug Zunveyl passes muster with FDA [Link]
- Alpha Cognition: Corporate Presentation Oct 2024 [Link]
External links
- “Benzgalantamine (Code C188656)”. NCI Thesaurus.
| Clinical data | |
|---|---|
| Trade names | Zunveyl |
| Other names | ALPHA-1062 |
| AHFS/Drugs.com | Zunveyl |
| License data | US DailyMed: Benzgalantamine |
| Routes of administration | By mouth |
| Drug class | Cholinesterase inhibitor |
| ATC code | None |
| Legal status | |
| Legal status | US: ℞-only[1] |
| Identifiers | |
| CAS Number | 224169-27-11542321-58-3 |
| DrugBank | DB19353 |
| UNII | XOI2Q0ZF7GLN7PMJ4P57 |
| KEGG | D12930D12931 |
| ChEMBL | ChEMBL5095056 |
| Chemical and physical data | |
| Formula | C24H25NO4 |
| Molar mass | 391.467 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| showSMILES | |
//////////BENZGALANTAMINE, Alpha 1062, GLN 1062, Memogain, FDA 2024, APPROVALS 2024, Zunveyl
Tisolagiline


Tisolagiline
CAS 1894207-44-3
PCH79KLX33
(2S)-2-[[4-[4-(trifluoromethyl)phenyl]phenyl]methylamino]propanamide
322.32 g/mol
SCHEME
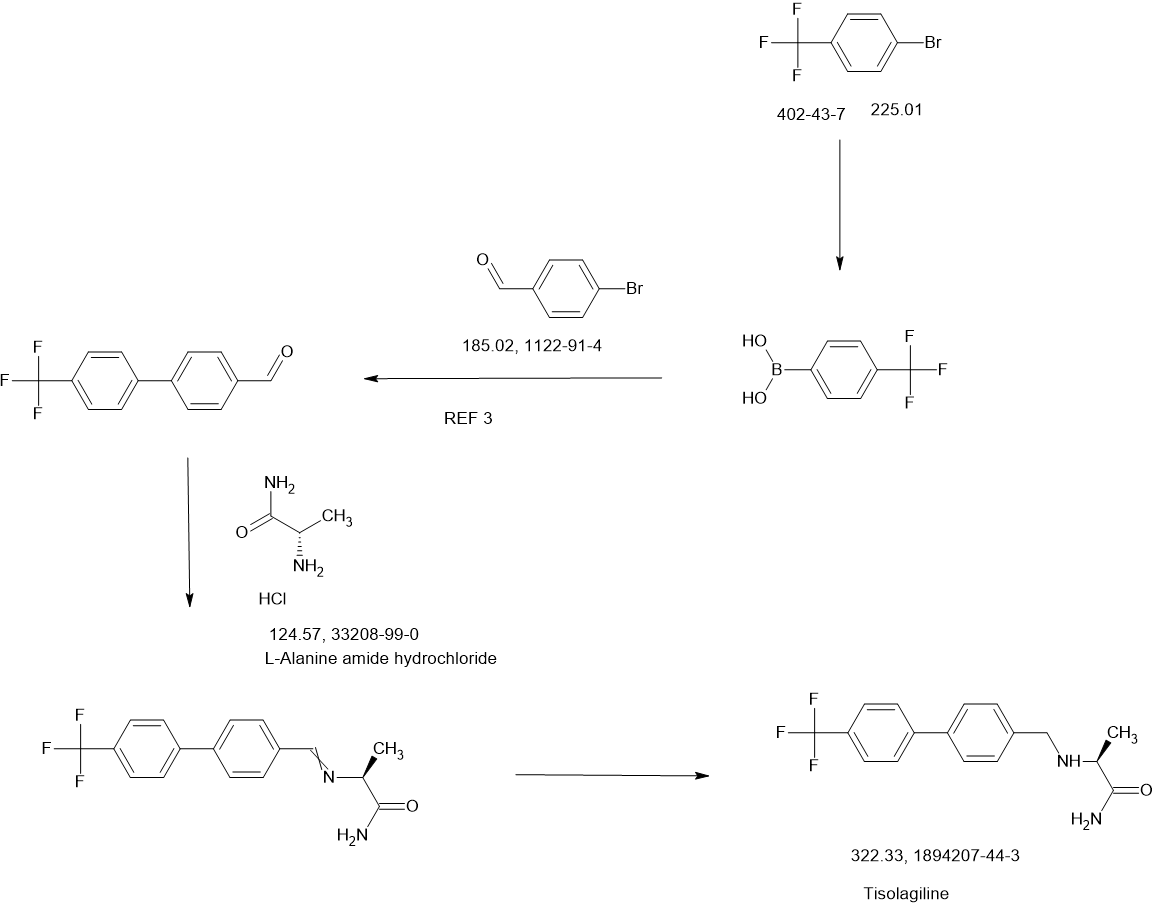
Tisolagiline (INNTooltip International Nonproprietary Name; developmental code names KDS-2010, SeReMABI) is a potent, highly selective, and reversible monoamine oxidase B (MAO-B) inhibitor which is under development for the treatment of Alzheimer’s disease and obesity.[1][2][3][4] It is taken by mouth.[1] Tisolagiline is being developed by NEUROBiOGEN and Scilex Bio.[1][2] As of December 2024, it is in phase 2 clinical trials for Alzheimer’s disease and obesity.[1][2]
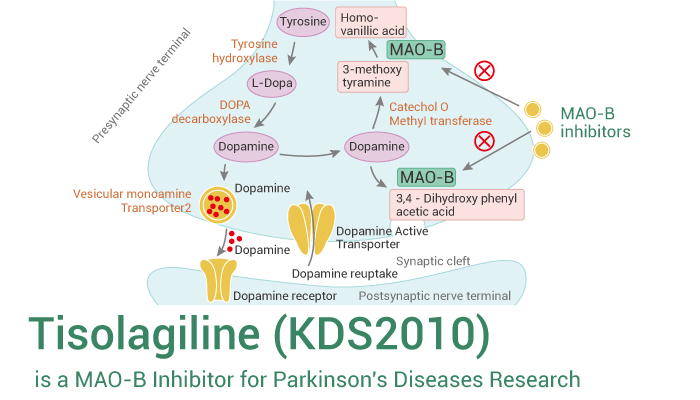
