
FLAGS AND HITS
 DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO FACEBOOK
...................................................................Join me on twitter
FACEBOOK
...................................................................Join me on twitter
 ..................................................................Join me on google plus
..................................................................Join me on google plus
 Googleplus
GoogleplusMYSELF

Velagliflozin
Velagliflozin
VETERINARY DRUG
- Cas 946525-65-1
- FV2YU8SL0P
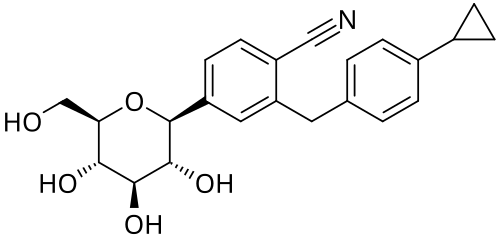
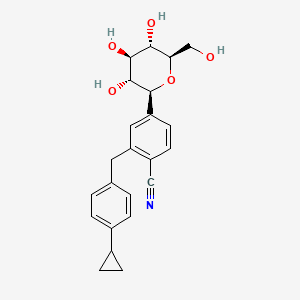
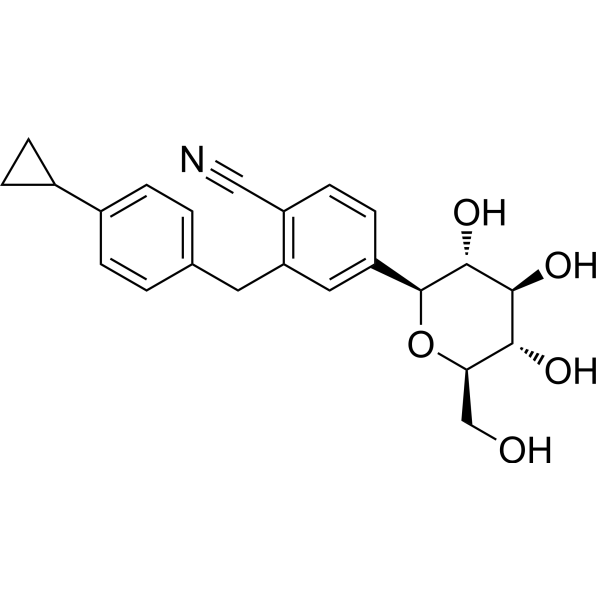
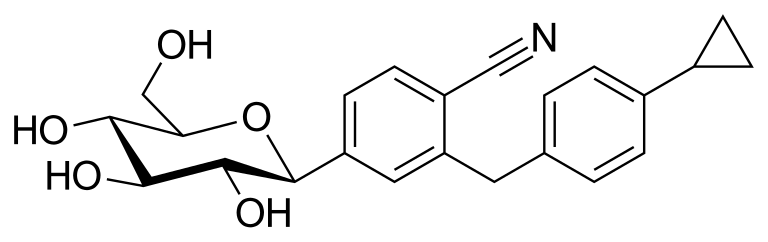
- 2-((4-cyclopropylphenyl)methyl)-4-((2S,3R,4R,5S,6R)-3,4,5-trihydroxy-6-(hydroxymethyl)oxan-2-yl)benzonitrile
- 2-((4-Cyclopropylphenyl)methyl)-4-beta-D-glucopyranosylbenzonitrile
- 395.4 g/mol, C23H25NO5
2-[(4-cyclopropylphenyl)methyl]-4-[(2S,3R,4R,5S,6R)-3,4,5-trihydroxy-6-(hydroxymethyl)oxan-2-yl]benzonitrile
- 2-((4-CYCLOPROPYLPHENYL)METHYL)-4-.BETA.-D-GLUCOPYRANOSYLBENZONITRILE
- BENZONITRILE, 2-((4-CYCLOPROPYLPHENYL)METHYL)-4-.BETA.-D-GLUCOPYRANOSYL-
Velagliflozin L-proline H2O
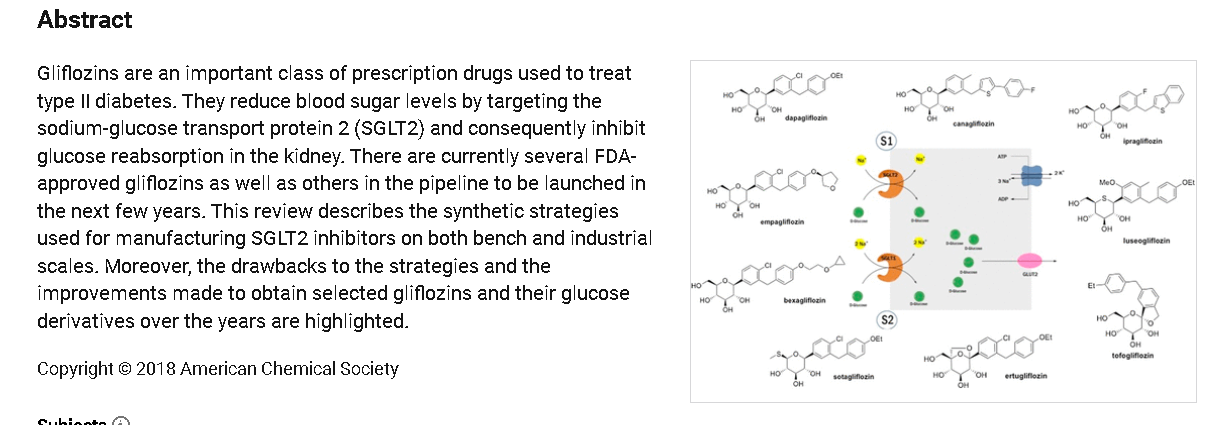
Velagliflozin, sold under the brand name Senvelgo, is an antidiabetic medication used for the treatment of cats.[2][4][5] Velagliflozin is a sodium-glucose cotransporter 2 (SGLT2) inhibitor.[6] It is taken by mouth.[2]
Velagliflozin is the active ingredient of the first oral liquid medication approved by the Food and Drug Administration for the treatment of diabetes in cats. This compound belongs to the known class of sodium-glucose cotransporter 2 inhibitors approved to treat diabetes in human.
- Application: NADA 141-568Drug: Senvelgo®Active Ingredient(s): VelagliflozinCompany: Boehringer lngelheim Animal Health USA Inc.Patent(s): 7776830 (Exp: 05/01/2027); 8557782 (Exp: 05/01/2027); 9145434 (Exp: 09/07/2033); 10617666 (Exp: 06/06/2035); 11896574 (Exp: 12/17/2034); 10220017 (Exp: 09/29/2036); 10709683 (Exp: 08/24/2036); 11225500 (Exp: 12/17/2038)
- [Indication for Use] To improve glycemic control in otherwise healthy cats with diabetes mellitus not previously treated with insulin.Application: NADA 141-568Active Ingredient(s): VelagliflozinCompany: Boehringer lngelheim Animal Health USA Inc.Freedom of Information: FOIA Summary 14320Approval Date: August 10, 2023
APPROVALS 2023, GDA 2023, EU 2023, EMA 2023, SENVELGO
Velagliflozin (brand name Senvelgo) is a veterinary medication approved for treating diabetes in cats, not humans.
Approved countries and years for velagliflozin:
- United States (US): Approved by the FDA in August 2023.
- European Union (EU): Received marketing authorization in November 2023.
- Switzerland: Approved in 2023.
- Great Britain: Approved in 2023.
SYN
https://patentscope.wipo.int/search/en/detail.jsf?docId=US310904480&_cid=P11-METCZG-99171-1
SYN
US7776830
https://patentscope.wipo.int/search/en/detail.jsf?docId=US41880220&_cid=P11-METD0X-00376-1
| The following compound is obtained analogously to Example XXIV: |
(1) 1-Cyano-2-(4-cyclopropyl-benzyl)-4-(β-D-glucopyranos-1-yl)-benzene
EXAMPLE 17
2-(4-Cyclopropyl-benzyl)-4-(β-D-glucopyranos-1-yl)-benzonitrile
| The compound is obtained according to example 6 using 4-cyclopropyl-phenylboronic acid as the coupling partner. |
SYN
WO2007128749
https://patents.google.com/patent/WO2007128749A1/en
The following compound is obtained analogously to Example XXIV:
(1 ) 1 -Cvano-2-(4-cvclopropyl-benzyl)-4-(3-D-glucopyranos-1 -vD-benzene

Mass spectrum (ESI“): m/z = 413 [M+H] + Advantageously, the reduction of the anomeric carbon center of the appropriate intermediate obtained during the synthesis of this compound is conducted with the oxygen functionalities on the pyranose ring protected. Preferred protective groups are benzyl, p-methoxybenzyl, trimethylsilyl, triethylsilyl, terfbutyldimethylsilyl, triisopropylsilyl and allyl.
Example XXV

1-Cyano-2-(4-cyclopropyl-benzyl)-4-(tetra-O-acetyl-β-D-glucopyranos-1-yl)-benzene To a flask charged with a stir bar, 4-(2,3,4,6-tetra-O-acetyl-D-glucopyranos-1-yl)-2-(4- trifluoromethylsulfonyloxy-benzyl)-benzonitrile (4.4 g), degassed toluene (12 ml.) and degassed water (8 ml.) and kept under argon atmosphere is added cyclopropylboronic acid (0.20 g), potassium phosphate (5.0 g), tricyclohexylphosphine (0.19 g) and at last palladium(ll)acetate (76 mg). The mixture is stirred at 1 10 °C for 6 h meanwhile cyclopropylboronic acid is added after each hour (5x 0.20 g). After cooling to room temperature, the mixture is diluted with aqueous sodium hydrogen carbonate solution and extracted with ethyl acetate. The combined extracts are dried (sodium sulphate) and the solvent is removed under reduced pressure. The residue is chromatographed on silica gel (cyclohexane/ethyl acetate 20:1 -> 1 :1 ). Yield: 3.2 g (87% of theory ) Mass spectrum (ESI+): m/z = 581 [M+NH4] +
Example XXVI

4-(1 -Hvdroxy-cvclopropyD-phenylboronic acid A 3.0 M solution of ethylmagnesium bromide in diethylether (7.6 ml.) is added to a stirred solution of titanium(IV) isopropoxide (2.2 ml.) in diethylether (70 ml.) chilled to -78 °C. The resultant solution is stirred at -78 °C for 1.5 h, before 4-(4,4,5,5-tetramethyl-[1 ,3,2]dioxa borolan-2-yl)-benzoic acid methyl ester (2.0 g) is added. The reaction mixture is warmed to ambient temperature and stirred for an additional 12 h. Then, 1 M aqueous hydrochloric acid is added and the resulting mixture is extracted with ethyl acetate. The combined organic extracts are dried (sodium sulphate) and the solvent is evaporated. The residue is dissolved in acetone (60 ml.) and 0.1 M aqueous NH4OAc solution (50 ml.) followed by NaIO4 (2.3 g) is added. The resulting reaction mixture is stirred at room temperature for 18 h. After removal of the acetone, the residue is extracted with ethyl acetate. The combined extracts are dried (sodium sulphate) and the solvent is evaporated. The residue is purified by chromatography on silicagel (cyclohexane/ethyl acetate). Yield: 0.45 g (33% of theory) Mass spectrum (ESI“): m/z = 223 [M+HCOO]“ Preparation of the end compounds:
Example 17: 2-(4-Cyclopropyl-benzyl)-4-(β-D-glucopyranos-1-yl)-benzonitrile

Mass spectrum (ESI+): m/z = 413 [M+NH4]+
The compound is obtained according to example 6 using 4-cyclopropyl-phenylboronic acid as the coupling partner.
Yield: 83% of theory
Alternatively this compound is obtained as described in Example XXIV(I ).
The compound of example 17 is also obtained by employing the following procedure:
A solution of 2-(4-cyclopropyl-benzyl)-4-(2,3,4,6-tetra-O-acetyl-D-glucopyranos-1 -yl)- benzonitrile (0.80 g) in methanol (5 ml.) and THF (5 ml.) is treated with aqueous potassium hydroxide solution (4 mol/l, 5 ml_). The reaction solution is stirred at ambient temperature for 1 h and then neutralized with 1 M hydrochloric acid. The organic solvents are evaporated and the residue is diluted with brine and extracted with ethyl acetate. The organic extracts are dried (sodium sulphate) and the solvent is removed. The residue is chromatographed on silica gel (dichloromethane/methanol 1 :0 -> 9:1 ). Yield: 0.54 g (96% of theory)
SYN
Synthesis 2024, 56, 906–943
In 2007, Boehringer-Ingelheim Vetmedica GmbH pioneered the development of velagliflozin (15), subsequently submitting a patent application in the United States with the identification number US7776830B2.72a More recently, through clinical investigations, this compound has demonstrated its efficacy as an SGLT2 inhibitor, proving adept at curtailing glucose reabsorption, encouraging glucosuria,
and leading to reductions in both blood glucose and insulin levels.
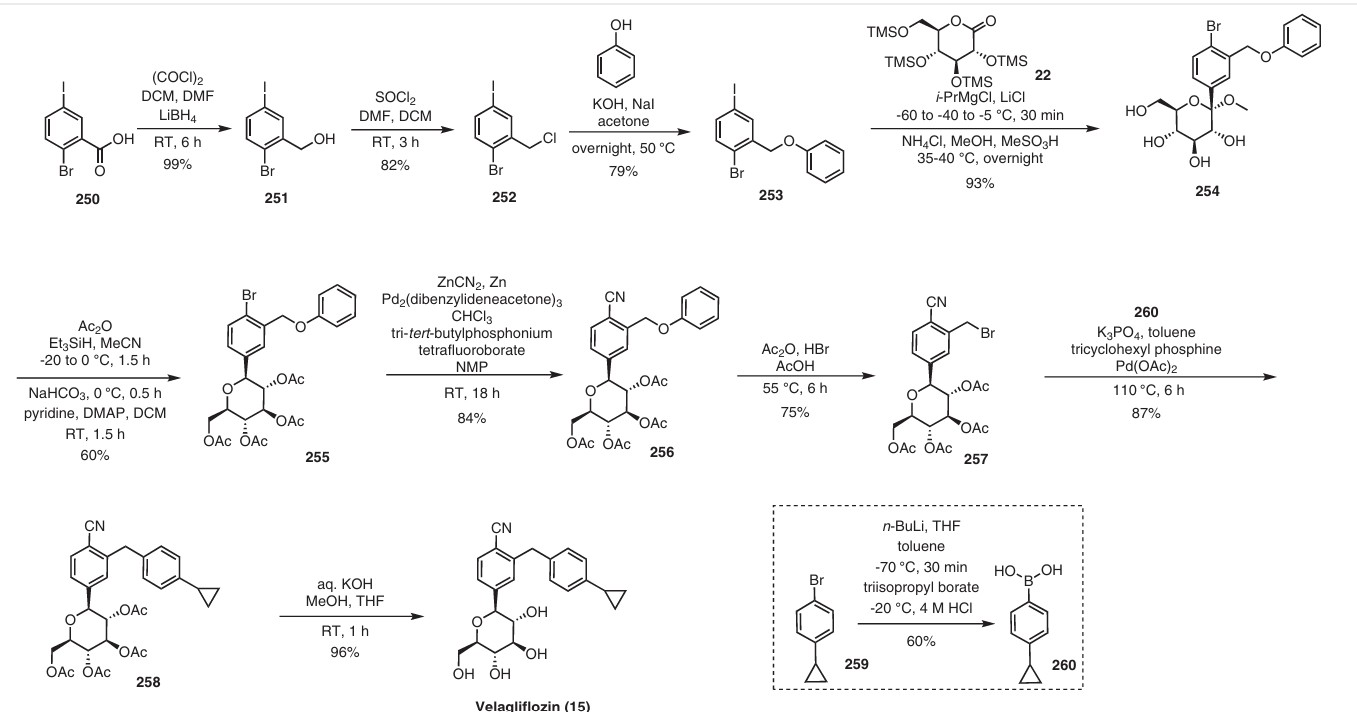
The initial synthesis of velagliflozin (15) was also disclosed in the above patent,72a and in patent
WO2007128749A1.72b The synthesis, depicted in Scheme46, comprises of nine-steps starting with the readily available raw material 2-bromo-5-iodobenzoic acid (250), which undergoes reduction using LiBH4 to form the corresponding alcohol 251. Subsequently, chlorination is carried out using thionyl chloride, resulting in the formation of chloride 252. O-Alkylation of phenol with compound 252 is
then conducted in a basic medium, yielding intermediate 253.The C-glycosylation of 253 with 2,3,4,6-tetrakis-O(trimethylsilyl)-D-glucopyranone 22 in the presence of turbo Grignard reagent (isopropylmagnesium chloride and LiCl) and methanesulfonic acid in methanol gives compound
254 with an impressive 93% yield. The hydroxy group of in termediate 254 is protected using acetic anhydride, and themethoxy group is subsequently removed via Lewis acid (BF3·Et2O, Et3SiH) treatment, providing compound 255 in a yield of 60%. A metal-catalyzed cyano group installation is then performed on intermediate 255, leading to the formation of compound 256 in 84% yield. The subsequent steps involve benzylic bromination followed by coupling with cyclopropylphenyl boronic acid 260, resulting in the formation of intermediate 258. Finally, deacetylation of intermediate 258 using aqueous KOH produces the desired product
The overall yield obtained for velagliflozin (15) is calculated to be 11.3%, with this synthetic route providing a systematic and efficient approach. The highlight of the route is high-yielding chemical transformations. However, the drawback is the use of two palladium-mediated couplings
that increase the possibility of leaching of the toxic metal in scale-up batches. Additionally, the synthetic route requires a large number of chemical transformations and not best suited for commercial production.
