
Home » Posts tagged 'antiobesity'
Tag Archives: antiobesity
 DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HERE
DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HEREFlag and hits
ORGANIC SPECTROSCOPY

SUBSCRIBE

 Subscribe in a reader
Subscribe in a reader
Enter your email address:
Delivered by FeedBurner
Subscribe to New Drug Approvals by Email![]()

![]()



![]()
![]()





Recent Comments
| shivkr2 on SPSR Excellence Award 2025 – S… | |
| Bonkasaurus on Infigratinib phosphate | |
| PALOVAROTENE | ORGAN… on Palovarotene | |
| Pfizer just purchase… on Temanogrel | |
| Pfizer To Cash In On… on Temanogrel |
Setmelanotide


Setmelanotide
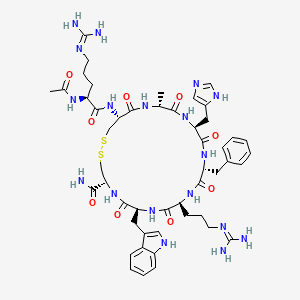
Ac-Arg-Cys(1)-D-Ala-His-D-Phe-Arg-Trp-Cys(1)-NH2
- Molecular FormulaC49H68N18O9S2
- Average mass1117.309 Da
- N-acetyl-L-arginyl-L-cysteinyl-D-alanyl-L-histidyl-D-phenylalanyl-L-arginyl-L-tryptophyl-L-cysteinamide (2->8)-disulfide
1,2-Dithia-5,8,11,14,17,20-hexaazacyclotricosane-4-carboxamide, 22-[[(2S)-2-(acetylamino)-5-[(diaminomethylene)amino]-1-oxopentyl]amino]-10-[3-[(diaminomethylene)amino]propyl]-16-(1H-imidazol-5-ylmeth yl)-7-(1H-indol-3-ylmethyl)-19-methyl-6,9,12,15,18,21-hexaoxo-13-(phenylmethyl)-, (4R,7S,10S,13R,16S,19R,22R)- [ACD/Index Name]10011920014-72-8[RN]Imcivree [Trade name]N2-acetyl-L-arginyl-L-cysteinyl-D-alanyl-L-histidyl-D-phenylalanyl-L-arginyl-Ltryptophyl- L-cysteinamide, cyclic (2-8)-disulfideN7T15V1FUYRM-493, BIM-22493UNII-N7T15V1FUYсетмеланотид [Russian] [INN]سيتميلانوتيد [Arabic] [INN]司美诺肽 [Chinese] [INN](4R,7S,10S,13R,16S,19R,22R)-22-[[(2S)-2-acetamido-5-(diaminomethylideneamino)pentanoyl]amino]-13-benzyl-10-[3-(diaminomethylideneamino)propyl]-16-(1H-imidazol-5-ylmethyl)-7-(1H-indol-3-ylmethyl)-19-methyl-6,9,12,15,18,21-hexaoxo-1,2-dithia-5,8,11,14,17,20-hexazacyclotricosane-4-carboxamide
FDA 11/25/2020, Imcivree, To treat obesity and the control of hunger associated with pro-opiomelanocortin deficiency, a rare disorder that causes severe obesity that begins at an early age
Drug Trials Snapshot, 10MG/ML, SOLUTION;SUBCUTANEOUS, Orphan


update Imcivree EMA APPROVED 2021/7/16
DESCRIPTION
IMCIVREE contains setmelanotide acetate, a melanocortin 4 (MC4) receptor agonist. Setmelanotide is an 8 amino acid cyclic peptide analog of endogenous melanocortin peptide α-MSH (alpha-melanocyte stimulating hormone).
The chemical name for setmelanotide acetate is acetyl-L-arginyl-L-cysteinyl-D-alanyl-Lhistidinyl-D-phenylalanyl-L-arginyl-L-tryptophanyl-L-cysteinamide cyclic (2→8)-disulfide acetate. Its molecular formula is C49H68N18O9S2 (anhydrous, free-base), and molecular mass is 1117.3 Daltons (anhydrous, free-base).
The chemical structure of setmelanotide is:
 |
IMCIVREE injection is a sterile clear to slightly opalescent, colorless to slightly yellow solution. Each 1 mL of IMCIVREE contains 10 mg of setmelanotide provided as setmelanotide acetate, which is a salt with 2 to 4 molar equivalents of acetate, and the following inactive ingredients: 100 mg N-(carbonyl-methoxypolyethylene glycol 2000)-1,2-distearoyl-glycero-3phosphoethanolamine sodium salt, 8 mg carboxymethylcellulose sodium (average MWt 90,500), 11 mg mannitol, 5 mg phenol, 10 mg benzyl alcohol, 1 mg edetate disodium dihydrate, and Water for Injection. The pH of IMCIVREE is 5 to 6.
Setmelanotide is a peptide drug and investigational anti-obesity medication which acts as a selective agonist of the MC4 receptor. Setmelanotide binds to and activates MC4 receptors in the paraventricular nucleus (PVN) of the hypothalamus and in the lateral hypothalamic area (LHA), areas involved in the regulation of appetite, and this action is thought to underlie its appetite suppressant effects. Setmelanotide increases resting energy expenditure in both obese animals and humans. Setmelanotide has been reported to possess the following activity profile (cAMP, EC50): MC4 (0.27 nM) > MC3 (5.3 nM) ≈ MC1 (5.8 nM) > MC5 (1600 nM) ≟ MC2 (>1000 nM).