Parkinson’s disease is a progressive disease that ranks second among degenerative neurological diseases, and the incidence rate is estimated to be about 6.3 million patients worldwide, and about 1 in 1,000 people develop Parkinson’s disease. The incidence rate is usually higher in the elderly, but it is now developing in young people as well. Parkinson’s disease is not easy to distinguish from other diseases because the symptoms progress slowly, and it is difficult to detect in the early stages. Clinical characteristics include tremors, rigidity, bradykinesia, postural instability, stooped posture, freezing of gait, depression, sleep disorders, urination disorders, and dementia.
[3]Parkinson’s disease has an unknown cause, but it is known to be a disease that occurs when nerve cells that secrete the neurotransmitter dopamine in the brain are destroyed, resulting in a lack of dopamine. The most widely developed and used drug is levodopa therapy, which is generally administered by administering levodopa, which is converted into dopamine in the body. Levodopa is the most effective treatment for Parkinson’s disease, but there are cases where the drug-related effects decrease or various movement disorders occur during the treatment process. Other drugs used include COMT inhibitors and MAO-B inhibitors, which suppress dopamine metabolism and maintain the concentration of dopamine in the brain.
[4]MAO-B is known to play an important role in dopamine metabolism in the brain and to suppress damage to brain neurons. Although there is no clear evidence that MAO-B inhibitors actually slow down the progression of Parkinson’s disease, it is known that inhibiting MAO-B has an effect of suppressing degeneration or death of dopamine neurons, as it plays an important role in the development of Parkinson’s disease caused by MPTP or similar environmental toxicants. In addition, evidence from animal and clinical trials suggests that MAO-B inhibitors have a brain protective effect, unlike other drugs.