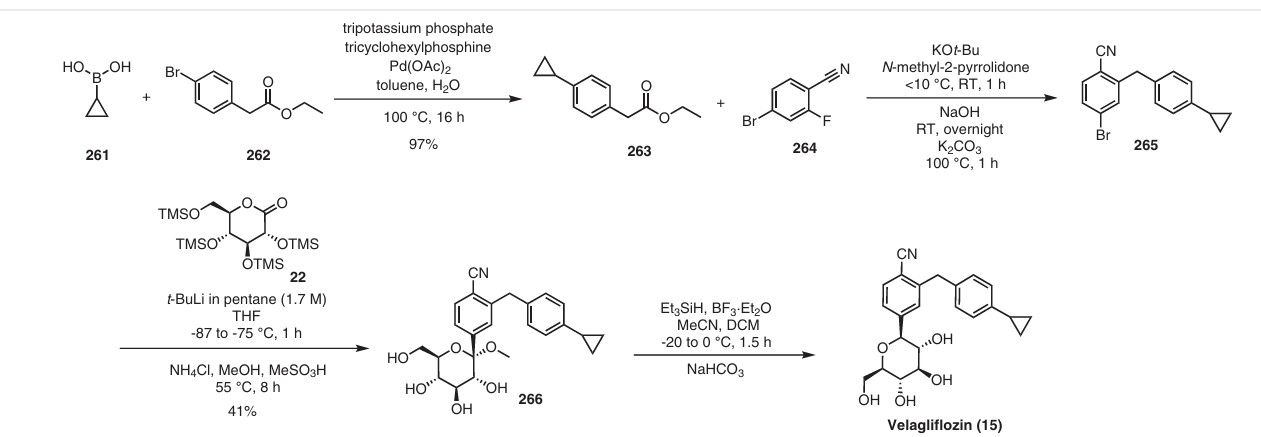
The same authors reported an alternative method (Scheme 47) for the synthesis of velagliflozin (15) in the product patent.72 The aglycone intermediate 265 is accessed in two steps starting from ethyl 2-(4-bromophenyl)acetate (262). O-Glycosylation takes place with the aglycone
4-bromo-2-(4-cyclopropylbenzyl)benzonitrile (265) using 2,3,4,6-tetrakis-O-(trimethylsilyl)-D-glucopyranone 22 in the presence of tert-butyllithium in pentane (1.7 M), resulting in the formation of compound 266. Reduction of compound 266 using boron trifluoride–diethyl etherate yields
the final API velagliflozin (15). This truncated synthetic route is well suited for scale-up due to the significantly low er number of transformations compared to the previous route. Unfortunately, the specific yields were not clearly in dicated for this process. This method presents an alternative approach to the synthesis of velagliflozin (15), providing a potential pathway for its preparation in 5 steps with
an overall yield of 40%.
(72) (a) Eckhardt, M.; Himmelsbach, F.; Eickelmann, P.; Sauer, A.;
Thomas, L. US7776830B2, 2010. (b) Eckhardt, M.; Himmelsbach,
F.; Eickelmann, P.; Sauer, A.; Thomas, L. WO2007128749A1,
2007.



AS ON JUNE2025 4.45 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT

join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE

join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com

……
Medical uses
Velagliflozin is indicated to improve glycemic control in otherwise healthy cats with diabetes not previously treated with insulin.[2][4][6]
References
- “Notice: Multiple additions to the Prescription Drug List (PDL) [2024-10-18]”. Health Canada. 18 October 2024. Retrieved 25 October 2024.
- “Senvelgo- velagliflozin solution”. DailyMed. 8 November 2023. Retrieved 13 December 2023.
- “Senvelgo Product information”. Union Register of veterinary medicinal products. 22 November 2023. Retrieved 29 August 2024.
- “NADA 141-568 Senvelgo (velagliflozin oral solution) Cats”.
 This article incorporates text from this source, which is in the public domain.
This article incorporates text from this source, which is in the public domain. - Cook AK, Behrend E (January 2025). “SGLT2 inhibitor use in the management of feline diabetes mellitus”. Journal of Veterinary Pharmacology and Therapeutics. 48 Suppl 1 (Suppl 1): 19–30. doi:10.1111/jvp.13466. PMC 11736986. PMID 38954371.
- “Dear Veterinarian Letter regarding important safety conditions associated with the use of Senvelgo (velagliflozin oral solution) for improving glycemic control in certain cats with diabetes mellitus”. U.S. Food and Drug Administration. 4 December 2023. Retrieved 13 December 2023. This article incorporates text from this source, which is in the public domain.
| Clinical data | |
|---|---|
| Trade names | Senvelgo |
| License data | US DailyMed: Velagliflozin |
| Routes of administration | By mouth |
| ATCvet code | QA10BK90 (WHO) |
| Legal status | |
| Legal status | CA: ℞-only[1]US: ℞-only[2]EU: Rx-only[3] |
| Identifiers | |
| IUPAC name | |
| CAS Number | 946525-65-1 |
| PubChem CID | 24862817 |
| ChemSpider | 58827717 |
| UNII | FV2YU8SL0PEQE2P2T77I |
| Chemical and physical data | |
| Formula | C23H25NO5 |
| Molar mass | 395.455 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| SMILES | |
| InChI | |
- SGLT2 inhibitors: a novel therapy for cognitive impairment via multifaceted effects on the nervous systemPublication Name: Translational NeurodegenerationPublication Date: 2024-08-09PMCID: PMC11312905PMID: 39123214DOI: 10.1186/s40035-024-00431-y
- Demographic, morphologic, hormonal and metabolic factors associated with the rate of improvement from equine hyperinsulinaemia-associated laminitisPublication Name: BMC Veterinary ResearchPublication Date: 2022-01-18PMCID: PMC8764787PMID: 35042535DOI: 10.1186/s12917-022-03149-z
- The efficacy and safety of velagliflozin over 16 weeks as a treatment for insulin dysregulation in poniesPublication Name: BMC Veterinary ResearchPublication Date: 2019-02-26PMCID: PMC6390376PMID: 30808423DOI: 10.1186/s12917-019-1811-2
- The sodium-glucose co-transporter 2 inhibitor velagliflozin reduces hyperinsulinemia and prevents laminitis in insulin-dysregulated poniesPublication Name: PLOS ONEPublication Date: 2018-09-13PMCID: PMC6136744PMID: 30212530DOI: 10.1371/journal.pone.0203655
- Effects of the sodium‐glucose cotransporter 2 (<scp>SGLT</scp>2) inhibitor velagliflozin, a new drug with therapeutic potential to treat diabetes in catsPublication Name: Journal of Veterinary Pharmacology and TherapeuticsPublication Date: 2017-11-15PMID: 29139146DOI: 10.1111/jvp.12467
/////////Velagliflozin, APPROVALS 2023, GDA 2023, EU 2023, EMA 2023, SENVELGO, DIABETES, SENVELGO,
Cetagliptin
Cetagliptin
CAS No. FREE FORM : 2243737-33-7 C18H18F6N4O, 420.4 g/mol
[ Cetagliptin Phosphate 2243737-33-7 ]
| 분자량 MW | 518.35 |
|---|---|
| 화학식 MF | C18H21F6N4O5P |
(3R)-3-amino-1-[(8R)-8-methyl-3-(trifluoromethyl)-6,8-dihydro-5H-imidazo[1,5-a]pyrazin-7-yl]-4-(2,4,5-trifluorophenyl)butan-1-one
(3R)-3-amino-1-[(8R)-8-methyl-3-(trifluoromethyl)-6,8-dihydro-5H-imidazo[1,5-a]pyrazin-7-yl]-4-(2,4,5-trifluorophenyl)butan-1-one
CHINA 2024, APPROVALS 2024, CGeneTec, DIABETES,
- GTPL13952
- CGT8012
- OriginatorCGeneTech
- Class2 ring heterocyclic compounds; Amines; Antihyperglycaemics; Fluorobenzenes; Imidazoles; Ketones; Pyrazines; Small molecules
- Mechanism of ActionDipeptidyl peptidase 4 inhibitors
RegisteredType 2 diabetes mellitus CHINA 2024
- 01 Dec 2024Registered for Type 2 diabetes mellitus in China (PO) – First global approval
- 20 Mar 2024Chemical structure information added
- 28 Jun 2023No recent reports of development identified for phase-I development in Type-2-diabetes-mellitus(In volunteers) in China (PO, Tablet)
- Cetagliptin is an orally active inhibitor for dipeptidyl peptidase 4 (DPP-4) and CYP2D6 (IC50 of 6 µM). Cetagliptin is a substrate for P-glycoprotein. Cetagliptin reduces the GLP-1 degradation, maintains the level of postprandial blood sugar, and can be used in type 2 diabetes mellitus research.
Cetagliptin (CGT-8012) is an orally bioavailable, dipeptidyl peptidase 4 enzyme (DPP-4) inhibitor (‘gliptin’) class drug. It was designed as an antihyperglycemic agent to treat type 2 diabetes mellitus (T2DM) via inhibition of DPP-4-mediated catbolism of incretin hormones including glucagon-like peptide-1 (GLP-1) [2].
- A DPP-4 inhibitor pharmaceutical composition and its preparation method and usePublication Number: CN-118557538-APriority Date: 2024-08-01
- A kind of preparation method of DPP-IV inhibitor and its key intermediatePublication Number: CN-114057751-APriority Date: 2022-01-17
- A kind of preparation method of DPP-IV inhibitor and its key intermediatePublication Number: CN-114057751-BPriority Date: 2022-01-17Grant Date: 2022-04-12
- A kind of preparation method of DPP-IV inhibitor and key intermediate thereofPublication Number: TW-202330535-APriority Date: 2022-01-17
- A preparation method of a DPP-IV inhibitor and its key intermediatePublication Number: TW-I842342-BPriority Date: 2022-01-17Grant Date: 2024-05-11
- Salt of cetagliptin, preparation method thereof, pharmaceutical composition, and use thereofPublication Number: US-2020123164-A1Priority Date: 2018-04-26
- Salt of cetagliptin, preparation method therefor, pharmaceutical composition, and use thereofPublication Number: EP-3785713-A1Priority Date: 2018-04-26
- Salt of cetagliptin, preparation method thereof, pharmaceutical composition, and use thereofPublication Number: US-11046701-B2Priority Date: 2018-04-26Grant Date: 2021-06-29
- Tetrahydro-imidaz0[1,5-a]pyrazine derivatives, preparation process and medicinal use thereofPublication Number: US-2010273786-A1Priority Date: 2007-12-26
- Tetrahydro-imidazo[1,5-α]pyrazine derivatives, preparation process and medicinal use thereofPublication Number: US-8207161-B2Priority Date: 2007-12-26Grant Date: 2012-06-26
SYN
https://patentscope.wipo.int/search/en/detail.jsf?docId=CN84092509&_cid=P20-MERZ31-36806-1
SYN
CN103351391
https://patents.google.com/patent/CN103351391A/en
Synthetic route and the concrete steps of compound (I) are as follows:
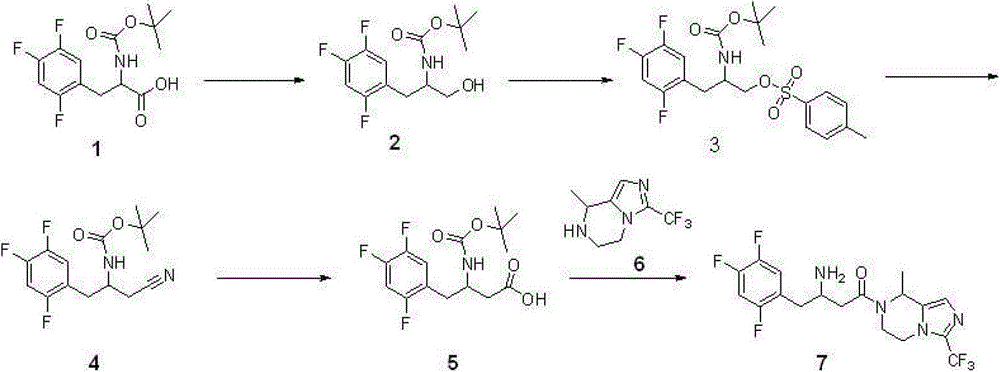
Step 1: synthetic compound 2
With 11.8 gram (0.037 mole) compound 1{DL N-[(1,1-dimethyl oxyethyl group) carbonyl]-2,4; 5-trifluorophenyl-L-Ala, DL N-[(1,1-dimethylethoxy) carbonyl]-2; 4; 5-trifluorophen yl-alanine, CAS:1367740-01-9, reference: synthetic chemistry; 2011; 19 (4), 557-560} is dissolved among 40 milliliters of THF, adds 5.8 milliliters of triethylamines (0.042 mole) again; reaction is cooled to 0 ℃; add 4.0 milliliters of Vinyl chloroformates (0.041 mole), 0 ℃ was reacted 1 hour under nitrogen protection, after the filtration filtered liquid was cooled to 0 ℃; slowly add sodium borohydride (1.4 grams; 0.057 the mole) mixed solution in 15 ml waters, stirring is spent the night, and adds 1N HCl acidifying; ethyl acetate extraction three times; merge organic phase, sodium hydrogen carbonate solution is washed, the saturated salt washing; anhydrous sodium sulfate drying; the concentrated 7.6 gram products that obtain, namely compound 2, yield 67%.Repeat this step, make more compound 2, use for subsequent step.
Step 2: synthetic compound 3
8.2 gram (0.027 mole) compounds 2 are dissolved in 40 milliliters of methylene dichloride; add again 4.2 milliliters of triethylamines (0.030 mole); the catalytic amount DMAP; reaction is cooled to 0 ℃; add Tosyl chloride (6.8 grams; 0.035 mole); 0 ℃ is arrived room temperature reaction 2 hours under nitrogen protection, adds 1N HCl acidifying, dichloromethane extraction three times; merge organic phase; sodium hydrogen carbonate solution is washed, saturated salt washing, anhydrous sodium sulfate drying; concentrate and obtain crude product, namely compound 3.Repeat this step, make more compound 3, use for subsequent step.
Step 3: synthetic compound 4
12.4 gram (0.027 mole) compounds 3 are dissolved in 40 milliliters of dimethyl formamides, slowly add the mixed solution of sodium cyanide (4.5 grams, 0.092 mole) in 30 milliliters of dimethyl formamides, room temperature reaction 48 hours, pour in 100 milliliters of frozen water, ethyl acetate extraction three times merges organic phase, the saturated salt washing, anhydrous sodium sulfate drying, concentrated rear column chromatography purification obtains 7.8 gram products, be compound 4, yield 92%.
Step 4: synthetic compound
5
3.1 gram (0.010 mole) compounds 4 are dissolved in 15 milliliters of 6N hydrochloric acid, and reflux is spent the night, and adds the neutralization of 2N sodium hydroxide solution, cooling drying.The gained solid is dissolved among 30 milliliters of THF, adds 20 milliliters of 0.5N sodium hydroxide solutions, adds tert-Butyl dicarbonate (2.4 grams again, 0.011 mole), room temperature reaction
16 hours, concentrated, add the neutralization of 10% sodium bisulfate, ethyl acetate extraction three times merges organic phase, the saturated salt washing, anhydrous sodium sulfate drying, the concentrated 3.3 gram products that obtain, namely, compound
5, yield 99%.
Step 5: synthetic compound 7
Compound 6{5; 6; 7; 8-tetrahydrochysene-8-methyl-3-(trifluoromethyl)-imidazo [1,5-a] pyrazine, 5; 6; 7,8-tetrahydro-8-methyl-3-(trifluoromethyl)-imidazo[1,5-a] pyrazine; synthesize and see CN103087067; 2.1 gram, 0.010 mole } be dissolved in 8 milliliters of methylene dichloride, add triethylamine 1.2 grams (0.012 mole); compound 5 (3.3 grams; 0.010 mole), EDCI2.3 restrains (0.012 mole), room temperature reaction is 24 hours under nitrogen protection; pour in 100 milliliters of frozen water; organic phase is washed saturated salt washing, anhydrous sodium sulfate drying; the concentrated crude product that obtains; be dissolved in 100 milliliters of the 2N HCl/ methanol solutions (anhydrous HCl gas is dissolved in the solution of methyl alcohol), room temperature reaction 4 hours is spin-dried for; cooling; pour in 100 milliliters of frozen water, transfer PH to 9, ethyl acetate extraction three times; merge organic phase; and wash saturated salt washing, anhydrous sodium sulfate drying; concentrated; column chromatography purification obtains 2.8 gram products, and namely compound 7, yield 66%.
Compound 7 comprises four optical isomers, and route and the concrete steps of their separation and purification are as follows:
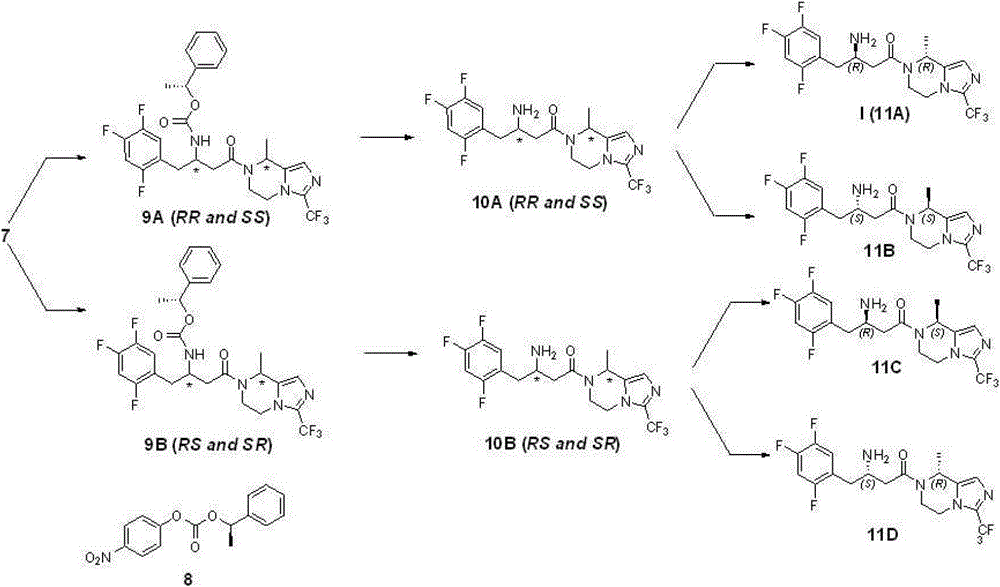
Step 6: preparation compound 9A and 9B
2.8 gram (6.67 mmole) compounds 7 are dissolved in 50 milliliters of acetonitriles; add triethylamine 1.2 grams (8.0 mmole); add again compound 8 (1.9 grams; 6.67 mmole; reference: J.Org.Chem.1995; 60 (3); 730), reflux is spent the night under nitrogen protection, and is concentrated; add ethyl acetate; the 1N sodium hydroxide solution is washed, and ethyl acetate milliliter extraction three times merges organic phase; the saturated salt washing; anhydrous sodium sulfate drying, the evaporating column chromatography purification obtains 1.6 gram 9A (43%) and 1.4 gram 9B (39%) products (de>98%); structural analysis determines that tentatively 9A is RR and SS mixture of enantiomers, and 9B is RS and SR mixture of enantiomers.Gained compound 9A and 9B give over to respectively next step and use.