Setmelanotide, sold under the brand name Imcivree, is a medication for the treatment of obesity.[1]
The most common side effects include injection site reactions, skin hyperpigmentation (skin patches that are darker than surrounding skin), headache and gastrointestinal side effects (such as nausea, diarrhea, and abdominal pain), among others.[1] Spontaneous penile erections in males and adverse sexual reactions in females have occurred with treatment.[1] Depression and suicidal ideation have also occurred with setmelanotide.[1]
SYN
WO 2011060355



Medical uses
Setmelanotide is indicated for chronic weight management (weight loss and weight maintenance for at least one year) in people six years and older with obesity due to three rare genetic conditions: pro-opiomelanocortin (POMC) deficiency, proprotein subtilisin/kexin type 1 (PCSK1) deficiency, and leptin receptor (LEPR) deficiency confirmed by genetic testing demonstrating variants in POMC, PCSK1, or LEPR genes considered pathogenic (causing disease), likely pathogenic, or of uncertain significance.[1] Setmelanotide is the first FDA-approved treatment for these genetic conditions.[1]
Setmelanotide is not approved for obesity due to suspected POMC, PCSK1, or LEPR deficiency with variants classified as benign (not causing disease) or likely benign or other types of obesity, including obesity associated with other genetic syndromes and general (polygenic) obesity.[1]
Setmelanotide binds to and activates MC4 receptors in the paraventricular nucleus (PVN) of the hypothalamus and in the lateral hypothalamic area (LHA), areas involved in the regulation of appetite, and this action is thought to underlie its appetite suppressant effects.[2] In addition to reducing appetite, setmelanotide increases resting energy expenditure in both obese animals and humans.[3] Importantly, unlike certain other MC4 receptor agonists, such as LY-2112688, setmelanotide has not been found to produce increases in heart rate or blood pressure.[4]
Setmelanotide has been reported to possess the following activity profile (cAMP, EC50): MC4 (0.27 nM) > MC3 (5.3 nM) ≈ MC1 (5.8 nM) > MC5 (1600 nM) ≟ MC2 (>1000 nM).[5] (19.6-fold selectivity for MC4 over MC3, the second target of highest activity.)
History
Setmelanotide was evaluated in two one-year studies.[1] The first study enrolled participants with obesity and confirmed or suspected POMC or PCSK1 deficiency while the second study enrolled participants with obesity and confirmed or suspected LEPR deficiency; all participants were six years or older.[1] The effectiveness of setmelanotide was determined by the number of participants who lost more than ten percent of their body weight after a year of treatment.[1]
The effectiveness of setmelanotide was assessed in 21 participants, ten in the first study and eleven in the second.[1] In the first study, 80 percent of participants with POMC or PCSK1 deficiency lost ten percent or more of their body weight.[1] In the second study, 46 percent of participants with LEPR deficiency lost ten percent or more of their body weight.[1]
The study also assessed the maximal (greatest) hunger in sixteen participants over the previous 24 hours using an eleven-point scale in participants twelve years and older.[1] In both studies, some, but not all, of participants’ weekly average maximal hunger scores decreased substantially from their scores at the beginning of the study.[1] The degree of change was highly variable among participants.[1]
The U.S. Food and Drug Administration (FDA) granted the application for setmelanotide orphan disease designation, breakthrough therapy designation, and priority review.[1] The FDA granted the approval of Imcivree to Rhythm Pharmaceutical, Inc.[1]
Research
Setmelanotide is a peptide drug and investigational anti-obesity medication which acts as a selective agonist of the MC4 receptor.[6][4] Its peptide sequence is Ac-Arg-Cys(1)-D-Ala-His-D-Phe-Arg-Trp-Cys(1)-NH2. It was first discovered at Ipsen and is being developed by Rhythm Pharmaceuticals for the treatment of obesity and diabetes.[6] In addition, Rhythm Pharmaceuticals is conducting trials of setmelanotide for the treatment of Prader–Willi syndrome (PWS), a genetic disorder which includes MC4 receptor deficiency and associated symptoms such as excessive appetite and obesity.[7] As of December 2014, the drug is in phase II clinical trials for obesity and PWS.[6][8][9][needs update] So far, preliminary data has shown no benefit of Setmelanotide in Prader-Willi syndrome.[10]
PATENT
WO 2007008704
WO 2011060355
WO 2011060352
US 20120225816
PAPER
Journal of Medicinal Chemistry, 61(8), 3674-3684; 2018
PATENT
https://patents.google.com/patent/US9314509
Synthesis of Example 1i.e., Ac-Arg-cyclo(Cys-D-Ala-His-D-Phe-Arg-Trp-Cys)-NH2

The title peptide having the above structure was assembled using Fmoc chemistry on an Apex peptide synthesizer (Aapptec; Louisville, Ky., USA). 220 mg of 0.91 mmol/g (0.20 mmoles) Rink Amide MBHA resin (Polymer Laboratories; Amherst, Mass., USA) was placed in a reaction well and pre-swollen in 3.0 mL of DMF prior to synthesis. For cycle 1, the resin was treated with two 3-mL portions of 25% piperidine in DMF for 5 and 10 minutes respectively, followed by 4 washes of 3-mL DMF—each wash consisting of adding 3 mL of solvent, mixing for 1 minute, and emptying for 1 minute. Amino acids stocks were prepared in NMP as 0.45M solutions containing 0.45M HOBT. HBTU was prepared as a 0.45M solution in NMP and DIPEA was prepared as a 2.73M solution in NMP. To the resin, 2 mL of the first amino acid (0 9 mmoles, Fmoc-Cys(Trt)-OH) (Novabiochem; San Diego, Calif., USA) was added along with 2 mL (0.9 mmoles) of HBTU and 1.5 mL (4.1 mmoles) of DIPEA. After one hour of constant mixing, the coupling reagents were drained from the resin and the coupling step was repeated. Following amino acid acylation, the resin was washed with two 3-mL aliquots of DMF for 1 minute. The process of assembling the peptide (deblock/wash/acylate/wash) was repeated for cycles 2-9 identical to that as described for cycle 1. The following amino acids were used: cycle 2) Fmoc-Trp(Boc)-OH (Genzyme; Cambridge, Mass., USA); cycle 3) Fmoc-Arg(Pbf)-OH (Novabiochem); cycle 4) Fmoc-DPhe-OH (Genzyme); cycle 5) Fmoc-His(Trt)-OH (Novabiochem); cycle 6) Fmoc-D-Ala-OH (Genzyme); cycle 7) Fmoc-Cys(Trt)-OH, (Novabiochem); and cycle 8) Fmoc-Arg(Pbf)-OH (Genzyme). The N-terminal Fmoc was removed with 25% piperidine in DMF as described above, followed by four 3-mL DMF washes for 1 minute. Acetylation of the N-terminus was performed by adding 0.5 mL of 3M DIPEA in NMP to the resin along with 1.45 mL of 0.45M acetic anhydride in NMP. The resin was mixed for 30 minutes and acetylation was repeated. The resin was washed with 3 mL of DMF for a total of 5 times followed with 5 washes with 5 mL of DCM each.