[5]The most representative MAO-B inhibitor approved is selegiline, which is prescribed as a treatment for Parkinson’s disease, but when taken, it is metabolized into amphetamine in the body, causing liver toxicity, and as an irreversible inhibitor, it has various side effects. Azilect, which contains rasagiline, was first marketed in Israel in 2005 and has recently been released in about 50 countries including Europe and the United States. Azilect does not have amphetamine side effects in the body when taken and is said to be more effective than other dopaminergic drugs. However, rasagiline, like selegiline, is an irreversible MAO-B inhibitor, so although it has an excellent MAO-B inhibition effect, it has the disadvantage of safety issues. Therefore, recently, drugs that are effective and can reversibly inhibit activity are being developed as alternatives to complement these shortcomings, but no notable reversible inhibitors have been prescribed to date.
[6]Meanwhile, obesity is a medical condition in which excessive fat accumulates in the body to the extent that it has a negative impact on health. Excessive weight can appear in combination with various diseases as the remaining energy is accumulated excessively due to the difference between energy consumed and energy used.
[7]Previous studies on the hypothalamus in relation to food regulation have focused on neurons that make up a portion of the brain, which has limited our understanding of the brain’s function in controlling food and obesity. Therefore, in order to comprehensively understand brain function, studies on glial cells, which make up the majority, must also be conducted in parallel. In addition, astrocytes, which are the most numerous among glial cells, have recently emerged as cells that can activate or inhibit surrounding neurons by secreting various signaling substances such as GABA (gamma-aminobutyric acid), glutamate, D-serine, and ATP. Astrocytes in the hypothalamus also interact closely with POMC (pro-opiomelanocortin) neurons and express leptin receptors, which can contribute to leptin signaling.
[8]There are two groups of POMC neurons in the hypothalamus: those that induce appetite reduction and those that induce energy consumption. Under normal circumstances, astrocytes help activate nearby POMC neurons that induce energy consumption. However, in obese states, unlike normal astrocytes, they are transformed into reactive astrocytes due to excessive leptin signals, and putrescine is converted into GABA by MAO-B (mono-aminoxidase B) and secreted. In addition, POMC neurons that induce energy consumption express GABAa receptors outside the synapse containing a4, a5, and a6 subunits due to excessive leptin signals, and are affected by persistent GABA secreted from anti-responsive astrocytes. As a result, POMC neurons are inhibited, energy consumption is reduced, and fat accumulation occurs.
[9]At this time, if MAOBI, the causal enzyme of GABA production, is inhibited, GABA production and secretion are inhibited, the inhibition of POMC neurons is relieved, and they are reactivated to promote energy consumption. However, POMC neurons that induce appetite reduction do not express GABAa receptors outside the synapse, so they are not continuously affected by GABA. Therefore, MAOBI inhibitors selectively act on POMC neurons that induce energy consumption and exhibit the effect of obesity treatment. However, most of the existing MAOBI inhibitors are irreversible inhibitors, and there is a problem that they are accompanied by various side effects. Accordingly, drugs that can reversibly inhibit MAOBI are being researched and developed, but no notable reversible MAOBI inhibitor that can effectively act on obesity has been prescribed to date.
REF
Regulatory Toxicology and Pharmacology (2020), 117, 104733
Toxicological Research (Cham, Switzerland) (2023), 39(4), 693-709
Combinatorial Chemistry & High Throughput Screening (2020), 23(9), 836-841
KR2023027416,
WO2023022256
WO2023022256
WO2016052928
PATENT
WO2016052928
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2016052928&_cid=P20-M8XX0L-81795-1


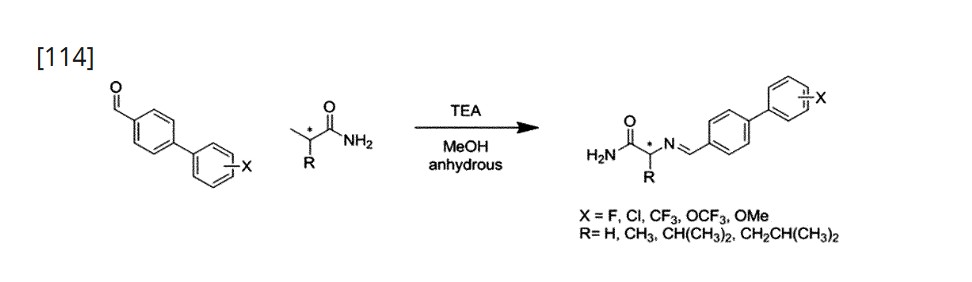
Using L-Alaninamide hydrochloride or D-Alaninamide hydrochloride, a reductive amination reaction was performed with the compound of step (a) to obtain an imine compound (step b, reaction scheme 1b), which was then reduced with sodium cyanoborohydride to obtain an amine compound (step c, reaction scheme 1c).