Step 7: preparation compound 10A and 10B
1.5 gram (2.64 mmole) compound 9A are dissolved in 50 milliliters of methylene dichloride, reaction is cooled to 0 ℃, adds HBr solution (2M, 2.6 milliliters, 5.2 mmole), be dissolved in ethyl acetate after concentrated, sodium hydrogen carbonate solution is washed, the saturated salt washing, anhydrous sodium sulfate drying, the concentrated product that obtains, namely compound 10A (RR and SS mixture of enantiomers) gives over to next step and uses.
According to same reaction principle, condition and step, take compound 9B as starting raw material, obtain compound 10B (RS and SR mixture of enantiomers), give over to next step and use.
Step 8: preparation compound 11A, 11B and 11C, 11D
Resulting compound 10A in the step 7 (1.1 gram) is dissolved in 20 milliliters of ethanol, adds D-tartrate 0.4 gram (2.64 moles), reflux 0.5 hour, cooling, filter, obtain white solid, again with behind ten times of amount ethyl alcohol recrystallizations 2 times, obtain white solid, free with saturated sodium bicarbonate aqueous solution, obtain 0.29 and digest compound 11A, be i.e. compound (I), yield 26% is surveyed ee value>95%.
PAPER
https://www.tandfonline.com/doi/full/10.1080/00498254.2022.2091494
SYN
https://patents.google.com/patent/US11046701B2/en
SYN
European Journal of Medicinal Chemistry 291 (2025) 117643
Cetagliptin phosphate, developed by CGeneTec, is a DPP-4 inhibitor designed for the treatment of T2DM. In 2024, the NMPA approved cetagliptin phosphate for managing T2DM. As a member of the DPP-4inhibitor, Cetagliptin exerts its effect on glycemic regulation by impeding the breakdown of incretin hormones. This action leads to a glucose-dependent increase in insulin secretion and a concurrent decrease in glucagon levels. Multiple clinical investigations have attested to the effectiveness and safety profile of sitagliptin. In a particular instance, a randomized, double-blind, placebo-controlled Phase 3 study was carried out to assess the use of sitagliptin as a single-agent treatment in patients diagnosed with type 2 diabetes [67]. The study found that cetagliptin significantly reduced HbA1c levels compared to placebo, with a greater proportion of patients achieving target glycemic control.
The treatment was generally well tolerated, with a safety profile comparable to placebo [68,69]. Regarding toxicity, cetagliptin was well tolerated in clinical studies, with no significant increase in adverse effects compared to placebo. No drug-related hypoglycemia was reported,
indicating a favorable safety profile [70].
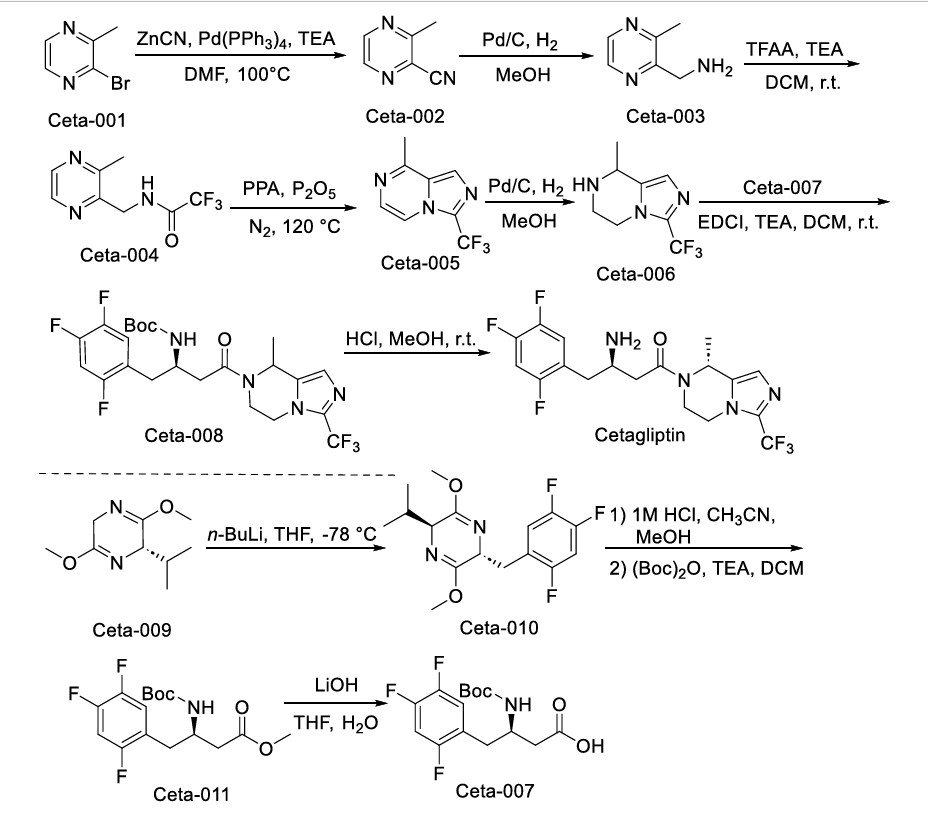
The synthesis of Cetagliptin, depicted in Scheme 16, initiates with Ceta-001 cyanidation affording Ceta-002, whose hydrogenative reduction yields Ceta-003 [71]. Subsequent amidation constructs Ceta-004,
followed by cyclization rearrangement producing Ceta-005. Hydrogenation delivers Ceta-006, which undergoes coupling with Ceta-007 assembling Ceta-008. Final TFA-mediated deprotection achieves
Cetagliptin. Concurrently, the side route involves Ceta-009 nucleophilic substitution forming Ceta-010. Sequential imine hydrolysis/protection converts Ceta-010 to Ceta-011, whose controlled hydrolysis ultimately delivers Ceta-007
67-70
[67] J. Lu, J. Zhao, D. Xie, J. Ding, Q. Yu, T. Wang, Use of a PK/PD model to select
Cetagliptin dosages for patients with type 2 diabetes in phase 3 trials, Clin.
Pharmacokinet. 63 (2024) 1463–1476.
[68] L. Guo, F. Tian, L. Liu, M. Chen, C. Jiang, S. Li, C. Liu, Y. Zhang, J. Qin, D. Yu,
Y. Zong, W. Dai, Retagliptin as add-on therapy to metformin in Chinese patients
with type 2 diabetes inadequately controlled with metformin: a multicentre,
randomized, double-blind, placebo-controlled, phase 3 trial, Diabetes Obes Metab
26 (2024) 2830–2838.
[69] C. Hu, J. Zheng, J. Miao, F. Liu, T.T. Hu, J.K. Gu, S.Q. Shu, Y. Wang, X.H. Zhu, M.
Z. Liang, [Pharmacokinetics of Phosphate Retagliptin Tabletin in Patients with
Renal Dysfunction], Sichuan Da Xue Xue Bao Yi Xue Ban 49 (2018) 74–80.
[70] A. Cahn, S. Cernea, I. Raz, An update on DPP-4 inhibitors in the management of
type 2 diabetes, Expert Opin Emerg Drugs 21 (2016) 409–419.
AS ON JUNE2025 4.45 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
……
https://en.cgenetech.com.cn/news/55.html
Since the listing application of a class of innovative drug Cetagliptin independently developed by CGeneTech was accepted by the State Food and Drug Administration, it has received great attention in the industry. Recently, the well-known industry media “Shell News Agency” also took this opportunity to comprehensively sort out the hot track and broad market prospects of domestic DPP-4 inhibitors. This article is shared with you. In the face of the high expectations given by the industry, CGeneTech will continue to run the last “one kilometer” of product launch with a scientific and rigorous attitude.
Diabetes (DM), as a chronic disease, has attracted much attention. Diabetes drugs have become the second largest drug market after tumor drugs, and it is also a place for pharmaceutical enterprises to compete.
With the development of medicine, some new drugs with different mechanism of action from traditional oral hypoglycemic drugs have emerged in recent years. Dipeptidyl peptidase-4 (DPP-4) inhibitor is one of them. At present, there are dozens of DPP-4 inhibitors, which are collectively known as “gliptin drugs”. In the future, the market size of gliptin drugs in China will exceed 30 billion yuan.
Cetagliptin seven-year long run
On February 2, CGeneTech submitted to the National Drug Administration (NMPA) the marketing application (NDA) of Cetagliptin, a DPP-4 inhibitor, which was mainly used to treat type 2 diabetes. This means that the domestic DPP-4 inhibitor market will usher in new members, and the official website of CGeneTech will also publicize the progress of Cetagliptin research and development in the product pipeline for the first time, and the listing has been confirmed.
Cetagliptin is a Class 1 innovative drug independently developed by CGeneTech, and once was its own fist product in its pipeline. It has also experienced a seven-year long run since its launch of research and development, and is about to hit the line successfully.
In 2006, the targeted hypoglycemic drug Sigliptin was approved by the FDA of the United States, which is undoubtedly a major event in the industry. Ten years later, CGeneTech completed the pre-clinical study of head-to-head comparison of Cetagliptin and Xigliptin.
At the beginning of 2018, CGeneTech launched the phase I clinical trial of head-to-head comparison of Cetagliptin and Xigliptin. Among nearly 200 patients in the Phase I clinical trial completed by Cetagliptin, the data showed that when the intake of Cetagliptin reached 50 mg, it was able to achieve the DPP-4 inhibition capacity equivalent to the intake of 100 mg of Xigliptin. Cetagliptin is administered once a day. It can reach the peak within 1 to 2 hours after administration, and has a longer half-life than Sigliptin, which can maintain stable glucose reduction for a longer time.
Diabetes requires long-term medication, and safety is the first factor to be considered when doctors choose drugs when prescribing. In the safety study, the adverse effects of the intake of Cetagliptin on the body of patients were almost undetectable, lower than that of the blank group and Sigliptin group. In addition, although Cetagliptin has a long half-life, there is no accumulation of residual drugs in the body in the phase I clinical trial, which reflects the high selectivity and strong inhibition of Cetagliptin. The beautiful phase I clinical trial data have provided the foundation for the later clinical trial research of Cetagliptin.
In 2019, Cetagliptin was officially approved by the National Drug Evaluation Center to “exempt Phase II clinical trials from Phase III trials”, becoming the first DPP-4 inhibitor in the world to pass the quantitative pharmacological model, exempt Phase II clinical trials, and directly carry out Phase III confirmatory trials, which attracted the attention of experts in the field of diabetes at home and abroad.
In October 2022, the unblinding results of Cetagliptin phase III clinical trial showed that the reduction of glycosylated hemoglobin (HbA1c) in Cetagliptin tablet 50mg group reached the main clinical end point at the end of the 24th week, which was significantly superior to the control group. After 28 weeks, the Cetagliptin 100mg dose group also showed good drug safety, and the incidence of adverse reactions was similar to that of the placebo group. The clinical trial has shown the advantages of halving the dose but the same efficacy as similar products.
In February 2023, the marketing application (NDA) of Cetagliptin has been accepted by NMPA for the treatment of type 2 diabetes.
The approval of Cetagliptin has attracted much attention, which means that CGeneTech will officially participate in the domestic hot track of DPP-4 inhibitors, and the market of 10 billion statins will usher in new members.
DPP-4 inhibitor track is hot
DPP-4 inhibitors play a hypoglycemic role mainly by inhibiting the degradation of glucagon-like peptide-1 (GLP-1) by DPP-4 enzyme, promoting insulin and glucose dependent secretion, and inhibiting glucagon secretion, which can improve β Cell dysfunction does not increase the risk of hypoglycemia and body weight of patients. Moreover, DPP-4 inhibitor is a “mild and versatile”. It is mild, versatile and safe in reducing blood sugar. It is an oral drug that can be combined with various drugs in the whole process of management.
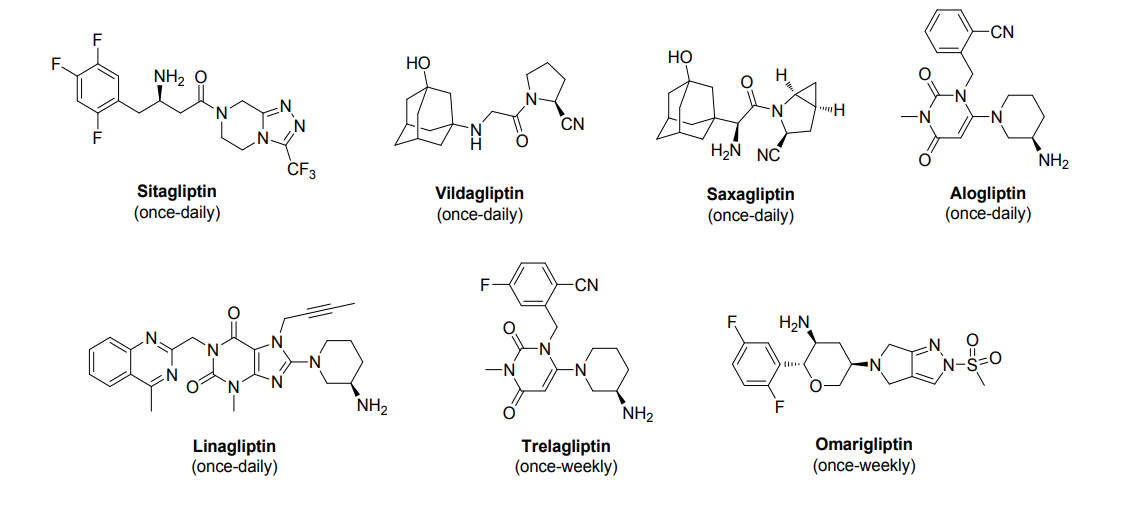
As the current mainstream hypoglycemic drug, DPP-4 inhibitor has become a hot spot in the eyes of major pharmaceutical enterprises. At present, there are five kinds of DPP-4 inhibitors that are taken daily on the market in China: Sigliptin, Viggliptin, Shagliptin, Aggliptin and Liggliptin, and these “five golden flowers” are included in the national health insurance list.
After entering medical insurance, the sales of several products have increased significantly. It is understood that from 2016 to 2022, the annual sales of DPP-4 inhibitors showed a continuous growth trend, with the highest year-on-year growth rate in 2018. In 2021 alone, the domestic sales of DPP-4 inhibitors reached nearly 7 billion yuan.
Sigliptin
Sigliptin is the first oral DPP-4 inhibitor on the market in the world, developed by MSD. It was approved by FDA for listing in October 2006; Sigliptin was approved for listing in China in September 2009; In July 2012, its compound preparation was approved for registration in China.
According to MSD’s annual report, the global market share of Sigliptin has been stable at more than US $3 billion in the past four years, ranking first in the global sales of DPP-4 inhibitors. At present, there are 14 pharmaceutical enterprises in China, including Zhengda Tianqing, Qilu Pharmaceutical, Kelun Pharmaceutical and Zhejiang Pharmaceutical, which have been copied and approved for production.
Viggliptin is the second DPP-4 inhibitor in the world developed by Novartis. In September 2007, Viggliptin was first approved for listing by the European Commission; In August 2011, it was officially approved for listing in China.
According to Novartis annual report, the global sales volume of Vigiletin has fluctuated steadily in recent years, basically maintaining at about 1.1 billion US dollars. The imitative production of Viggliptin in the domestic market is also hot. At present, 18 pharmaceutical enterprises such as Qilu Pharmaceutical, Yangzijiang Pharmaceutical, Jiangsu Haosen Pharmaceutical, Shandong Langnuo Pharmaceutical and Nanjing Shenghe Pharmaceutical have been approved for production. They are worthy of the title of the king of domestic imitative drugs for DPP-4 inhibitors.
Shagliptin was jointly developed by Bristol-Myers Squibb and AstraZeneca. It was approved by FDA for listing in July 2009; In May 2011, Shagliptin was approved for listing in China. Shagliptin’s overseas market share exceeded 20%. At present, there are five pharmaceutical enterprises in China, including Zhengda Tianqing, Qilu Pharmaceutical and Jiangsu Aosaikang Pharmaceutical, whose generic drugs have been approved for production.
Liggliptin was developed by BI. In May 2011, it was approved for listing by the FDA of the United States, and was jointly sold by Berger Ingelheim and Lilly. In March 2013, China approved the import registration of liggliptin. Liggliptin’s overseas market share exceeds 15%. At present, there are 6 pharmaceutical enterprises in China, including Guangdong East Sunshine Pharmaceutical, Yangzijiang Pharmaceutical and Kelun Pharmaceutical, which have been approved for production.