To cleave and deprotect the peptide, 5mL of the following reagent was added to the resin: 2% TIS/5% water/5% (w/v) DTT/88% TFA. The solution was allowed to mix for 3.5 hours. The filtrate was collected into 40 mL of cold anhydrous ethyl ether. The precipitate was pelleted for 10 minutes at 3500 rpm in a refrigerated centrifuge. The ether was decanted and the peptide was re-suspended in fresh ether. The ether workup was performed three times. Following the last ether wash, the peptide was allowed to air dry to remove residual ether.
The peptide was dissolved in 10% acetonitrile and analyzed by mass spectrometry and reverse-phase HPLC employing a 30×4.6 cm C18 column (Vydac; Hesperia, Calif., USA) with a gradient of 2-60% acetonitrile (0.1% TFA) over 30 minutes. This analysis identified a product with ˜53% purity. Mass analysis employing electrospray ionization identified a main product containing a mass of 1118.4 corresponding to the desired linear product. The crude product (˜100 mg) was diluted to a concentration of 2 mg/mL in 5% acetic acid. To this solution, 0.5M iodine/methanol was added dropwise with vigorous stirring until a pale yellow color was achieved. The solution was vigorously stirred for another 10 minutes. Excess iodine was then quenched by adding 1.0M sodium thiosulfate under continuous mixing until the mixture was rendered colorless. The peptide was re-examined by mass spectrometry analysis and HPLC. Mass spectrometry analysis identified a main species with a mass of 1116.4 which indicated successful oxidation to form the cyclic peptide. The peptide solution was purified on a preparative HPLC equipped with a C18 column using a similar elution gradient. The purified product was re-analyzed by HPLC for purity (>95%) and mass spectrometry (1116.9 which is in agreement with the expected mass of 1117.3) and subsequently lyophilized. Following lyophilization, 28 mg of purified product was obtained representing a 24% yield.
The other exemplified peptides were synthesized substantially according to the procedure described for the above-described synthetic process. Physical data for select exemplified peptides are given in Table 1.
TABLE 1 Example Mol. Wt. Mol. Wt. Purity Number (calculated) (ES-MS) (HPLC) 1 1117.3 1116.9 95.1% 2 1117.3 1116.8 99.2% 3 1280.5 1280.6 98.0% 5 1216.37 1216.20 99.9%
Preparation of Pamoate Salt of Example 1
The acetate salt of Example 1 (200 mg, 0.18 mmole) was dissolved in 10 mL of water. Sodium pamoate (155 mg, 0.36 mmole) was dissolved in 10 mL of water. The two solutions were combined and mixed well. The precipitates were collected by centrifugation at 3000 rpm for 20 minutes, washed for three times with water, and dried by lyophilization.
References
- ^ Jump up to:a b c d e f g h i j k l m n o p q r “FDA approves first treatment for weight management for people with certain rare genetic conditions”. U.S. Food and Drug Administration (FDA) (Press release). 27 November 2020. Retrieved 27 November 2020.
 This article incorporates text from this source, which is in the public domain.
This article incorporates text from this source, which is in the public domain. - ^ Kim GW, Lin JE, Blomain ES, Waldman SA (January 2014). “Antiobesity pharmacotherapy: new drugs and emerging targets”. Clinical Pharmacology and Therapeutics. 95 (1): 53–66. doi:10.1038/clpt.2013.204. PMC 4054704. PMID 24105257.
- ^ Chen KY, Muniyappa R, Abel BS, Mullins KP, Staker P, Brychta RJ, et al. (April 2015). “RM-493, a melanocortin-4 receptor (MC4R) agonist, increases resting energy expenditure in obese individuals”. The Journal of Clinical Endocrinology and Metabolism. 100 (4): 1639–45. doi:10.1210/jc.2014-4024. PMC 4399297. PMID 25675384.