[112]Add 1.2 equivalents of Glycinamide hydrochloride or L-Alaninamide hydrochloride or D-Alaninamide hydrochloride or L-Valinamide hydrochloride or L-Leucinamide hydrochloride to anhydrous methanol at a concentration of 0.92 molar, and then add 1.5 equivalents of triethylamine. When the solution becomes transparent, add 1.0 equivalent of the aldehyde synthesized in step (a). After two hours, wash with ethyl acetate and distilled water. Dry the organic layer with sodium sulfate and concentrate in vacuo. Dissolve the concentrated reaction solution in anhydrous methanol at a concentration of 1.0 molar, and add 4.0 equivalents of sodium cyanoborohydride at 0 ℃. Then, react at room temperature for 18 hours, and after completion of the reaction, wash the reaction solution with ethyl acetate and distilled water. The organic layer was dried over sodium sulfate, concentrated in vacuo, and separated and purified using silica gel column chromatography.
References
- ^ Jump up to:a b c d “KDS 2010”. AdisInsight. 6 February 2025. Retrieved 24 February 2025.
- ^ Jump up to:a b c “Delving into the Latest Updates on KDS-2010 with Synapse”. Synapse. 23 January 2025. Retrieved 24 February 2025.
- ^ Nam MH, Sa M, Ju YH, Park MG, Lee CJ (April 2022). “Revisiting the Role of Astrocytic MAOB in Parkinson’s Disease”. International Journal of Molecular Sciences. 23 (8): 4453. doi:10.3390/ijms23084453. PMC 9028367. PMID 35457272.
4.4. KDS2010 A recently developed KDS2010, which is ~12,500-fold more selective to MAOB than MAOA, differentiates the role of MAOB from MAOA and reports that MAOB does not contribute to DA degradation [39]. KDS2010 is a potent (IC50 = 7.6 nM), and selective MAOB inhibitor named shows no known off-target effect (no other enzymes or channels causing >40% inhibition) or toxicity for 4 weeks of repeated dosing in non-human primates [16,41]. KDS2010 was turned out to be highly effective for alleviating the PD-related motor symptoms and PD-like pathology, including reactive astrogliosis, excessive astrocytic GABA, and nigrostriatal DAergic neuronal loss in multiple rodent models of PD [41]. Its clinical efficacy is still waiting to be tested in future studies.
- ^ Duarte P, Cuadrado A, León R (2021). “Monoamine Oxidase Inhibitors: From Classic to New Clinical Approaches”. Handbook of Experimental Pharmacology. 264: 229–259. doi:10.1007/164_2020_384. ISBN 978-3-030-68509-6. PMID 32852645.
KDS2010 is a novel compound highly potent and selective reversible MAO-B inhibitor (Fig. 2). It has demonstrated learning and memory improvements, promotion of synaptic transmission, and reduction of astrogliosis and astrocytic GABA levels in APP/presenilin 1 mice (Park et al. 2019).
| Clinical data | |
|---|---|
| Other names | KDS-2010; KDS2010; SeReMABI |
| Drug class | Reversible monoamine oxidase B (MAO-B) inhibitor |
| Identifiers | |
| showIUPAC name | |
| CAS Number | 1894207-44-3 |
| PubChem CID | 132023446 |
| ChemSpider | 128942408 |
| UNII | PCH79KLX33 |
| ChEMBL | ChEMBL5314546 |
| Chemical and physical data | |
| Formula | C17H17F3N2O |
| Molar mass | 322.331 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| showSMILES | |
| showInChI | |
///////////Tisolagiline, PCH79KLX33

{kind=link}
{kind=link}