Agiletin
Agiletin was developed by Takeda Pharmaceutical of Japan. Approved for listing in Japan in April 2010; In January 2013, it was approved by the US FDA for listing; In July of the same year, Agiletin obtained the import registration certificate of China. According to the statistics of IQVIA, the sales amount of Agiletin in the Chinese market in 2022 was 52.36 million yuan. At present, 11 pharmaceutical enterprises such as Yabao Pharmaceutical, Ruiyang Pharmaceutical and Guorui Pharmaceutical of the National Pharmaceutical Group have been approved for production.
Throughout the domestic market of DPP-4 inhibitors, the original drugs and generic drugs of the “five golden flowers” are all in the Jianghu. In order to break the competition pattern, pharmaceutical enterprises have also invested in innovative self-research teams.
At present, the research and development of innovative DPP-4 inhibitors is also advancing rapidly. According to the data, in addition to the approval of CGeneTech’s Cetagliptin, many innovative DPP-4 inhibitors (excluding compound preparations) have entered the clinical research stage in China.
TQ-F3083 of Nanjing Shunxin, Shingliptin of Chenxin Pharmaceutical, and Boggliptin of Shandong Baiji Dichang Pharmaceutical are in clinical phase II; Fugliptin of Xinritai, DBPR108 of Shiyao Group, HSK7653 of Hisco and Unigliptin of Yuandong Biological are all in clinical phase III; Hengrui Pharmaceutical’s Retagliptin has submitted its listing application.
Although there are only a few “Ting” who have been approved to market independently developed DPP-4 inhibitors in China, the approval of Cetagliptin will take the lead in ushering in the harvest period of domestic innovative DPP-4 inhibitors, break the monopoly of non-self-developed DPP-4 inhibitors again, and give great confidence to pharmaceutical enterprises engaged in the research and development of DPP-4 inhibitors.
epilogue
The huge market potential of diabetes is like a magnet, attracting pharmaceutical enterprises to participate in the hot domestic track of DPP-4 inhibitors.
As the first oral DPP-4 inhibitor launched in the world and China, Sigliptin has been in the Chinese market for more than ten years, and still dominates the market. According to the Phase I clinical trial study, Cetagliptin has obtained significantly better data than Sigliptin in terms of efficacy, safety, half-life, toxicology and pathology, which will have considerable market persuasion and is expected to help it become a similar Best-in-class product, or change the curve overtaking into a competitive pattern.
Cetagliptin is only one step away from its listing. Not only is CGeneTech full of expectations for it, but also the industry has high expectations. Cetagliptin can be expected in the future, and we also expect more home-made original new “Ting” to come out.
reference material:
1. CGeneTech official website, official account
2. New weapon for treating diabetes (I) – DPP-4 inhibitor, Department of General Medicine, Shenzhen Hospital, University of Hong Kong, December 9, 2020
3. Unique Mechanism, Multi-dimensional Benefits – Mechanism and Clinical Application of DPP-4 Inhibitor, China Medical Forum Endocrinology Today, April 9, 2020
4. DPP-4 inhibitor market may add new force. Can CGeneTech break the “five giants” pattern
5. Market | DPP-4 inhibitor market pattern seen from the withdrawal of the first generic antidiabetic drug from the network of East Sunshine, CPHI Pharmaceutical Online, November 17, 2022
- [1]. Zhou C, et al., Safety, tolerability, pharmacokinetics and pharmacokinetic-pharmacodynamic modeling of cetagliptin in patients with type 2 diabetes mellitus. Front Endocrinol (Lausanne). 2024 Mar 11;15:1359407. [Content Brief][2]. Lu J, et al., In vitro study of the drug-drug interaction potential of cetagliptin and clinical study of pharmacokinetic interaction of cetagliptin and metformin in healthy volunteers. Xenobiotica. 2021 Oct;51(10):1122-1131. [Content Brief]
/////////Cetagliptin, CHINA 2024, APPROVALS 2024, CGeneTec, DIABETES, GTPL13952, CGT 8012,
Cofrogliptin
Cofrogliptin
HSK 7653
- Haisco HSK 7653
- CAS 1844874-26-5
- 466.4 g/mol
- C18H19F5N4O3S
(2R,3S,5R,6S)-2-(2,5-difluorophenyl)-5-(2-methylsulfonyl-4,6-dihydropyrrolo[3,4-c]pyrazol-5-yl)-6-(trifluoromethyl)oxan-3-amine
- (2R,3S,5R,6S)-2-(2,5-Difluorophenyl)-5-(2- (methanesulfonyl)-2,6-dihydropyrrolo(3,4-C)pyrazol- 5(4H)-yl)-6-(trifluoromethyl)oxan-3-amine
- (2R,3S,5R,6S)-2-(2,5-difluorophenyl)-5-[2- (methanesulfonyl)-2,6-dihydropyrrolo[3,4-c]pyrazol- 5(4H)-yl]-6-(trifluoromethyl)oxan-3-amine
- (6R)-5-Amino-2,6-anhydro-1,3,4,5-tetradeoxy-6-C-(2,5-difluorophenyl)-3-(2,6-dihydro-2-(methylsulfonyl)pyrrolo(3,4-C)pyrazol-5(4H)-yl)-1,1,1-trifluoro-D-arabino-hexitol
- (6R)-5-Amino-2,6-anhydro-1,3,4,5-tetradeoxy-6-C-(2,5-difluorophenyl)-3-[2,6-dihydro-2-(methylsulfonyl)pyrrolo[3,4-c]pyrazol-5(4H)-yl]-1,1,1-trifluoro-D-arabino-hexitol
- D-Arabino-hexitol, 5-amino-2,6-anhydro-1,3,4,5-tetradeoxy-6-C-(2,5-difluorophenyl)-3-(2,6-dihydro-2-(methylsulfonyl)pyrrolo(3,4-C)pyrazol-5(4H)-yl)-1,1,1-trifluoro-, (6R)-
- (2r,3s,5r,6s)-2-(2,5-difluorophenyl)-5-[2-(methylsulfonyl)-2,6-dihydropyrrolo[3,4-c]pyrazol-5(4h)-yl]-6-(trifluoromethyl)-tetrahydro-2h-pyran-3-amine
APPROVALS 2024, CHINA 2024, Haisco Pharmaceutical Group Co, Beichangping, DIABETES
Cofrogliptin (developmental name HSK7653) is a long-acting DPP4 inhibitor dosed once every two weeks.[1][2][3][4]
Cofrogliptin (HSK7653) (compound 2), a tetrahydropyran derivative, is a potent oral dipeptidyl aminopeptidase 4 (DPP-4) inhibitor with Long-acting antidiabetic efficacy. Cofrogliptin (compound 2) has a great potential for type 2 diabetes mellitus (T2DM) .
SYN
J Med Chem. 2020 Jul 9;63(13):7108-7126
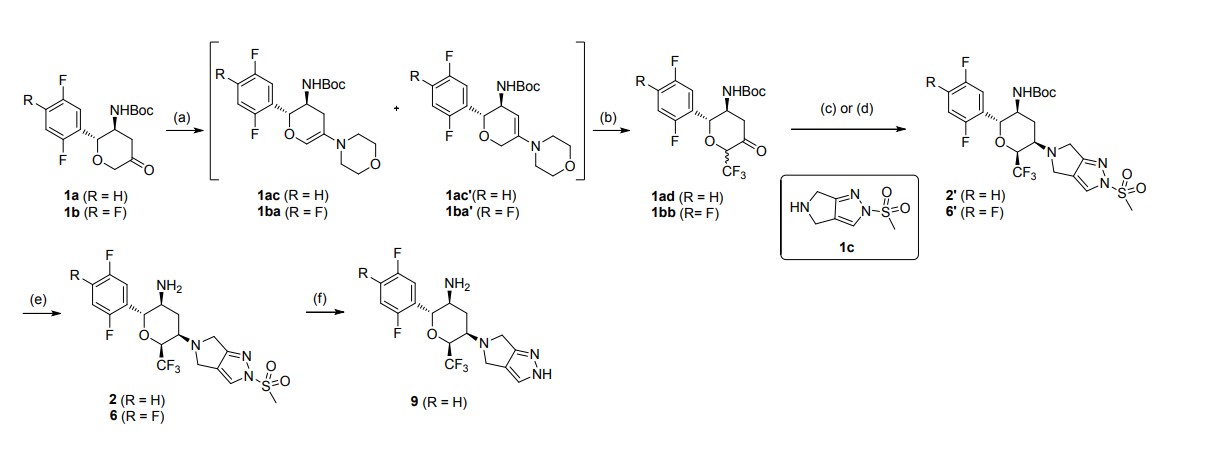
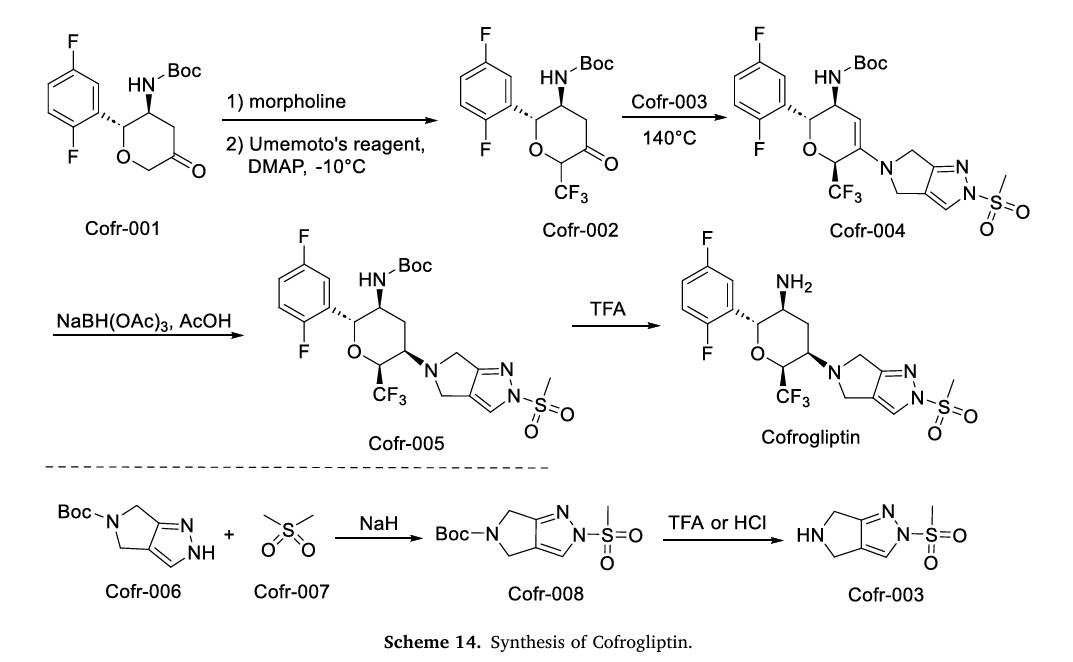
aReagents and conditions: (a) morpholine, toluene, reflux in Dean-Stark appartus; (b)
Umemoto’s reagent, DMAP, DMAc; (c) step 1: 1c, toluene, reflux; step 2: NaBH(OAc)3, CH3COOH, 1,2-DCE; (d) step 1: 1c, CHCl3, reflux in Dean-Stark apparatus; step 2:
NaBH(OAc)3, CH3COOH, 1,2-DCE; (e) TFA, DCM; (f) t-BuOK, THF
Step 2: To a stirred solution of tert-butyl N-[(2R,3S,5R,6S)-2-(2,5-difluorophenyl)-5-
(2-methylsulfonyl-4,6-dihydropyrrolo[3,4-c]pyrazol-5-yl)-6-
(trifluoromethyl)tetrahydropyran-3-yl]carbamate (2′) (407.5 mg, 0.72 mmol) in DCM (6
mL) was added CF3COOH (2 mL) under nitrogen at 0 ℃. After the addition, the reaction
mixture was allowed to warm to room temperature and stirred for 2 h. The reaction mixture
was quenched with a saturated solution of Na2CO3 (15 mL), and extracted with DCM (15
mL × 2). The organic layer was dried over anhydrous Na2SO4 and concentrated in vacuo.
The residue was purified by flash column chromatography (Eluent: DCM/MeOH = 80:1–
30:1) to afford the desired product 2 (301.9 mg, yield: 90%). White solid. Mp: 150.1–152.0
℃. [α]D20 = +17.6 (c = 2.000 in MeOH). Rf= 0.40 (1:15 MeOH/CH2Cl2, TLC).
1H NMR
(400 MHz, CDCl3) δ = 7.71 (s, 1H), 7.20 – 7.12 (m, 1H), 7.10 – 6.97 (m, 2H), 4.63 (d, J =
10.0 Hz, 1H), 4.49 – 4.38 (m, 1H), 4.07 – 3.97 (m, 2H), 3.93 – 3.81 (m, 2H), 3.53 – 3.42
(m, 1H), 3.29 (s, 3H), 3.01 – 2.91 (m, 1H), 2.45 – 2.35 (m, 1H), 2.07 – 1.93 (m, 1H), 1.19
(br. s, 2H). 13C NMR (100 MHz, CDCl3) δ = 163.6, 159.1 (dd, J = 2.3 Hz, 235.8 Hz), 156.6
SYN
https://www.sciencedirect.com/science/article/abs/pii/S0223523424003441
SYN
WO2015192701
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2015192701&_cid=P20-MEQV3M-18104-1

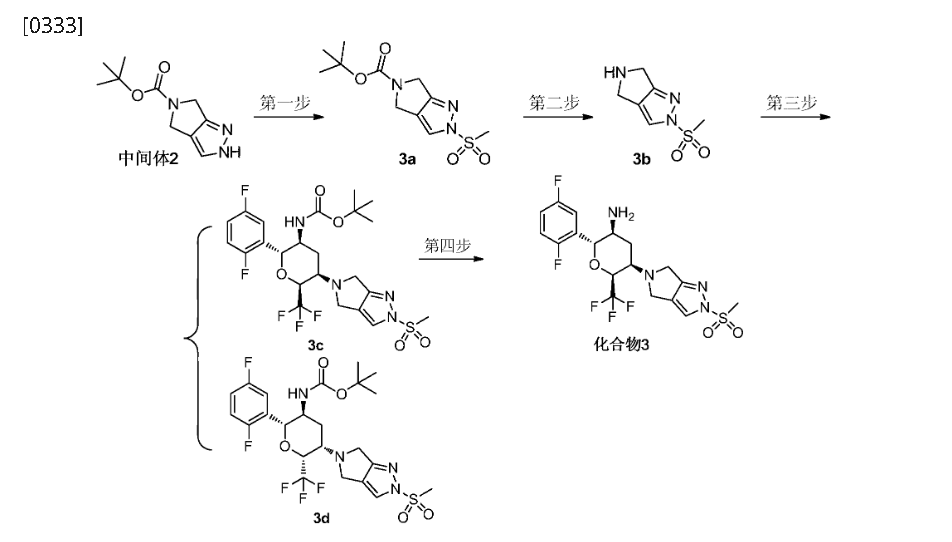
Step 4: (2R,3S,5R,6S)-2-(2,5-difluorophenyl)-5-(2-(methylsulfonyl)-pyrrolo[3,4]pyrazol-5(2H,4H,6H)-yl)-6-(trifluoromethyl)tetrahydro-2H-pyran-3-amine (Compound 3)
[0345]
(2R,3S,5R,6S)-2-(2,5-difluorophenyl)-5-(2-(methylsulfonyl)pyrrolo[3,4-c]pyrazol-5(2H,4H,6H)-yl)-6-(trifluoromethyl)tetrahydro-2H-pyran-3-amine
[0346]3c (410 mg, 0.72 mmol) was dissolved in 6 mL of dichloromethane and 2 mL of trifluoroacetic acid and stirred at room temperature for 1 hour. After completion, saturated aqueous sodium bicarbonate (30 mL) was added to quench the reaction. After separation, the aqueous phase was extracted with ethyl acetate (30 mL x 2). The combined organic phases were dried over anhydrous sodium sulfate, and concentrated. Purification by silica gel column chromatography (dichloromethane/methanol (v/v) = 30:1) afforded compound 3 (250 mg, 75% yield) as a white powder.