- ^ Jump up to:a b Kievit P, Halem H, Marks DL, Dong JZ, Glavas MM, Sinnayah P, et al. (February 2013). “Chronic treatment with a melanocortin-4 receptor agonist causes weight loss, reduces insulin resistance, and improves cardiovascular function in diet-induced obese rhesus macaques”. Diabetes. 62 (2): 490–7. doi:10.2337/db12-0598. PMC 3554387. PMID 23048186.
- ^ Muniyappa R, Chen K, Brychta R, Abel B, Mullins K, Staker P, et al. (June 2014). “A Randomized, Double-Blind, Placebo-Controlled, Crossover Study to Evaluate the Effect of a Melanocortin Receptor 4 (MC4R) Agonist, RM-493, on Resting Energy Expenditure (REE) in Obese Subjects” (PDF). Endocrine Reviews. Rhythm Pharmaceuticals. 35 (3). Retrieved 2015-05-21.
- ^ Jump up to:a b c Lee EC, Carpino PA (2015). “Melanocortin-4 receptor modulators for the treatment of obesity: a patent analysis (2008-2014)”. Pharmaceutical Patent Analyst. 4 (2): 95–107. doi:10.4155/ppa.15.1. PMID 25853469.
- ^ “Obesity and Diabetes Caused by Genetic Deficiencies in the MC4 Pathway”. Rhythm Pharmaceuticals. Retrieved 2015-05-21.
- ^ Jackson VM, Price DA, Carpino PA (August 2014). “Investigational drugs in Phase II clinical trials for the treatment of obesity: implications for future development of novel therapies”. Expert Opinion on Investigational Drugs. 23 (8): 1055–66. doi:10.1517/13543784.2014.918952. PMID 25000213. S2CID 23198484.
- ^ “RM-493: A First-in-Class, Phase 2-Ready MC4 Agonist: A New Drug Class for the Treatment of Obesity and Diabetes”. Rhythm Pharmaceuticals. Archived from the original on 2015-06-14. Retrieved 2015-05-21.
- ^ Duis J, van Wattum PJ, Scheimann A, Salehi P, Brokamp E, Fairbrother L, et al. (March 2019). “A multidisciplinary approach to the clinical management of Prader-Willi syndrome”. Molecular Genetics & Genomic Medicine. 7 (3): e514. doi:10.1002/mgg3.514. PMC 6418440. PMID 30697974.
ADDITIONAL INFORMATION
The peptide sequence is Ac-Arg-Cys(1)-D-Ala-His-D-Phe-Arg-Trp-Cys(1)-NH2. It is being researched by Rhythm Pharmaceuticals for the treatment of obesity and diabetes. In addition, Rhythm Pharmaceuticals is conducting trials of setmelanotide for the treatment of Prader–Willi syndrome (PWS), a genetic disorder which includes MC4 receptor deficiency and associated symptoms such as excessive appetite and obesity. As of December 2014, the drug is in phase II clinical trials for obesity and PWS.
L-Cysteinamide, N2-acetyl-L-arginyl-L-cysteinyl-D-alanyl-L-histidyl-D-phenylalanyl-L-arginyl-L-tryptophyl-, cyclic (2->8)-disulfide
Ac-Arg-Cys(1)-D-Ala-His-D-Phe-Arg-Trp-Cys(1)-NH2
REFERENCES
1: Lee EC, Carpino PA. Melanocortin-4 receptor modulators for the treatment of obesity: a patent analysis (2008-2014). Pharm Pat Anal. 2015;4(2):95-107. doi: 10.4155/ppa.15.1. PubMed PMID: 25853469.
2: Chen KY, Muniyappa R, Abel BS, Mullins KP, Staker P, Brychta RJ, Zhao X, Ring M, Psota TL, Cone RD, Panaro BL, Gottesdiener KM, Van der Ploeg LH, Reitman ML, Skarulis MC. RM-493, a melanocortin-4 receptor (MC4R) agonist, increases resting energy expenditure in obese individuals. J Clin Endocrinol Metab. 2015 Apr;100(4):1639-45. doi: 10.1210/jc.2014-4024. Epub 2015 Feb 12. PubMed PMID: 25675384; PubMed Central PMCID: PMC4399297.
3: Clemmensen C, Finan B, Fischer K, Tom RZ, Legutko B, Sehrer L, Heine D, Grassl N, Meyer CW, Henderson B, Hofmann SM, Tschöp MH, Van der Ploeg LH, Müller TD. Dual melanocortin-4 receptor and GLP-1 receptor agonism amplifies metabolic benefits in diet-induced obese mice. EMBO Mol Med. 2015 Feb 4;7(3):288-98. doi: 10.15252/emmm.201404508. PubMed PMID: 25652173; PubMed Central PMCID: PMC4364946.
4: Jackson VM, Price DA, Carpino PA. Investigational drugs in Phase II clinical trials for the treatment of obesity: implications for future development of novel therapies. Expert Opin Investig Drugs. 2014 Aug;23(8):1055-66. doi: 10.1517/13543784.2014.918952. Epub 2014 Jul 7. Review. PubMed PMID: 25000213.
5: Kievit P, Halem H, Marks DL, Dong JZ, Glavas MM, Sinnayah P, Pranger L, Cowley MA, Grove KL, Culler MD. Chronic treatment with a melanocortin-4 receptor agonist causes weight loss, reduces insulin resistance, and improves cardiovascular function in diet-induced obese rhesus macaques. Diabetes. 2013 Feb;62(2):490-7. doi: 10.2337/db12-0598. Epub 2012 Oct 9. PubMed PMID: 23048186; PubMed Central PMCID: PMC3554387.
6: Kumar KG, Sutton GM, Dong JZ, Roubert P, Plas P, Halem HA, Culler MD, Yang H, Dixit VD, Butler AA. Analysis of the therapeutic functions of novel melanocortin receptor agonists in MC3R- and MC4R-deficient C57BL/6J mice. Peptides. 2009 Oct;30(10):1892-900. doi: 10.1016/j.peptides.2009.07.012. Epub 2009 Jul 29. PubMed PMID: 19646498; PubMed Central PMCID: PMC2755620.
External links
- “Setmelanotide”. Drug Information Portal. U.S. National Library of Medicine.
| Clinical data | |
|---|---|
| Trade names | Imcivree |
| Other names | RM-493; BIM-22493; IRC-022493; N2-Acetyl-L-arginyl-L-cysteinyl-D-alanyl-L-histidyl-D-phenylalanyl-L-arginyl-L-tryptophyl-L-cysteinamide, cyclic (2-8)-disulfide |
| ATC code | None |
| Legal status | |
| Legal status | US: ℞-only |
| Identifiers | |
| IUPAC name[show] | |
| CAS Number | 920014-72-8 |
| PubChem CID | 11993702 |
| ChemSpider | 10166169 |
| UNII | N7T15V1FUY |
| KEGG | D11927 |
| Chemical and physical data | |
| Formula | C49H68N18O9S2 |
| Molar mass | 1117.32 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| SMILES[hide]C[C@@H]1C(=O)N[C@H](C(=O)N[C@@H](C(=O)N[C@H](C(=O)N[C@H](C(=O)N[C@@H](CSSC[C@@H](C(=O)N1)NC(=O)[C@H](CCCN=C(N)N)NC(=O)C)C(=O)N)Cc2c[nH]c3c2cccc3)CCCN=C(N)N)Cc4ccccc4)Cc5cnc[nH]5 | |
| InChI[hide]InChI=1S/C49H68N18O9S2/c1-26-41(70)63-37(20-30-22-55-25-59-30)46(75)64-35(18-28-10-4-3-5-11-28)44(73)62-34(15-9-17-57-49(53)54)43(72)65-36(19-29-21-58-32-13-7-6-12-31(29)32)45(74)66-38(40(50)69)23-77-78-24-39(47(76)60-26)67-42(71)33(61-27(2)68)14-8-16-56-48(51)52/h3-7,10-13,21-22,25-26,33-39,58H,8-9,14-20,23-24H2,1-2H3,(H2,50,69)(H,55,59)(H,60,76)(H,61,68)(H,62,73)(H,63,70)(H,64,75)(H,65,72)(H,66,74)(H,67,71)(H4,51,52,56)(H4,53,54,57)/t26-,33+,34+,35-,36+,37+,38+,39+/m1/s1Key:HDHDTKMUACZDAA-PHNIDTBTSA-N |
///////////Setmelanotide, FDA 2020, 2020 APPROVALS, Imcivree, Orphan, PEPTIDE, ANTIOBESITY, UNII-N7T15V1FUY, сетмеланотид , سيتميلانوتيد , 司美诺肽 , BIM 22493, RM 493
CC1C(=O)NC(C(=O)NC(C(=O)NC(C(=O)NC(C(=O)NC(CSSCC(C(=O)N1)NC(=O)C(CCCN=C(N)N)NC(=O)C)C(=O)N)CC2=CNC3=CC=CC=C32)CCCN=C(N)N)CC4=CC=CC=C4)CC5=CN=CN5
Ayurveda- Obesity control

Currently, Indian anti-obesity drug market is bifurcated into prescription and non-prescription. Amongst the prescription anti-obesity drug market there is only one drug – Orlistat that is been used globally. While the other anti-obesity drugs, Rimonabant and Sibutramine were banned by Indian government in 2009 and 2010 as side-effects were found in those drugs.
According to the experts, the market size of anti-obesity for prescription drug (generic Orlistat) is Rs 40 crore. While market size of non-prescription drug mostly herbal and ayurvedic drugs is estimated at Rs 500 crore in India. The global anti-obesity drug market is expected to reach $11 billion by 2017.
Orlistat is originally made by multinational drug company Roche that markets the prescription drug under the brand/trade name Xenical. The drug’s patent protection ended in 2009. Currently, there is plethora of generic drug makers like Ranbaxy, Intas Pharma, Biocon Ltd, Torrent Pharma, Troikaa Pharma and Mankind Pharmaceuticals that makes generic copies of Orlistat in India.
http://ijrap.net/admin/php/uploads/870_pdf.pdf
http://nopr.niscair.res.in/bitstream/123456789/6269/1/IJTK%208(4)%20602-605.pdf
anti obesity drugs
Obesity is a medical condition in which excess body fat has accumulated to the extent that it may have an adverse effect on health, leading to reduced life expectancy and/or increased health problems. Body mass index (BMI), a measurement which compares weight and height, defines people as overweight (pre-obese) when their BMI is between 25 kg/m2 and 30 kg/m2, and obese when it is greater than 30 kg/m
Obesity increases the likelihood of various diseases, particularly heart disease, type 2 diabetes, breathing difficulties during sleep, certain types of cancer, and osteoarthritis. Obesity is most commonly caused by a combination of excessive dietary calories, lack of physical activity, and genetic susceptibility, although a few cases are caused primarily by genes, endocrine disorders, medications or psychiatric illness. Evidence to support the view that some obese people eat little yet gain weight due to a slow metabolism is limited; on average obese people have a greater energy expenditure than their thin counterparts due to the energy required to maintain an increased body mass.