[0347]MS m/z(ESI): 467.1[M+1];
[0348]
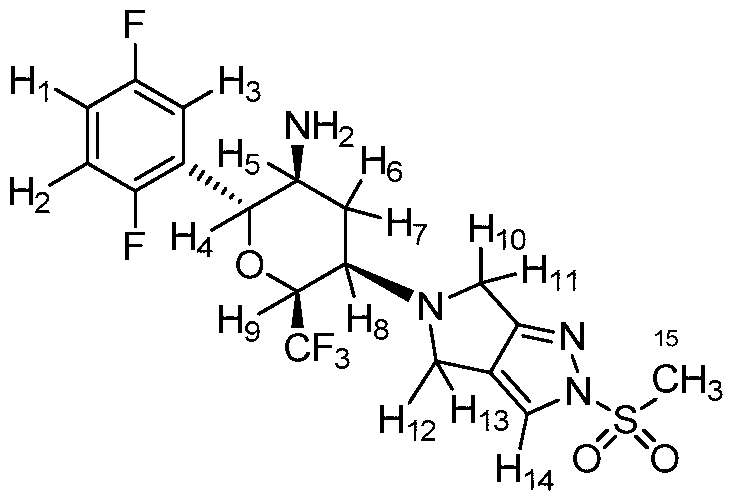
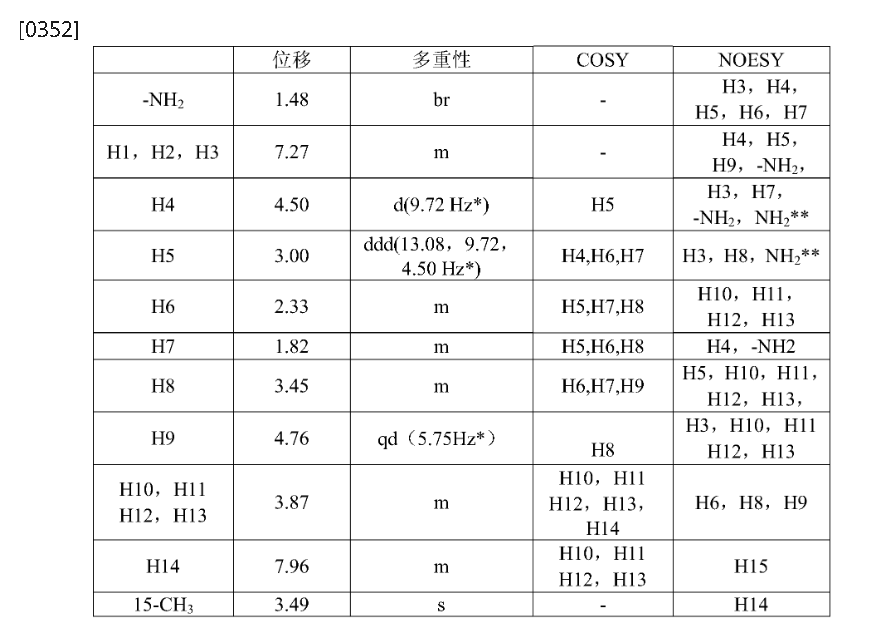
1H NMR(400MHz,DMSO-d 6):δ7.96(m,1H),7.35–7.04(m,3H),4.86–4.63(qd,1H),4.50(d,1H),3.95(dd,2H),3.78(dd,2H),3.49(s,3H),3.45(m,1H),3.00(ddd,1H),2.33(m,1H),1.82(m,1H),1.48(br,2H)。
SYN
Cofrogliptin, developed by Haisco Pharmaceutical Group Co., Ltd., is a novel, ultra-long-acting dipeptidyl peptidase-4 (DPP-4) inhibitor designed for the treatment of T2DM. It is marketed under the brand name (Beichangping). In 2024, the NMPA approved Cofrogliptin for improving blood glucose control in adult patients with T2DM [59].Cofrogliptin acts pharmacologically by inhibiting DPP-4, an enzyme tasked with degrading incretin hormones like glucagon-like peptide-1(GLP-1) and glucose-dependent insulinotropic polypeptide (GIP). By obstructing the degradation of these hormones, it amplifies their activity. This leads to a glucose-dependent rise in insulin secretion and a
corresponding decrease in glucagon release, which in turn improves glycemic control. The clinical efficacy of Cofrogliptin was demonstrated in Phase III, randomized, double-blind, non-inferiority trial
(NCT04556851), where its efficacy and safety were compared to those of daily linagliptin in patients with T2DM whose blood sugar was not well-controlled by metformin. The study reported that Cofrogliptin
administered once every two weeks achieved a reduction in HbA1c comparable to that of daily linagliptin, with a mean decrease of approximately 0.96 % over 24 weeks. Regarding toxicity, Cofrogliptin
was generally well-tolerated [60,61]. The incidence of hypoglycemia was low, and no severe hypoglycemic events directly attributed to the drug were reported.
The synthesis of Cofrogliptin, illustrated in Scheme 14, initiates with trifluoromethylation of Cofr-001 via oxidation, affording Cofr-002 [62]. Nucleophilic addition of Cofr-003 to Cofr-002 yields Cofr-004, followed by NaBH(OAc)3 reduction to Cofr-005. TFA-mediated deprotection of Cofr-005 ultimately delivers Cofrogliptin. Concurrently, Cofr-006 undergoes nucleophilic substitution with Cofr-007 to form Cofr-008, whose deprotection regenerates Cofr-003
[59] L. Gao, F. Bian, T. Pan, H. Jiang, B. Feng, C. Jiang, J. Sun, J. Xiao, P. Yan, L. Ji,
Efficacy and safety of cofrogliptin once every 2 weeks in Chinese patients with type
2 diabetes: a randomized, double-blind, placebo-controlled, phase 3 trial, Diabetes
Obes Metab 27 (2025) 280–290.
[60] C. Cui, F. Cao, I.I. Kong, Q. Wu, F. Li, H. Li, D. Liu, A model-informed approach to
accelerate the clinical development of cofrogliptin (HSK7653), a novel ultralong-
acting dipeptidyl peptidase-4 inhibitor, Diabetes Obes Metab 26 (2024) 592–601.
[61] Q. Ren, L. Li, X. Su, X. Hu, G. Qin, J. Han, Y. Liu, J. Wang, L. Ji, Cofrogliptin once
every 2 weeks as add-on therapy to metformin versus daily linagliptin in patients
with type 2 diabetes in China: a randomized, double-blind, non-inferiority trial,
Diabetes Obes Metab 26 (2024) 5013–5024.
[62] C. Zhang, J. Wang, C. Li, Y. Wei, Amino Pyranoid Ring Derivative as DPP-IV
Inhibitor and Its Preparation, 2015. WO2015192701A1.
AS ON JUNE2025 4.45 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
……
References
- Ji, Linong; Bian, Fang; Pan, Tianrong; Jiang, Hongwei; Jiang, Chengxia; Ren, Qian (20 June 2023). “55-OR: HSK7653, a Novel Ultralong-Acting DPP-4 Inhibitor, as Monotherapy in Patients With Type 2 Diabetes—A Randomized, Double-Blind, Placebo-Controlled Phase III Trial”. Diabetes. 72 (Supplement_1). doi:10.2337/db23-55-OR. S2CID 259433641.
- Zhang, Miao; Zhang, Shudong; Yu, Zhiheng; Yao, Xueting; Lei, Zihan; Yan, Pangke; Wu, Nan; Wang, Xu; Hu, Qin; Liu, Dongyang (October 2023). “Dose decision of HSK7653 oral immediate release tablets in specific populations clinical trials based on mechanistic physiologically-based pharmacokinetic model”. European Journal of Pharmaceutical Sciences. 189 106553. doi:10.1016/j.ejps.2023.106553. PMC 10485820. PMID 37532063.
- Liu, Yang; Yan, Shuai; Liu, Jie; Liu, Hongzhong; Song, Ling; Yao, Xueting; Jiang, Ji; Li, Fangqiong; Du, Ke; Liu, Dongyang; Hu, Pei (May 2023). “Development and validation of an HPLC coupled with tandem mass spectrometry method for the determination of HSK7653, a novel super long-acting dipeptidyl peptidase-4 inhibitor, in human plasma and urine and its application to a pharmacokinetic study”. Biomedical Chromatography. 37 (5): e5607. doi:10.1002/bmc.5607. PMID 36802077. S2CID 257048524.
- Bai, Nan; Wang, Jin; Liang, Wenxin; Gao, Leili; Cui, Wei; Wu, Qinghe; Li, Fangqiong; Ji, Linong; Cai, Yun (6 November 2023). “A Multicenter, Randomized, Double-Blind, Placebo-Controlled, and Dose-Increasing Study on the Safety, Tolerability and PK/PD of Multiple Doses of HSK7653 by Oral Administration in Patients with Type 2 Diabetes Mellitus in China”. Diabetes Therapy. 15 (1): 183–199. doi:10.1007/s13300-023-01496-0. PMC 10786778. PMID 37930584.
| Clinical data | |
|---|---|
| Other names | HSK7653 |
| Legal status | |
| Legal status | Investigational |
| Identifiers | |
| IUPAC name | |
| CAS Number | 1844874-26-5 |
| PubChem CID | 118613788 |
| ChemSpider | 115037226 |
| UNII | LH4G6K6NKP |
| ChEMBL | ChEMBL4646510 |
| Chemical and physical data | |
| Formula | C18H19F5N4O3S |
| Molar mass | 466.43 g·mol−1 |
- [1]. International Nonproprietary Names for Pharmaceutical Substances (INN)[2]. Chen Zhang, et al. Design, Synthesis, and Evaluation of a Series of Novel Super Long-Acting DPP-4 Inhibitors for the Treatment of Type 2 Diabetes. J Med Chem. 2020 Jul 9;63(13):7108-7126. [Content Brief]
///////Cofrogliptin, APPROVALS 2024, CHINA 2024, Haisco Pharmaceutical Group Co, Beichangping, DIABETES, HSK 7653, Haisco HSK 7653, 1844874-26-5
Janagliflozin
Janagliflozin
WeightAverage: 460.95
Monoisotopic: 460.1652664
Chemical FormulaC25H29ClO6
- WK4RT85HCA
- XZP-5695
- UNII-WK4RT85HCA
- 1800115-22-3
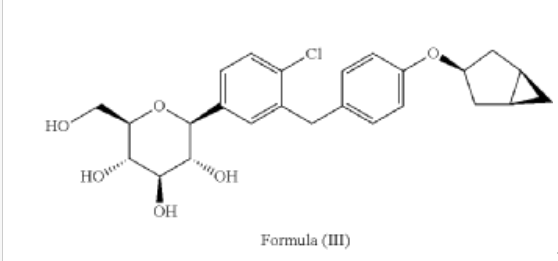
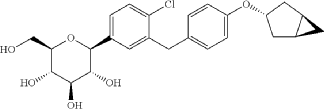
- (2S,3R,4R,5S,6R)-2-[3-[[4-[[(1S,5R)-3-bicyclo[3.1.0]hexanyl]oxy]phenyl]methyl]-4-chlorophenyl]-6-(hydroxymethyl)oxane-3,4,5-triol
- D-Glucitol, 1,5-anhydro-1-C-(3-((4-((1alpha,3alpha,5alpha)-bicyclo(3.1.0)hex-3-yloxy)phenyl)methyl)-4-chlorophenyl)-, (1S)-
- (2S,3R,4R,5S,6R)-2-[3-[[4-[[(1S,5R)-3-bicyclo[3.1.0]hexanyl]oxy]phenyl]methyl]-4-chlorophenyl]-6-(hydroxymethyl)oxane-3,4,5-triol
- D-GLUCITOL, 1,5-ANHYDRO-1-C-(3-((4-((1.ALPHA.,3.ALPHA.,5.ALPHA.)-BICYCLO(3.1.0)HEX-3-YLOXY)PHENYL)METHYL)-4-CHLOROPHENYL)-, (1S)-
- (2S,3R,4R,5S,6R)-2-(3-(4-(((1R,3s,5S)-bicyclo[3.1.0]hexan-3-yl)oxy)benzyl)-4-chlorophenyl)-6-(hydroxymethyl)tetrahydro-2H-pyran-3,4,5-triol
China 2024, approvals 2024, Jilin Huisheng Biopharmaceutical Co, sihuan, SGLT2 inhibitors, Huiyoujing
Janagliflozin is an SGLT2 inhibitor developed by Sihuan Pharmaceutical.[1][2][3][4][5][6] It is approved in China for the treatment of type 2 diabetes.[7]
PAPER
https://www.thieme-connect.de/products/ejournals/abstract/10.1055/s-0042-1751524
(71) (a) Wu, F. US9315438B2, 2016. (b) Wu, F. EP2891654A1, 2014.
Initially, the two advanced intermediates were synthesized and then coupled under cryogenic conditions using nBuLi. The construction of 242 commences with the reaction of 5-bromo-2-chlorobenzoic acid (26c) with oxalyl chloride and a catalytic amount of DMF in DCM, yielding the acid chloride derivative 26c′. This intermediate is then subjected to Friedel–Crafts acylation with anisole to produce 240 in
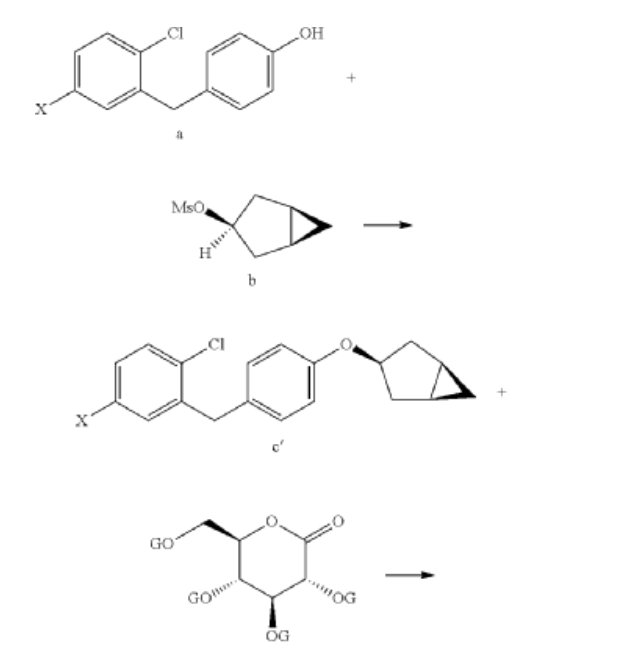
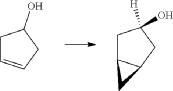
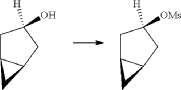
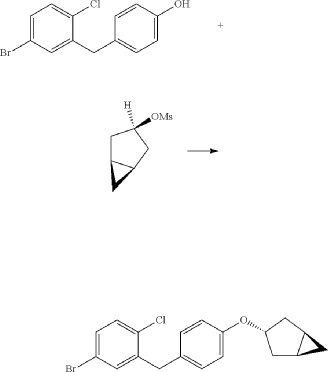
71% yield. Subsequent reduction of 240 was carried out using boron trifluoride–diethyl etherate and triethylsilane in a DCM/acetonitrile mixture, leading to the formation of 241 in an excellent yield. Demethylation of compound 241 is accomplished using boron tribromide at low temperature, resulting in 242 with a yield of 97%. On the other hand, the synthesis of 245 involves two steps starting from commercially available cyclopent-3-en-1-ol (243). The Simmons Smith cyclopropanation of 243 is performed using a mixture of trifluoroacetic acid, diiodomethane, and diethylzinc in DCM, providing 244 with a yield of 48%. Compound 244 is then further treated with methanesulfonyl chloride to give the mesylated compound 245 in a yield of 68%. Subse quently, 4-(5-bromo-2-chlorobenzyl)phenol (242) is allowed to react with 245 in the presence of NMP, cesium carbonate, and BTEAC (benzyltriethylammonium chloride) to give 246. The next step involves a lithium–halogen exchange on
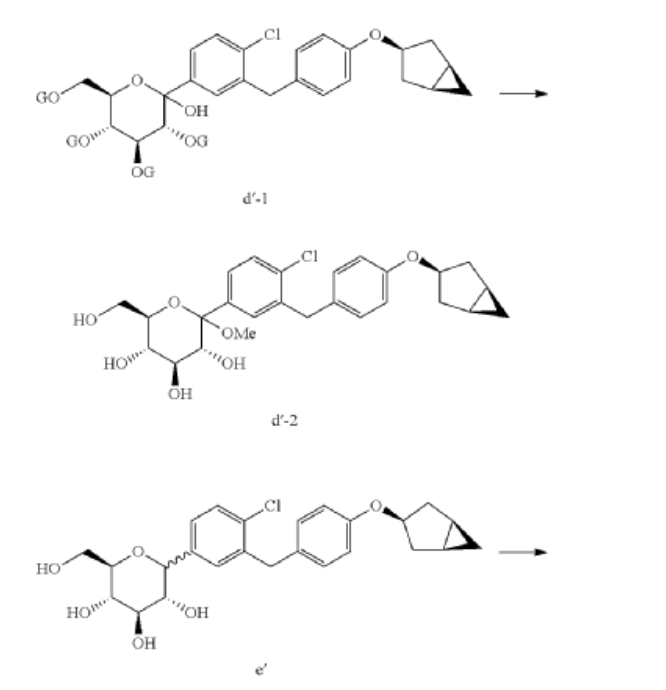
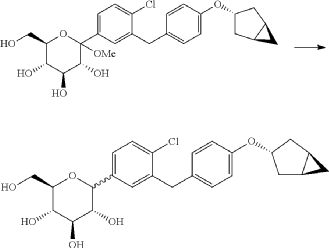
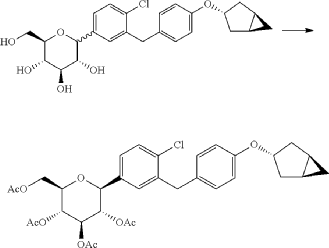
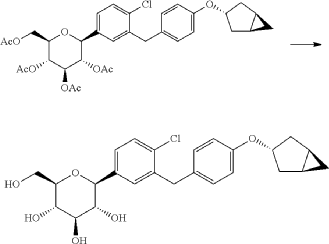
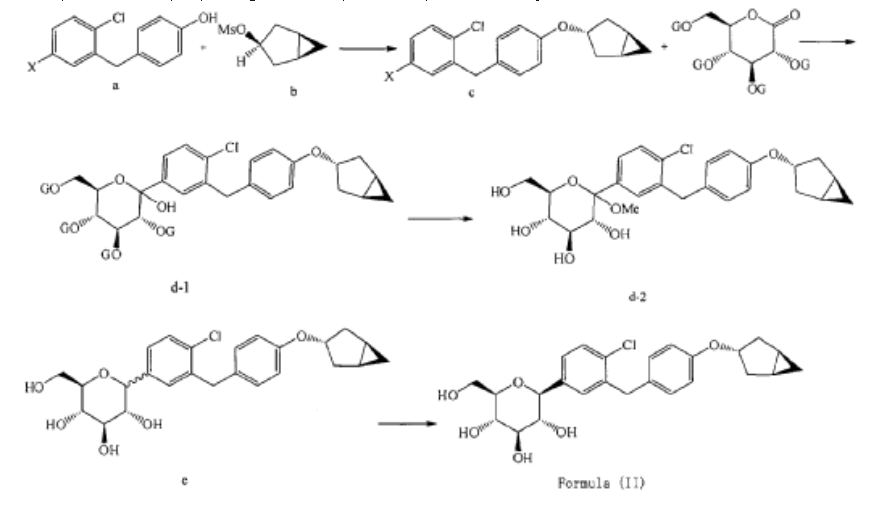
246 using n-butyllithium, with addition to 22 at –78 °C affording the hydroxy intermediate. Methylation of this hydroxy intermediate using methanesulfonic acid and methanol provides 247 in 98% yield. Reduction of 247 using borontrifluoride–diethyl etherate and triethylsilane at –78 °C furnishes 248. To achieve the desired isomer, all of the hydroxy groups of compound 248 were protected using acetic anhydride, DMAP, and pyridine in DCM at 0 °C to give the O-acylated compound 249. In the final step, 249 is hydrolyzed us ing lithium hydroxide monohydrate in a mixed solvent consisting of methanol, THF, and water to provide the desired compound janagliflozin (14) in a yield of 91%. This truncated synthetic route is protection-group-free, and is well suited for scale-up. The drawback of the synthetic route is
the late-stage enrichment of the desired isomer in the final product via acylated derivative 249. The poor isolated yield of 249 is not commercially favored due to low throughput and an increase in raw material and production costs.