The primary treatment for obesity is dieting and physical exercise. To supplement this, or in case of failure, anti-obesity drugs may be taken to reduce appetite or inhibit fat absorption. In severe cases, surgery is performed or an intragastric balloon is placed to reduce stomach volume and/or bowel length, leading to earlier satiation and reduced ability to absorb nutrients from food.
Obesity is a leading preventable cause of death worldwide, with increasing prevalence in adults and children, and authorities view it as one of the most serious public health problems of the 21st century. Obesity is stigmatized in the modern Western world, though it has been perceived as a symbol of wealth and fertility at other times in history, and still is in many parts of Africa.[
Excessive body weight is associated with various diseases, particularly cardiovascular diseases, diabetes mellitus type 2, obstructive sleep apnea, certain types of cancer, and osteoarthritis. As a result, obesity has been found to reduce life expectancy.
Obesity is one of the leading preventable causes of death worldwide. Large-scale American and European studies have found that mortality risk is lowest at a BMI of 22.5–25 kg/m in non-smokers and at 24–27 kg/m2 in current smokers, with risk increasing along with changes in either direction. A BMI above 32 has been associated with a doubled mortality rate among women over a 16-year period. In the United States obesity is estimated to cause an excess 111,909 to 365,000 death per year, while 1 million (7.7%) of deaths in the European Union are attributed to excess weight On average, obesity reduces life expectancy by six to seven years: a BMI of 30–35 reduces life expectancy by two to four years, while severe obesity (BMI > 40) reduces life expectancy by 10 year
Causes
At an individual level, a combination of excessive caloric intake and a lack of physical activity is thought to explain most cases of obesity. A limited number of cases are due primarily to genetics, medical reasons, or psychiatric illness. In contrast, increasing rates of obesity at a societal level are felt to be due to an easily accessible and palatable diet,[64] increased reliance on cars, and mechanized manufacturing. A 2006 review identified ten other possible contributors to the recent increase of obesity: (1) insufficient sleep, (2) endocrine disruptors (environmental pollutants that interfere with lipid metabolism), (3) decreased variability in ambient temperature, (4) decreased rates of smoking, because smoking suppresses appetite, (5) increased use of medications that can cause weight gain (e.g., atypical antipsychotic), (6) proportional increases in ethnic and age groups that tend to be heavier, (7) pregnancy at a later age (which may cause susceptibility to obesity in children), (8) epigenetic risk factors passed on gene rationally, (9) natural selection for higher BMI, and (10) assortative mating leading to increased concentration of obesity risk factors (this would not necessarily increase the number of obese people, but would increase the average population weight).[67] While there is substantial evidence supporting the influence of these mechanisms on the increased prevalence of obesity, the evidence is still inconclusive, and the authors state that these are probably less influential than the ones discussed in the previous paragraph.
Ways of preventing Obesity
Dieting
Main article: Dieting
Diets to promote weight loss are generally divided into four categories: low-fat, low-carbohydrate, low-calorie, and very low calorie. A meta-analysis of six randomized controlled trials found no difference between three of the main diet types (low calorie, low carbohydrate, and low fat), with a 2–4 kilogram (4.4–8.8 lb) weight loss in all studies. At two years these three methods resulted in similar weight loss irrespective of the macronutrients emphasized.[132]
Very low calorie diets provide 200–800 kcal/day, maintaining protein intake but limiting calories from both fat and carbohydrates. They subject the body to starvation and produce an average weekly weight loss of 1.5–2.5 kilograms (3.3–5.5 lb). These diets are not recommended for general use as they are associated with adverse side effects such as loss of lean muscle mass, increased risks of gout, and electrolyte imbalances. People attempting these diets must be monitored closely by a physician to prevent complications.
Exercise
With use, muscles consume energy derived from both fat and glycogen. Due to the large size of leg muscles, walking, running, and cycling are the most effective means of exercise to reduce body fat. Exercise affects macronutrient balance. During moderate exercise, equivalent to a brisk walk, there is a shift to greater use of fat as a fuel. To maintain health the American Heart Association recommends a minimum of 30 minutes of moderate exercise at least 5 days a week.
A meta-analysis of 43 randomized controlled trials by the Cochrane Collaboration found that exercising alone led to limited weight loss. In combination with diet, however, it resulted in a 1 kilogram weight loss over dieting alone. A 1.5 kilogram (3.3 lb) loss was observed with a greater degree of exercise. Even though exercise as carried out in the general population has only modest effects, a dose response curve is found, and very intense exercise can lead to substantial weight loss. During 20 weeks of basic military training with no dietary restriction, obese military recruits lost 12.5 kg (27.6 lb). High levels of physical activity seem to be necessary to maintain weight loss. A pedometer appears useful for motivation. Over an average of 18-weeks of use physical activity increased by 27% resulting in a 0.38 decreased in BMI.
Signs that encourage the use of stairs as well as community campaigns have been shown to be effective in increasing exercise in a population. The city of Bogota, Colombia for example blocks off 113 kilometers (70 miles) of roads every Sunday and on holidays to make it easier for its citizens to get exercise. These pedestrian zones are part of an effort to combat chronic diseases, including obesity.
Weight loss programs
Weight loss programs often promote lifestyle changes and diet modification. This may involve eating smaller meals, cutting down on certain types of food, and making a conscious effort to exercise more. These programs also enable people to connect with a group of others who are attempting to lose weight, in the hopes that participants will form mutually motivating and encouraging relationships.