PAPER
https://pubs.acs.org/doi/10.1021/acs.oprd.8b00017
SYN
https://www.sciencedirect.com/science/article/abs/pii/S022352342400223X
PAT
https://patentscope.wipo.int/search/en/detail.jsf?docId=US142552820&_cid=P11-MEPJES-88258-1
Example 1
Preparation of (2S,3R,4R,5S,6R)-2-(3-(4-(((1R,3s,5S)-bicyclo[3.1.0]hexan-3-yl)oxy)benzyl)-4-chlorophenyl)-6-(hydroxymethyl)tetrahydro-2H-pyran-3,4,5-triol (Formula II)
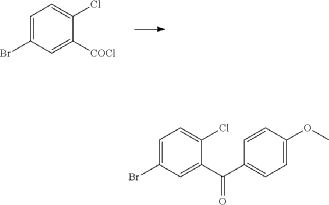
(1) Preparation of 5-bromo-2-chlorobenzoyl chloride

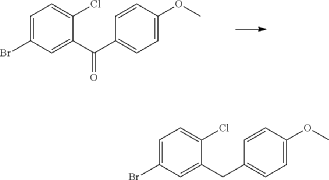
(2) Preparation of (5-bromo-2-chlorophenyl)(4-methoxyphenyl)methanone
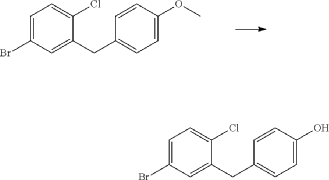
(3) Preparation of 4-bromo-1-chloro-2-(4-methoxybenzyl)benzene
(4) Preparation of 4-(5-bromo-2-chlorobenzyl)phenol
(5) Preparation of (1R,3r,5S)-bicyclo[3.1.0]hexan-3-ol
(6) Preparation of (1R,3r,5S)-bicyclo[3.1.0]hexan-3-yl methanesulfonate
(7) Preparation of (1R,3s,5S)-3-(4-(5-bromo-2-chlorobenzyl)phenyloxy)bicyclo[3.1.0]hexane
(8) Preparation of (3R,4S,5R,6R)-3,4,5-tri((trimethylsilyl)oxy)-6-(((trimethylsilyl)oxy)methyl)tetrahydro-2H-pyran-2-one
(9) Preparation of (3R,4S,5S,6R)-2-(3-(4-(((1R,3s,5S)-bicyclo[3.1.0]hexan-3-yl)oxy)benzyl)-4-chlorophenyl)-6-(hydroxymethyl)-2-methoxytetrahydro-2H-pyran-3,4,5-triol
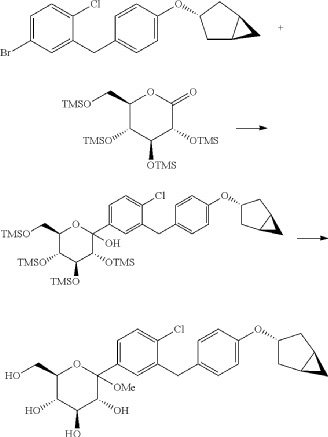
(10) Preparation of (3R,4R,5S,6R)-2-(3-(4-(((1R,3s,5S)-bicyclo[3.1.0]hexan-3-yl)oxy)benzyl)-4-chlorophenyl)-6-(hydroxymethyl)tetrahydro-2H-pyran-3,4,5-triol
(11) Preparation of (2R,3R,4R,5S,6S)-2-(acetoxymethyl)-6-(3-(4-(((1R,3s,5S)-bicyclo[3.1.0]hexan-3-yl)oxy)benzyl)-4-chlorophenyl)tetrahydro-2H-pyran-3,4,5-triyl triacetate
(12) Preparation of (2S,3R,4R,5 S,6R)-2-(3-(4-(((1R,3s,5S)-bicyclo[3.1.0]hexan-3-yl)oxy)benzyl)-4-chlorophenyl)-6-(hydroxymethyl)tetrahydro-2H-pyran-3,4,5-triol
PAT
EP2891654
https://patentscope.wipo.int/search/en/detail.jsf?docId=EP142501978&_cid=P20-MEQIAN-96633-1
[0027] The compound represented by formula (II) as defined hereinbefore, lab-made, its chemical name and preparation process are described in the following Example 1.
Reference compound 1: Compound 4 as described in the PCT application WO2013/000275A1, lab-made (with reference to the PCT application WO2013/000275A1), its structure is as follows:
Compound 4, i.e. the compound represented by formula (I).
Reference compound 2: Compound 22 as described in the PCT application WO2013/000275A1, lab-made (with reference to the PCT application WO2013/000275A1), its structure is as follows:
Compound 22.
(12) Preparation of
[0057] (2 S,3 R,4 R,5 S,6 R)-2-(3-(4-(((1 R,3 s,5 S)-bicyclo[3.1.0]hexan-3-yl)oxy)benzyl)-4-chlorophenyl)-6-(hydr oxymethyl)tetrahydro-2 H-pyran-3,4,5-triol

[0058] (2 R,3 R,4 R,5 S,6 S)-2-(acetoxymethyl)-6-(3-(4-(((1 R,3 s,5 S)-bicyclo[3.1.0]hexan-3-yl)oxy)benzyl)-4-chlo rophenyl)tetrahydro-2 H-pyran-3,4,5-triyl triacetate (81g, 0.129mol) was dissolved in a mixed solvent of tetrahydrofuran (313mL), methanol (470mL) and water (156mL). To the resulting mixture was added lithium hydroxide monohydrate (6.32g, 150mmol). The mixture was stirred at room temperature overnight. TLC indicated the completion of reaction. The solvent was removed from the reaction mixture by rotary evaporation. The residual reaction mixture was dissolved with ethyl acetate (400mL). The organic phase was washed with an aqueous saturated sodium chloride solution, with an aqueous KHSO 4 solution, and with water twice, dried over anhydrous sodium sulphate, and evaporated by rotation. The residue was purified with C18 reverse phase preparative chromatography to produce 54.2g of a final product in a yield of 91%.
Formula: C 25H 29ClO 6 Mw: 460.95 LC-MS( m/ z): 478.3 [M+NH 4] +
1H-NMR (400MHz, MeOD) δ: 7.35-7.26 (m, 3H), 7.08-7.06 (d, 2H), 6.76-6.74 (d, 2H), 4.45-4.41 (m, 1H), 4.10-4.00 (m, 3H), 3.89-3.88 (d, 1H), 3.71-3.69 (m, 1H), 3.45-3.38 (m, 3H), 3.31-3.26 (m, 1H), 2.34-2.29 (m, 2H), 1.87-1.81 (m, 2H), 1.37-1.33 (m, 2H), 0.43-0.42 (m, 1H), 0.11-0.10 (m, 1H).
SYN
European Journal of Medicinal Chemistry 291 (2025) 117643
Janagliflozin, engineered by Jilin Huisheng Biopharmaceutical Co., Ltd., a subsidiary under the umbrella of Sihuan Pharmaceutical Holdings Group, falls within the category of oral sodium-glucose co-transporter 2(SGLT2) inhibitors. This agent has been specifically designed with the aim of optimizing glycemic regulation in the adult population grappling with type 2 diabetes mellitus (T2DM) [54]. It is marketed under the brand name Huiyoujing. In 2024, the NMPA gave its approval for Janagliflozin, indicated for adult patients with T2DM, where it can be employed either as a standalone treatment (monotherapy) or in combination with metformin to optimize blood glucose regulation [55]. The clinical effectiveness of Janagliflozin was substantiated through a Phase III clinical trial (NCT03811548). This trial specifically assessed its application as a monotherapy in Chinese patients suffering from T2DM
whose blood glucose was not well – managed via diet and exercise alone. The findings of the study indicated notable decreases in glycated hemoglobin levels. Concurrently, improvements were observed in both body weight and blood pressure. Collectively, these outcomes serve as evidence of the drug’s ability to enhance glycemic regulation [56]. Regarding safety, Janagliflozin was generally well-tolerated. In line with the well-established safety characteristics of SGLT2 inhibitors, the frequently encountered adverse events associated with this treatment were urinary tract infections and genital mycotic infections. No serious adverse events were reported during the trial [57].
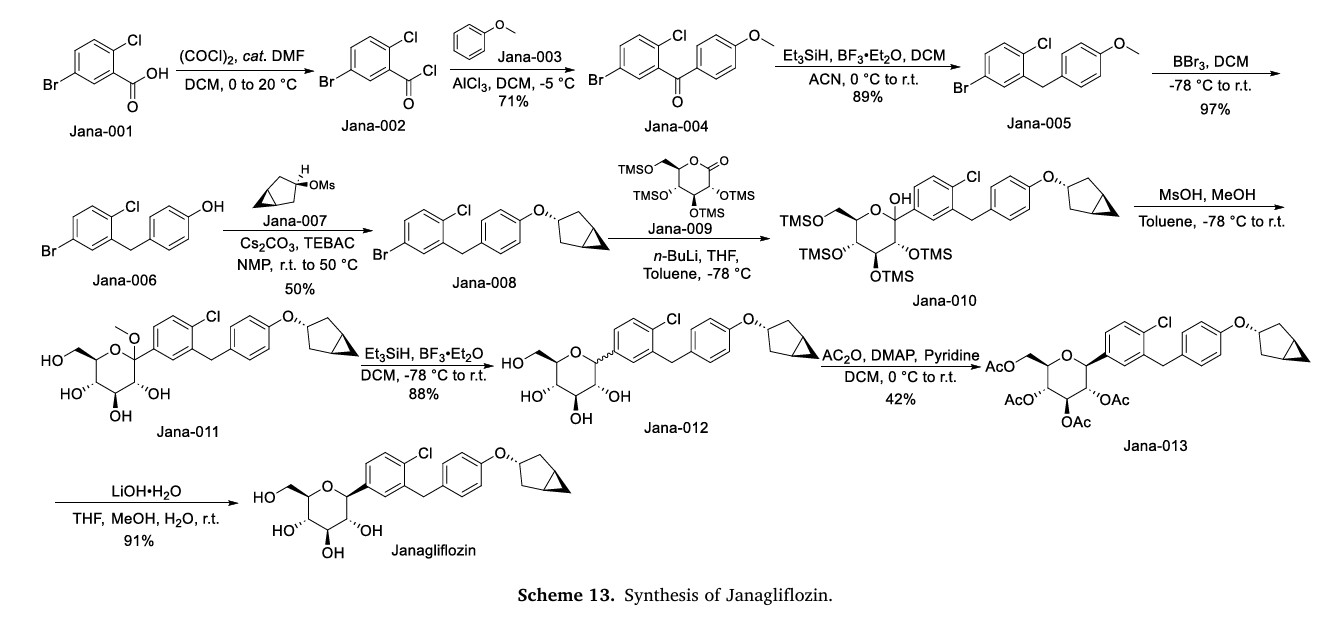
The synthesis of Janagliflozin, depicted in Scheme 13, commences with the acylation of 5-bromo-2-chlorobenzoic acid (Jana-001) using oxalyl chloride, yielding the acyl chloride intermediate Jana-002 [58]. Friedel-Crafts acylation of Jana-002 with anisole (Jana-003) affords ketone Jana-004. Subsequent reduction of the carbonyl group in Jana-004 produces Jana-005. Demethylation of Jana-005 with BBr3
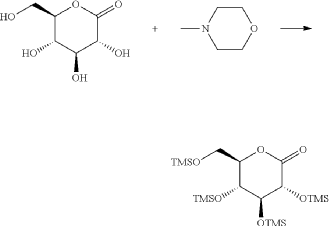
generates phenol Jana-006, which undergoes substitution with intermediate Jana-007 to form ether Jana-008. Addition of gluconolactone (Jana-009) to Jana-008 affords Jana-010, where concurrent TMS
deprotection during etherification yields Jana-011. Reduction of Jana-011 using Et3SiH/BF3.ET2Oproduces Jana-012which is sequentially esterified with Ac2O , and hydrolyzed under LiOH conditions, ultimately yielding Janagliflozin
[54] L. Gao, Z. Cheng, B. Su, X. Su, W. Song, Y. Guo, L. Liao, X. Chen, J. Li, X. Tan, F. Xu,
S. Pang, K. Wang, J. Ye, Y. Wang, L. Chen, J. Sun, L. Ji, Efficacy and safety of
janagliflozin as add-on therapy to metformin in Chinese patients with type 2
diabetes inadequately controlled with metformin alone: a multicentre,
randomized, double-blind, placebo-controlled, phase 3 trial, Diabetes Obes Metab
25 (2023) 785–795.
[55] L. Ji, X. Jiang, Q. Hao, Z. Cheng, K. Wang, S. Pang, M. Liu, Y. Guo, X. Chen, X. Su,
T. Ning, J. Liu, F. Bian, Y. Li, Z. Zhang, W. Song, J. Sun, Efficacy and safety of
janagliflozin monotherapy in Chinese patients with type 2 diabetes mellitus
inadequately controlled on diet and exercise: a multicentre, randomized, double-
blind, placebo-controlled, phase 3 trial, Diabetes Obes Metab 25 (2023)
1229–1240.
[56] L. Song, X. Wang, J. Sun, X. Hu, H. Li, P. Hu, D. Liu, A model-informed approach to
accelerate the clinical development of janagliflozin, an innovative SGLT2 inhibitor,
Clin. Pharmacokinet. 62 (2023) 505–518.
[57] Canagliflozin, Drugs and Lactation Database (Lactmed®), National Institute of
Child Health and Human Development, Bethesda (MD), 2006.
[58] F. Wu, Optically Pure benzyl-4-chlorophenyl-C-glucoside Derivatives as SGLT
Inhibitors (Diabetes Mellitus), 2015. EP2891654.
AS ON JUNE2025 4.45 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
……
References
- Song, Ling; Yao, Xueting; Liu, Yang; Zhong, Wen; Jiang, Ji; Liu, Hongzhong; Zhou, Huimin; Shi, Chongtie; Zong, Kaiqi; Wang, Chong; Ma, Chuanxiang; Liu, Dongyang; Hu, Pei (April 2020). “Translational prediction of first-in-human pharmacokinetics and pharmacodynamics of janagliflozin, a selective SGLT2 inhibitor, using allometric scaling, dedrick and PK/PD modeling methods”. European Journal of Pharmaceutical Sciences. 147: 105281. doi:10.1016/j.ejps.2020.105281. S2CID 212405270.
- Liu, Dongyang; Song, Ling; Wang, Xiaoxu; Liu, Xu; Cao, Fangrui; Liu, Hongzhong; Ding, Yanhua; Xiao, Xinhua; Jiang, Ji; Hu, Pei (1 June 2019). “154-LB: Accelerating Clinical Development of Janagliflozin, a Novel Antidiabetic Drug, Using Model-Informed Drug Development Strategy”. Diabetes. 68 (Supplement_1). doi:10.2337/db19-154-LB. S2CID 195440798.
- Zhao, Hengli; Wei, Yilin; He, Kun; Zhao, Xiaoyu; Mu, Hongli; Wen, Qing (December 2022). “Prediction of janagliflozin pharmacokinetics in type 2 diabetes mellitus patients with liver cirrhosis or renal impairment using a physiologically based pharmacokinetic model”. European Journal of Pharmaceutical Sciences. 179: 106298. doi:10.1016/j.ejps.2022.106298. PMID 36162752. S2CID 252505056.
- Zhao, Hengli; Zhao, Zhirui; He, Kun; Mi, Nianrong; Lou, Kai; Dong, Xiaolin; Zhang, Wenyu; Sun, Jingfang; Hu, Xinyu; Pang, Shuguang; Cheng, Hong; Wen, Qing (August 2023). “Pharmacokinetics, Pharmacodynamics and Safety of Janagliflozin in Chinese Type 2 Diabetes Mellitus Patients with Renal Impairment”. Clinical Pharmacokinetics. 62 (8): 1093–1103. doi:10.1007/s40262-023-01256-0. PMID 37284974. S2CID 259097798.
- Gao, Leili; Cheng, Zhifeng; Su, Benli; Su, Xiuhai; Song, Weihong; Guo, Yushan; Liao, Lin; Chen, Xiaowen; Li, Jiarui; Tan, Xingrong; Xu, Fangjiang; Pang, Shuguang; Wang, Kun; Ye, Jun; Wang, Yuan; Chen, Lili; Sun, Jingfang; Ji, Linong (March 2023). “Efficacy and safety of janagliflozin as add‐on therapy to metformin in Chinese patients with type 2 diabetes inadequately controlled with metformin alone: A multicentre, randomized, double‐blind, placebo‐controlled, phase 3 trial”. Diabetes, Obesity and Metabolism. 25 (3): 785–795. doi:10.1111/dom.14926. PMID 36433709. S2CID 253967474.