A number of popular programs exist, including Weight Watchers, Overeaters Anonymous, and Jenny Craig. These appear to provide modest weight loss (2.9 kg, 6.4 lb) over dieting on one’s own (0.2 kg, 0.4 lb) over a two year period. Internet-based programs appear to be ineffective. The Chinese government has introduced a number of “fat farms” where obese children go for reinforced exercise, and has passed a law which requires students to exercise or play sports for an hour a day at school (see Obesity in China).
Medication
Main article: Anti-obesity medication
The two most commonly used medications to treat obesity: orlistat (Xenical) and sibutramine (Meridia)
Only two anti-obesity medications are currently approved by the FDA for long term use.[147] One is orlistat (Xenical), which reduces intestinal fat absorption by inhibiting pancreatic lipase; the other is sibutramine (Meridia), which acts in the brain to inhibit deactivation of the neurotransmitters norepinephrine, serotonin, and dopamine (very similar to some anti-depressants), therefore decreasing appetite. Rimonabant (Acomplia), a third drug, works via a specific blockade of the endocannabinoid system. It has been developed from the knowledge that cannabis smokers often experience hunger, which is often referred to as “the munchies”. It had been approved in Europe for the treatment of obesity but has not received approval in the United States or Canada due to safety concerns.[148][149] European Medicines Agency in October 2008 recommended the suspension of the sale of rimonabant as the risk seem to be greater than the benefits.
Weight loss with these drugs is modest. Over the longer term, average weight loss on orlistat is 2.9 kg (6.4 lb), sibutramine is 4.2 kg (9.3 lb) and rimonabant is 4.7 kg (10.4 lb). Orlistat and rimonabant lead to a reduced incidence of diabetes, and all three drugs have some effect on cholesterol. However, there is little information on how these drugs affect the longer-term complications or outcomes of obesity. In 2010 the FDA noted concerns that sibutramine increases the risk of heart attacks and strokes in patients with a history of cardiovascular disease.
There are a number of less commonly used medications. Some are only approved for short term use, others are used off-label, and still others are used illegally. Most are appetite suppressants that act on one or more neurotransmitters. Phendimetrazine (Bontril), diethylpropion (Tenuate), and phentermine (Adipex-P) are approved by the FDA for short term use, while bupropion (Wellbutrin), topiramate (Topamax), and zonisamide (Zonegran) are sometimes used off-label.
The usefulness of certain drugs depends upon the comorbities present. Metformin (Glucophage) is preferred in overweight diabetics, as it may lead to mild weight loss in comparison to sulfonylureas or insulin. The thiazolidinediones, on the other hand, may cause weight gain, but decrease central obesity.[155] Diabetics also achieve modest weight loss with fluoxetine (Prozac), orlistat and sibutramine over 12–57 weeks. Preliminary evidence has however found higher number of cardiovascular events in people taking sibutramine verses control (11.4% vs. 10.0%). The long-term health benefits of these treatments remain unclear.
Fenfluramine and dexfenfluramine were withdrawn from the market in 1997, while ephedrine (found in the traditional Chinese herbal medicine má huáng made from the Ephedra sinica) was removed from the market in 2004. Dexamphetamines are not approved by the FDA for the treatment of obesity due to concerns regarding addiction.[147] the use of these drugs is not recommended due to potential side effects. However, people do occasionally use these drugs illegally.
Surgery
Main article: Bariatric surgery
Bariatric surgery (“weight loss surgery”) is the use of surgical intervention in the treatment of obesity. As every operation may have complications, surgery is only recommended for severely obese people (BMI > 40) who have failed to lose weight following dietary modification and pharmacological treatment. Weight loss surgery relies on various principles: the two most common approaches are reducing the volume of the stomach (e.g. by adjustable gastric banding and vertical banded gastroplasty), which produces an earlier sense of satiation, and reducing the length of bowel that comes into contact with food (gastric bypass surgery), which directly reduces absorption. Band surgery is reversible, while bowel shortening operations are not. Some procedures can be performed laparoscopically. Complications from weight loss surgery are frequent.
Surgery for severe obesity is associated with long-term weight loss and decreased overall mortality. One study found a weight loss of between 14% and 25% (depending on the type of procedure performed) at 10 years, and a 29% reduction in all cause mortality when compared to standard weight loss measures. A marked decrease in the risk of diabetes mellitus, cardiovascular disease and cancer has also been found after bariatric surgery. Marked weight loss occurs during the first few months after surgery, and the loss is sustained in the long term. In one study there was an unexplained increase in deaths from accidents and suicide, but this did not outweigh the benefit in terms of disease prevention. When the two main techniques are compared, gastric bypass procedures are found to lead to 30% more weight loss than banding procedures one year after surgery.
The effects of liposuction on obesity are less well determined. Some small studies show benefits while others show none. A treatment involving the placement of an intragastric balloon via gastroscopy has shown promise. One type of balloon lead to a weight loss of 5.7 BMI units over 6 months or 14.7 kg (32.4 lb). Regaining lost weight is common after removal, however, and 4.2% of people were intolerant of the device.
Other Home Remedies
Honey: Mix one teaspoon of honey with two teaspoons of lime juice and some pepper. Drink this at least once a day.
Boiled Water: Drink a glass of boiled water every day after a meal.
Ginger Tea: Drink ginger tea 2-3 times a day.
Black Pepper: Seasoning foods with black pepper will decrease the need for salts and fats, and will still add flavor to foods. This will also help reduce weight.
Cinnamon: This spice can act as a low calorie sweetener to help reduce the amount of sugar needed in a recipe. It also adds a unique flavor to most cookie recipes.
Shudh Guggulu: Take Guggulu with a teaspoon of ginger and honey twice a day. This helps increase a body’s metabolism.
Trifla: This is another diet aid that contains amalaki, bibbitaki, and haritaki. This should be taken at least once a day if one chooses to use this supplement.
Raw or Cooked Cabbage: The intake of cabbage reduces the conversion of sugars to fat. Therefore, eating plenty of this well help increase the body’s ability to metabolize fatty foods.
Vitamin B-12: Take a vitamin B-12 tablet at least once daily. For further information on vitamin usage, read the directions on the vitamin bottle, and consult a doctor for more information. This vitamin comes also in leafy dark green vegetables, so eat many of these as often as possible.
Ayurvedic Medicines for Obesity
- Traphala Capsules
- Shuddha Guggulu Capsules
- Morslim-Z slimming Capsules of Obesity
When one follow the above diet recommendations and partake in one or more of the ayurvedic remedies, that person will be cured from obesity.
When not sure about how to apply herbal remedies or diet tablets, one should consult an ayurvedic specialist who is trained to help people in determining correct dosage. This is especially true for children inflicted with any disease, but is true for everyone. All medicines should be taken within the recommended guidelines.

Commiphora mukul ,Guggul

- as a binding agent only from modern perspective. Ayurveda mentions its use as anti-inflammatory, anti-obesity, uterine tonic, anti-hypercholesterolemic and immodulatory
- dose of the gum resin is from 5 to 50 grain used in placenta previa,amenorrhoea,dysmenorrhoea sore nipples,gonorrhea and ringworm
- how it is purified for gynecological disorders and what is the anupana
- purification of gum guggul (loban in unani medicine) – resin is soaked in water and left for some time . the supernatant water is decanted off. this process may be repeated once again. the vessel containing the dissolved resin is placed in the open and dried, that is the water is allowed to evaporate. drying may effected mechanically also.the resin to be employed will be in the form of an extract.
- Guggulu is considered to be a binding agent, though they have not used this term.
Acharya Sharangadhara mentions in Madhyama khanda 7/3….
Kuryad Avahnisiddena kwachid Gugguluna vatim!!
To prepare tablets without application of heat, Guggulu is added and tablets are advised to prepare. Here Guggulu acts as a binding agent only. - Lipid-lowering effects: Guggul (gum guggul) is a resin produced by the mukul mirth tree. Guggulipid is extracted from guggul using ethyl acetate. The preparation produced by extraction with petroleum ether is called a fraction A. Typical guggulipid preparations contain 2.5-5% of the plant sterols guggulsterones E and Z. These two components have been reported to exert effects on lipids.Several hypotheses have been advanced to explain these effects on lipids. Guggulsterones, particularly guggulsterone -pregnadiene-3,16-dione), have been reported to function as antagonists of the farsenoid X receptor (FXR) and the bile acid receptor (BAR), nuclear hormones which are involved with cholesterol metabolism and bile acid regulation. It has been reported that guggulsterone does not exert its lipid effects on mice lacking FXR. Other publications have proposed that guggul may inhibit lipogenic enzymes and HMG-Co A reductase in the liver. increase uptake of cholesterol by the liver via stimulation of LDL receptor binding. directly activate the thyroid gland and/or increase biliary and fecal excretion of cholesterol.
- Antioxidant effects: Guggul extracts have been reported to possess antioxidant properties possibly mediating protection against myocardial necrosis
- Platelet effects: Guggulipid has been found to inhibit platelet aggregation and increase fibrinolysis
- Anti-inflammatory: the results of several studies suggest possible anti-inflammatory and antiarthritic activities of guggul. On a per-microgram basis, guggulipid appears to be significantly less potent than indomethacin or hydrocortisone. Possible effects on high-sensitivity C-reactive protein (hs-CRP) have recently been observed in a clinical trial.
- Guggul has been a key component in ancient Indian Ayurvedic system of medicine. But has become so scarce because of its overuse in its two habitats in India where it is found — Gujarat and Rajasthan that the World Conservation Union (IUCN) has enlisted it in its Red Data List of endangered species.Guggul produces a resinous sap known as gum guggul. The extract of this gum, called gugulipid, guggulipid or guglipid, has been used in Ayurvedic medicine, a traditional Hindu medicine, for nearly 3,000 years in India. The active ingredient in the extract is the steroid guggulsterone, which acts as an antagonist of the farnesoid X receptor, once believed to result in decreased cholesterol synthesis in the liver. However, several studies have been published that indicate no overall reduction in total cholesterol occurs using various dosages of guggulsterone, and levels of low-density lipoprotein (“bad cholesterol”) increased in many people.
- Guggul is sought for its gummy resin, which is harvested from the plant’s bark through the process of tapping. In India and Pakistan, guggul is cultivated commercially. The resin of the guggul plant, known as gum guggulu, has a fragrance similar to that of myrrh and is commonly used in incense and perfumes. It is the same product that was known in Hebrew, ancient Greek and Latin sources as bdellium.Guggul can be purchased in a loosely packed form called dhoop, an incense from India, which is burned over hot coals. This produces a fragrant, dense smoke. The burning coals which let out the smoke are then carried around to different rooms and held in all corners for a few seconds. This is said to drive away evil spirits as well as remove the evil eye from the home and its family members.

{kind=link}