- Ji, Linong; Jiang, Xiaozhen; Hao, Qingshun; Cheng, Zhifeng; Wang, Kun; Pang, Shuguang; Liu, Meiying; Guo, Yushan; Chen, Xiaowen; Su, Xiuhai; Ning, Tao; Liu, Jie; Bian, Fang; Li, Yulan; Zhang, Zhinong; Song, Weihong; Sun, Jingfang (May 2023). “Efficacy and safety of janagliflozin monotherapy in Chinese patients with type 2 diabetes mellitus inadequately controlled on diet and exercise: A multicentre, randomized, double‐blind, placebo‐controlled, Phase 3 trial”. Diabetes, Obesity and Metabolism. 25 (5): 1229–1240. doi:10.1111/dom.14971. PMID 36594724. S2CID 255474211.
- “NMPA approves China’s second homegrown SGLT2 inhibitor janagliflozin”. bioworld.com. January 23, 2024.
| Legal status | |
|---|---|
| Legal status | Rx in China; investigational elsewhere |
| Identifiers | |
| IUPAC name | |
| CAS Number | 1800115-22-3 |
| PubChem CID | 91820686 |
| DrugBank | DB16209 |
| UNII | WK4RT85HCA |
| Chemical and physical data | |
| Formula | C25H29ClO6 |
| Molar mass | 460.95 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| SMILES | |
| InChI | |
///////////Janagliflozin, china 2024, approvals 2024, Jilin Huisheng Biopharmaceutical Co, sihuan, SGLT2 inhibitors, Huiyoujing, WK4RT85HCA, XZP 5695, UNII-WK4RT85HCA, 1800115-22-3
SYN
SYNTHESIS 2024, 56, 906–943
synthesis of janagliflozin (14) was achieved through an eleven-step process in an overall yield of 3% (Scheme 45).71 Initially, the two advanced intermediates were synthesized and then coupled under cryogenic conditions using nBuLi. The construction of 242 commences with the reaction of 5-bromo-2-chlorobenzoic acid (26c) with oxalyl chloride and a catalytic amount of DMF in DCM, yielding the acid
chloride derivative 26c′. This intermediate is then subjected to Friedel–Crafts acylation with anisole to produce 240 in 71% yield. Subsequent reduction of 240 was carried out using boron trifluoride–diethyl etherate and triethylsilane in a DCM/acetonitrile mixture, leading to the formation of 241 in an excellent yield. Demethylation of compound 241 is accomplished using boron tribromide at low temperature, re
sulting in 242 with a yield of 97%. On the other hand, the synthesis of 245 involves two steps starting from commercially available cyclopent-3-en-1-ol (243). The Simmons Smith cyclopropanation of 243 is performed using a mixture of trifluoroacetic acid, diiodomethane, and diethylzinc in DCM, providing 244 with a yield of 48%. Compound 244 is then further treated with methanesulfonyl chloride to
give the mesylated compound 245 in a yield of 68%. Subsequently, 4-(5-bromo-2-chlorobenzyl)phenol (242) is allowed to react with 245 in the presence of NMP, cesium carbonate, and BTEAC (benzyltriethylammonium chloride) to give 246. The next step involves a lithium–halogen exchange on
246 using n-butyllithium, with addition to 22 at –78 °C affording the hydroxy intermediate. Methylation of this hydroxy intermediate using methanesulfonic acid and methanol provides 247 in 98% yield. Reduction of 247 using boron trifluoride–diethyl etherate and triethylsilane at –78 °C furnishes 248. To achieve the desired isomer, all of the hydroxy groups of compound 248 were protected using acetic anhydride, DMAP, and pyridine in DCM at 0 °C to give the O-acylated compound 249. In the final step, 249 is hydrolyzed us ing lithium hydroxide monohydrate in a mixed solvent consisting of methanol, THF, and water to provide the desired compound janagliflozin (14) in a yield of 91%. This truncated synthetic route is protection-group-free, and is well suited for scale-up. The drawback of the synthetic route is
the late-stage enrichment of the desired isomer in the final product via acylated derivative 249. The poor isolated yield of 249 is not commercially favored due to low throughput and an increase in raw material and production costs

(71) (a) Wu, F. US9315438B2, 2016. (b) Wu, F. EP2891654A1, 2014.
Zorifertinib
Zorifertinib
AZD 3759
CAS 1626387-80-1, 67SX9H68W2
WeightAverage: 459.91
Monoisotopic: 459.1473455
Chemical FormulaC22H23ClFN5O3
[4-(3-chloro-2-fluoroanilino)-7-methoxyquinazolin-6-yl] (2R)-2,4-dimethylpiperazine-1-carboxylate
- [4-(3-chloro-2-fluoroanilino)-7-methoxyquinazolin-6-yl] (2R)-2,4-dimethylpiperazine-1-carboxylate
- (4-(3-chloro-2-fluoroanilino)-7-methoxyquinazolin-6-yl) (2R)-2,4-dimethylpiperazine-1-carboxylate
- (R)-4-((3-chloro-2-fluorophenyl)amino)-7-methoxyquinazolin-6-yl 2,4-dimethylpiperazine-1-carboxylate
- 4-[(3-CHLORO-2-FLUOROPHENYL)AMINO]-7-METHOXYQUINAZOLIN-6-YL (2R)-2,4-DIMETHYLPIPERAZINE-1-CARBOXYLATE
China 2024, APPROVALS 2024, Alpha Biopharma, ASTRA ZENECA, Zorifer,
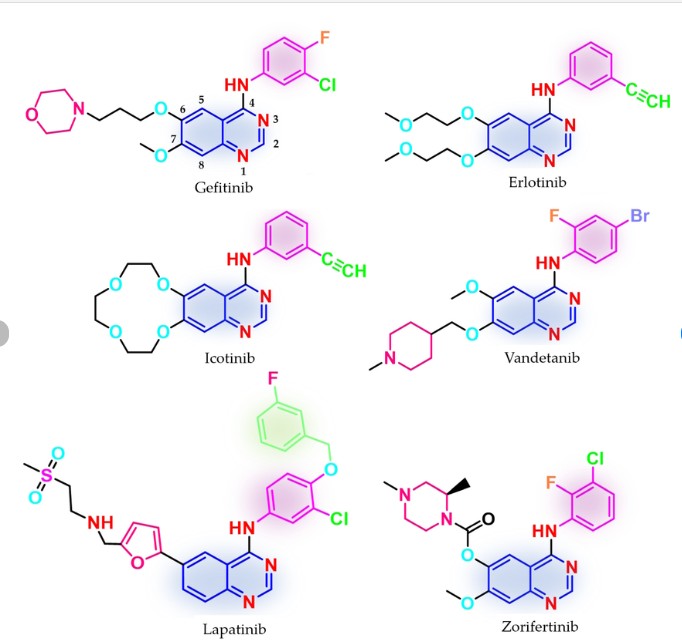
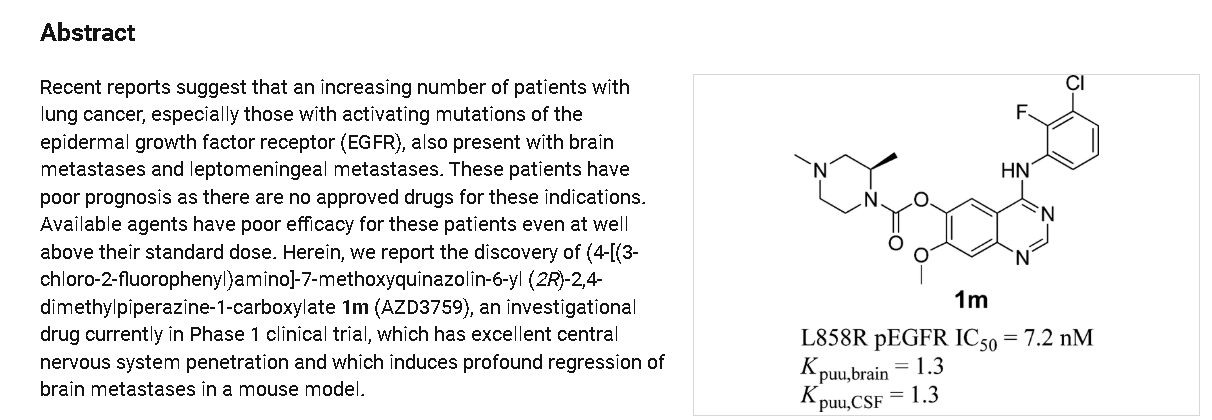
Zorifertinib (AZD3759) is a drug for the treatment of cancer.[1] In China, it was approved in 2024 for locally advanced or metastatic non-small-cell lung cancer (NSCLC) that has epidermal growth factor receptor exon 19 deletion or exon 21 L858R substitution mutations and central nervous system (CNS) metastases.[2]
Zorifertinib is an orally available inhibitor of the epidermal growth factor receptor (EGFR), with potential antineoplastic activity. Upon oral administration, zorifertinib binds to and inhibits the activity of EGFR as well as certain mutant forms of EGFR. This prevents EGFR-mediated signaling, and may lead to both induction of cell death and inhibition of tumor growth in EGFR-overexpressing cells. EGFR, a receptor tyrosine kinase mutated in many tumor cell types, plays a key role in tumor cell proliferation and tumor vascularization.
SYN
J. Med. Chem. 58 (2015) 8200–8215.
https://pubs.acs.org/doi/10.1021/acs.jmedchem.5b01073
SYN
European Journal of Medicinal Chemistry 291 (2025) 117643
Zorifertinib, developed by AstraZeneca as AZD3759, is a novel EGFR TKI designed to effectively penetrate the blood-brain barrier (BBB) [44,45]. In 2018, Alpha Biopharma, in collaboration with AstraZeneca, advanced its development. In 2024, the NMPA gave its approval to zorifertinib hydrochloride tablets, which are sold under the brand name Zorifer. This approval is for the use of these tablets in the first-line treatment of adult patients who have the following conditions: they
have locally advanced or metastatic NSCLC with either EGFR exon 19 deletion or exon 21 L858R substitution mutations, and also have CNSmetastases [45]. Zorifertinib exerts its pharmacological action through the selective inhibition of EGFR tyrosine kinase activity, with a particular focus on mutational forms such as L858R and exon 19 deletions. In contrast to several other tyrosine kinase inhibitors (TKIs), it does not serve as a substrate for BBB efflux transporters, namely P-glycoprotein (P-gp) and breast cancer resistance protein (BCRP). This unique property enables zorifertinib to reach elevated concentrations within brain tissue and cerebrospinal fluid. As a result, it can effectively target and
act against CNS metastases [44,45]. The clinical efficacy of zorifertinib was demonstrated in the EVEREST study (NCT03653546), a random ized, open-label, international multicenter Phase II/III trial. The study
enrolled 492 patients with EGFR-mutant NSCLC and CNS metastases. Results showed that zorifertinib significantly improved systemic PFS to 9.6 months compared to 6.9 months with first-generation EGFR-TKIs, reducing the risk of disease progression or death by 28 %. Intracranial PFS was notably extended to 15.2 months versus 8.3 months in the control group. The ORR was 68.6 % for zorifertinib compared to 58.4 % for the control. Regarding toxicity, zorifertinib exhibited a manageable safety profile. The incidence of treatment-related adverse events (TRAEs) was similar between the zorifertinib and control groups (97.7 %vs. 94.0 %), with grade ≥3 TRAEs occurring in 65.9 % of patients receiving zorifertinib compared to 18.3 % in the control group. No new safety signals were identified, indicating an acceptable tolerability for patients. The approval of zorifertinib offers a significant advancement in
the treatment of EGFR-mutant NSCLC patients with CNS metastases,providing an effective therapeutic option capable of addressing both systemic and intracranial disease [44].
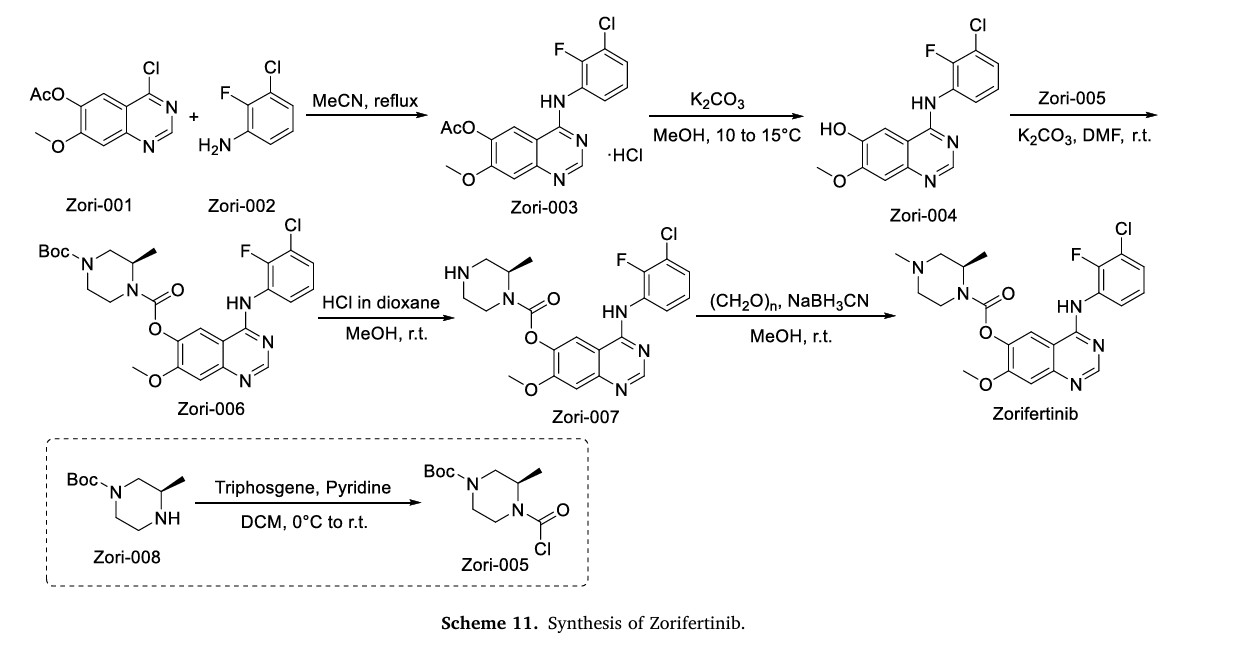
The synthesis of Zorifertinib, depicted in Scheme 11, initiates with nucleophilic substitution between Zori-001 and Zori-002 in MeCN, affording Zori-003 [46]. Hydrolysis of the ester moiety in Zori-003
yields Zori-004, which is subsequently esterified with Zori-005 in DMF to form Zori-006. Acidic deprotection of Zori-006 generates Zori-007, followed by methylation to deliver Zorifertinib. Concurrently, Zori-005 is prepared via amidation of Zori-008
[44] M. Roy-O’Reilly, D. Rogawski, The climb toward intracranial efficacy: Zorifertinib
in EGFR-mutant NSCLC with CNS metastases in the EVEREST trial, Med 6 (2025)
100525.
[45] Q. Zhou, Y. Yu, L. Xing, Y. Cheng, Y. Wang, Y. Pan, Y. Fan, J. Shi, G. Zhang, J. Cui,
J. Zhou, Y. Song, W. Zhuang, Z. Ma, Y. Hu, G. Li, X. Dong, J. Feng, S. Lu, J. Wu,
J. Li, L. Zhang, D. Wang, X. Xu, T.Y. Yang, N. Yang, Y. Guo, J. Zhao, Y. Yao,
D. Zhong, B. Xia, C.T. Yang, B. Zhu, P. Sun, B.Y. Shim, Y. Chen, Z. Wang, M.J. Ahn,
J. Wang, Y.L. Wu, First-line zorifertinib for EGFR-Mutant non-small cell lung
cancer with central nervous system metastases: the phase 3 EVEREST trial, Med 6
(2025) 100513.
[46] Q. Zeng, J. Wang, Z. Cheng, K. Chen, P. Johnstr¨om, K. Varn¨as, D.Y. Li, Z.F. Yang,
X. Zhang, Discovery and evaluation of clinical candidate AZD3759, a potent, oral
active, central nervous system-penetrant, epidermal growth factor receptor
tyrosine kinase inhibitor, J. Med. Chem. 58 (2015) 8200–8215.
AS ON JUNE2025 4.45 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
……
References
- Zhou Q, Yu Y, Xing L, Cheng Y, Wang Y, Pan Y, et al. (January 2025). “First-line zorifertinib for EGFR-mutant non-small cell lung cancer with central nervous system metastases: The phase 3 EVEREST trial”. Med. 6 (1) 100513. doi:10.1016/j.medj.2024.09.002. PMID 39389055.
- “Zorifertinib Receives NMPA Approval for EGFR+ NSCLC With CNS Metastases”. November 20, 2024.
| Clinical data | |
|---|---|
| Other names | AZD3759 |
| Legal status | |
| Legal status | Rx in China |
| Identifiers | |
| IUPAC name | |
| CAS Number | 1626387-80-1 |
| PubChem CID | 78209992 |
| IUPHAR/BPS | 10456 |
| DrugBank | DB14795 |
| ChemSpider | 38772332 |
| UNII | 67SX9H68W2 |
| ChEMBL | ChEMBL3623290 |
| Chemical and physical data | |
| Formula | C22H23ClFN5O3 |
| Molar mass | 459.91 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| SMILES | |
| InChI | |
//////////Zorifertinib, china 2024, APPROVALS 2024, Alpha Biopharma, ASTRA ZENECA, Zorifer, AZD 3759, 67SX9H68W2
Garsorasib
Garsorasib
Chemical Formula: C32H32F2N8O2
Exact Mass: 598.2616
Molecular Weight: 598.66
- CAS 2559761-14-5
- P491NE9G6Z
- D-1553
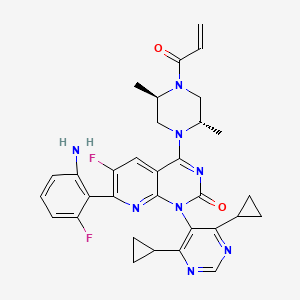
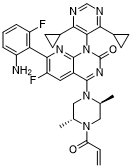
- 7-(2-amino-6-fluorophenyl)-1-(4,6-dicyclopropylpyrimidin-5-yl)-4-[(2S,5R)-2,5-dimethyl-4-prop-2-enoylpiperazin-1-yl]-6-fluoropyrido[2,3-d]pyrimidin-2-one
- 4-((2S,5R)-4-Acryloyl-2,5-dimethylpiperazin-1-yl)-7-(2-amino-6-fluorophenyl)-1-(4,6-dicyclopropylpyrimidin-5-yl)-6-fluoropyrido(2,3-d)pyrimidin-2(1H)-one
- Pyrido(2,3-d)pyrimidin-2(1H)-one, 7-(2-amino-6-fluorophenyl)-1-(4,6-dicyclopropyl-5-pyrimidinyl)-4-((2S,5R)-2,5-dimethyl-4-(1-oxo-2-propen-1-yl)-1-piperazinyl)-6-fluoro-
D 1553, Chia Tai Tianqing, CHINA 2024, APPROVALS 2024, Anfangning,
Garsorasib is an orally available inhibitor of the oncogenic KRAS substitution mutation, G12C, with potential antineoplastic activity. Upon oral administration, garsorasib selectively targets the KRAS G12C mutant and inhibits KRAS G12C mutant-dependent signaling. KRAS, a member of the RAS family of oncogenes, serves an important role in cell signaling, division and differentiation. Mutations of KRAS may induce constitutive signal transduction leading to tumor cell growth, proliferation, invasion, and metastasis.
PAT
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2021120045&_cid=P11-MEJTS8-41135-1
Example 5. Preparation and Solid state characterization of Compound 2
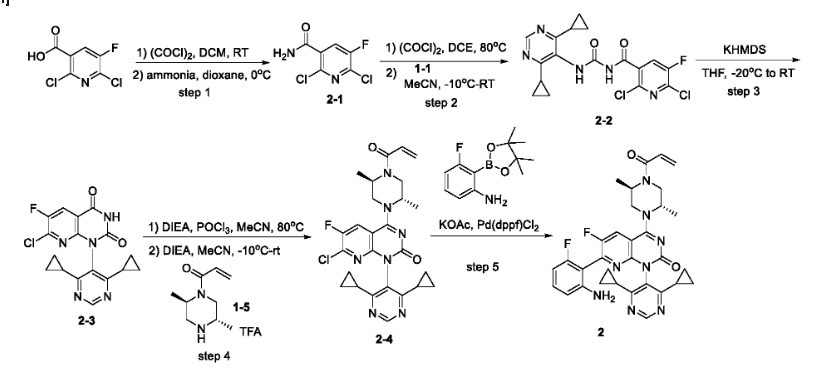
Step 1: To a mixture of 2, 6-dichloro-5-fluoronicotinic acid (23 g, 0.11 mol) in dichloromethane (300 mL) was added dimethylformamide (0.2 mL) . Oxalyl chloride (33 g, 0.26 mol) was then added slowly over 30 minutes at room temperature. The mixture was stirred at room temperature for an hour and then concentrated to give an oil which was dissolved in dioxane (50 mL) . The solution was added to ammonium hydroxide (150 mL) at 0℃ over 30 minutes. The resulting mixture was stirred at 0℃ for 30 minutes and then filtered. The filter cake was washed with cooled water (50 mL) and dried to afford 2-1.
[0183]
Step 2: A solution of 2-1 (11 g, 52.6 mmol) in 1, 2-dichloroethane (80 mL) was treated with oxalyl chloride (8.68 g, 68.4 mmol) . The mixture was stirred at 80℃ for 45 minutes and the reaction was concentrated. The residue was dissolved in acetonitrile (100 mL) , cooled to -10℃, and a solution of 1-1 (9.6 g, 55.2 mmol) in THF (30 mL) was added. The resulting mixture was stirred at room temperature for 2 hours. The solution was diluted with a sat. aqueous NaHCO 3solution and extracted with ethyl acetate. The organic layer was dried over anhydrous sodium sulfate and concentrated. The residue was purified by column chromatography on silica gel (petroleum ether to petroleum ether/ethyl acetate = 4/1) to afford 2-2.
[0184]
Step 3: To a stirred solution of 2-2 (7.9 g, 19.3 mmol) in THF (100 mL) at -20℃ was added KHMDS (38.6 mL, 1 M in THF, 38.6 mmol) . The resulting mixture was stirred at room temperature for 2 hours. The reaction was quenched with sat. aqueous NH 4Cl solution and extracted with ethyl acetate. The combined organic layers were dried over anhydrous sodium sulfate and concentrated. The residue was purified by flash column chromatography on silica gel (petroleum ether to petroleum ether/ethyl acetate = 2/1) to afford 2-3.
[0185]
Step 4: To a solution of 2-3 (746 mg, 2 mmol) and DIEA (387 mg, 3 mmol) in MeCN (20 mL) was added POCl 3(367 mg, 2.4 mmol) dropwise at room temperature. The resulting mixture was stirred at 80℃ for 45 minutes, followed by addition of DIEA (3.87 g, 30 mmol) and a solution of 1-5 (1.58 g, 4 mmol) in MeCN (10 mL) dropwise at -10℃. After stirring at room temperature for 1 hour, the reaction was quenched with ice-water and the mixture was extracted with ethyl acetate. The combined organic layers were dried over anhydrous sodium sulfate and concentrated. The residue was purified by flash column chromatography on silica gel (dichloromethane to dichloromethane/methanol = 10/1) to afford 2-4.
[0186]
Step 5: A mixture of 2-4 (8 mg, 0.15 mmol) , 3-fluoro-2- (4, 4, 5, 5-tetramethyl-1, 3, 2-dioxaborolan-2-yl) aniline (42 mg, 0.18 mmol) , Pd (dppf) Cl 2(13 mg, 0.018 mmol) and KOAc (40 mg, 0.41 mmol) in dioxane (3 mL) /H 2O (1 drop) was stirred at 80℃ for 2 hours under nitrogen atmosphere. The mixture was diluted with water and extracted with ethyl acetate. The combined organic layers were dried over anhydrous Na 2SO 4and concentrated. The residue was purified by a Prep-HPLC (acetonitrile with 0.05%of TFA in water (30%to 65%) to afford 2. LCMS (ESI, m/z) : [M+H] += 599.1; HNMR (400 MHz, methanol-d 4, ppm) : δ 8.73 (s, 1H) , 8.26-8.22 (m, 1H) , 7.15-7.09 (m, 1H) , 6.84-6.74 (m, 1H) , 6.53 (d, J = 8.4 Hz, 1H) , 6.42-6.38 (m, 1H) , 6.30-6.24 (m, 1H) , 5.83-5.78 (m, 1H) , 5.01 (brs, 1H) , 4.91-4.83 (m, 1H) , 4.53-4.29 (m, 2H) , 3.96-3.89 (m, 1.5H) , 3.54-3.50 (m, 0.5H) , 1.82-1.75 (m, 1H) , 1.73-1.66 (m, 1H) , 1.47 (d, J = 6.8 Hz, 3H) , 1.37-1.27 (m, 3H) , 1.16-1.05 (m, 4H) , 1.03-0.97 (m, 2H) , 0.88-0.83 (m, 2H) . FNMR (376 MHz, methanol-d 4, ppm) : δ -114.9 (1F) , -125.6 (1F) .
[0187]
Compound 2 prepared via the above procedure was slurried in EtOAc, and filtered to provide Compound 2 in a crystalline form A. About 1.1%of residual EtOAc was detected by 1H-NMR, corresponding to weight loss at 120 –290 ℃ in TGA (FIG. 5B) . Two overlapped endothermic peaks were observed by DSC (FIG. 5B) . Compound 2 in Form A was heated to 250 ℃ and DSC profile of the residual solid was unchanged, suggesting the overlapped peak was due to melting with crystal form transformation. Thus, the starting material was an anhydrate.
[0188]
Form A was very soluble in DCM (> 92 mg/mL) and soluble (20 –33 mg/mL) in MeOH, butanone, THF, ACN and acetone. In other solvents, Form A was practically insoluble
SYN
CN112585129
https://patentscope.wipo.int/search/en/detail.jsf?docId=CN321747237&_cid=P11-MEJTN6-36089-1
SYN
European Journal of Medicinal Chemistry 291 (2025) 117643
Garsorasib (D-1553), marketed as Anfangning, is an orally bioavailable KRAS G12C inhibitor jointly developed by InventisBio and Chia Tai Tianqing Pharmaceutical Group [40]. This compound is specifically engineered to target the KRAS G12C mutation, a prevalent oncogenic driver in multiple cancers, including NSCLC. In 2024, the NMPA granted conditional approval for Garsorasib to treat adult patients with advanced NSCLC harboring the KRAS G12C mutation, who have undergone at least one prior systemic therapy regimen [41]. Garsorasib exerts its pharmacological effects through selective and irreversible binding to the KRAS G12C mutant protein, thereby immobilizing it in an inactive GDP-bound conformation. This binding event effectively disrupts the activation of downstream signaling path
ways, including mitogen-activated protein kinase (MAPK) and phosphatidylinositol-3-kinase (PI3K), resulting in diminished tumor cell proliferation and survival. The clinical efficacy of Garsorasib has been
confirmed in a Phase II clinical trial (NCT05383898) involving patients with advanced NSCLC harboring the KRAS G12C mutation. The trial reported an ORR of 52.0 % and a DCR of 88.6 %. Additionally, the
median PFS was observed to be 9.1 months, while the median overall survival (OS) reached 14.1 months, both indicative of significant antitumor activity within this patient cohort. In terms of safety, Garsorasib
exhibited a generally favorable tolerability profile [42]. The most common treatment-related adverse events included diarrhea, nausea, and elevated liver enzymes, which were predominantly of grade 1 or 2
severity.The synthesis of Garsorasib, depicted in Scheme 10, initiates with Suzuki-Miyaura coupling of Gars-001 and cyclopropylboronic acid, affording Gars-002 [43]. Gars-003 undergoes nucleophilic acylation with acryloyl chloride to yield Gars-004. TFA-mediated Boc deprotection of Gars-004 affords Gars-005. In parallel, Gars-006 is sequentially acylated with oxalyl chloride and aminated with ammonia to form Gars-007. DCE-mediated acylation of Gars-007, followed by concentration and coupling with Gars-002 in MeCN, produces Gars-008.KHMDS-catalyzed intramolecular cyclization of Gars-008 generates Gars-009. DIEA-catalyzed intermediate generation enables nucleophilic coupling with Gars-005 to assemble Gars-010. Final Suzuki-Miyaura coupling of Gars-010 with 3-fluoro-2-(4,4,5,5-tetramethyl-1,3,2-dioxaborolan-2-yl)aniline delivers Garsorasib.
[40] W. Luo, J. Zhu, W. Zhang, A. Yu, W. Zhou, K. Xu, Efficacy and toxicity of drugs
targeting KRAS(G12C) mutation in non-small cell lung cancer: a meta-analysis,
Expert Rev. Anticancer Ther. 23 (2023) 1295–1303.
[41] Z. Li, X. Dang, D. Huang, S. Jin, W. Li, J. Shi, X. Wang, Y. Zhang, Z. Song, J. Zhang,
W. Zhuang, X. Liu, L. Jiang, X. Meng, M. Zhao, J. Zhou, L. Zhang, P. Wang, H. Luo,
J. Yang, S. Cang, X. Wang, L. Zhang, S. Lu, Garsorasib in patients with KRAS
(G12C)-mutated non-small-cell lung cancer in China: an open-label, multicentre,
single-arm, phase 2 trial, Lancet Respir. Med. 12 (2024) 589–598.
[42] Z. Li, Z. Song, Y. Zhao, P. Wang, L. Jiang, Y. Gong, J. Zhou, H. Jian, X. Dong,
W. Zhuang, S. Cang, N. Yang, J. Fang, J. Shi, J. Lu, R. Ma, P. Wu, Y. Zhang,
M. Song, C.W. Xu, Z. Shi, L. Zhang, Y. Wang, X. Wang, Y. Zhang, S. Lu, D-1553
(garsorasib), a potent and selective inhibitor of KRAS(G12C) in patients with
NSCLC: phase 1 study results, J. Thorac. Oncol. 18 (2023) 940–951.
[43] X. Dai, Y. Wang, Y. Jiang, Y. Liu, Z. Shi, Z. Wang, L. Tao, Z. Han, H. Niu, J. Weng,
Heterocyclic Compounds, Preparation Methods and Uses Thereof in the Treatment
of Cancers, 2020 CN112585129A.
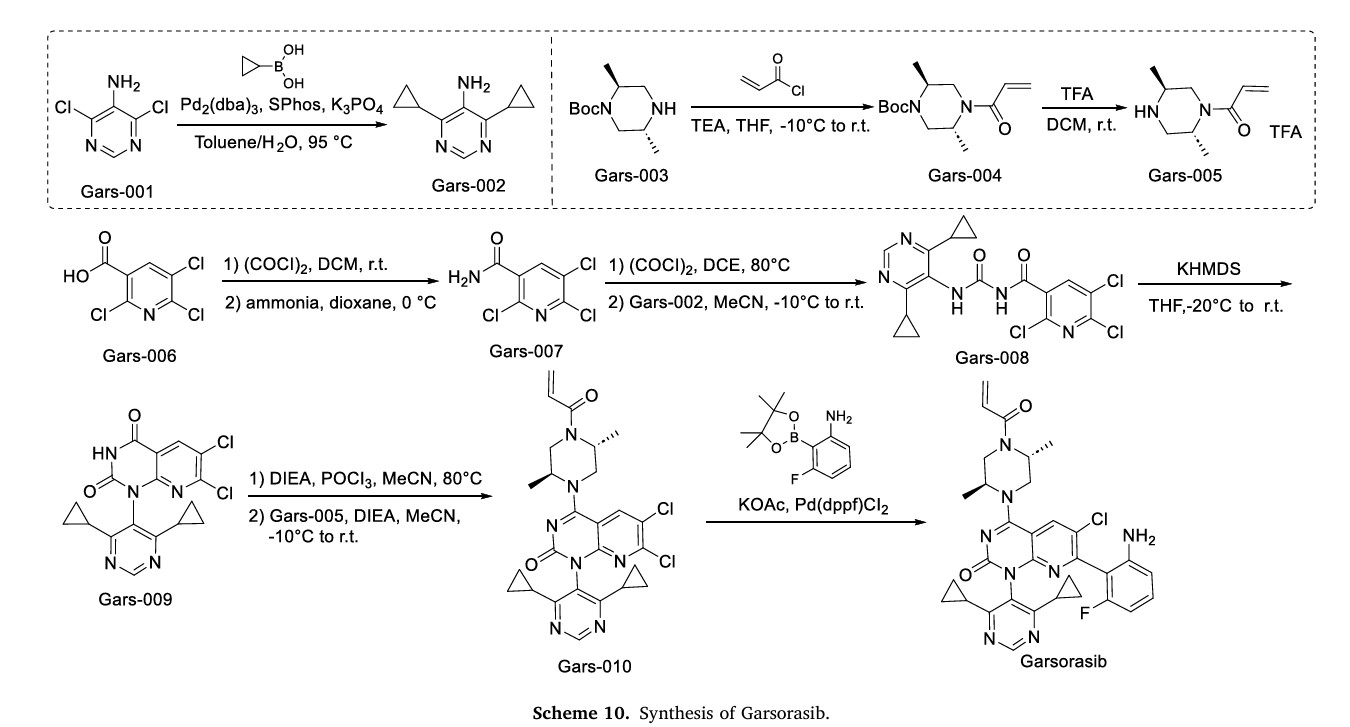
AS ON JUNE2025 4.45 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
……
- New drugs approved by the NMPA in 2024: Synthesis and clinical applicationsPublication Name: European Journal of Medicinal ChemistryPublication Date: 2025-07-05PMID: 40262297DOI: 10.1016/j.ejmech.2025.117643
- D‐1553: A novel <scp>KRASG12C</scp> inhibitor with potent and selective cellular and in vivo antitumor activityPublication Name: Cancer SciencePublication Date: 2023-05-09PMCID: PMC10323112PMID: 37158138DOI: 10.1111/cas.15829
Methods of treating a ras protein-related disease or disorder
Publication Number: US-2025049810-A1
- Heterocyclic compounds, preparation methods and uses thereofPublication Number: US-2022226328-A1Priority Date: 2019-12-18
- Heterocyclic compounds, preparation methods and uses thereofPublication Number: WO-2020233592-A1Priority Date: 2019-05-21
- Heterocyclic compounds, preparation and methods and uses thereofPublication Number: US-11091481-B2Priority Date: 2019-05-21Grant Date: 2021-08-17
- Heterocyclic compounds, preparation and methods and uses thereofPublication Number: US-2021198255-A1Priority Date: 2019-05-21
- Heterocyclic compounds, preparation methods and uses thereofPublication Number: US-2021355125-A1Priority Date: 2019-05-21
- Medicament for treatment and/or prevention of cancerPublication Number: WO-2023008462-A1Priority Date: 2021-07-27
- Heterocyclic compounds, preparation methods and uses thereofPublication Number: US-2021260067-A1Priority Date: 2019-12-18
- Heterocyclic compounds, preparation methods and uses thereofPublication Number: WO-2021120045-A1Priority Date: 2019-12-18
- Heterocyclic compounds, preparation methods and uses thereofPublication Number: WO-2021121330-A1Priority Date: 2019-12-18
- Heterocyclic compounds, preparation methods and uses thereofPublication Number: US-11241437-B2Priority Date: 2019-12-18Grant Date: 2022-02-08
- Medicament for treatment and/or prevention of cancerPublication Number: AU-2022320304-A1Priority Date: 2021-07-27
- Medicament for treatment and/or prevention of cancerPublication Number: CA-3227706-A1Priority Date: 2021-07-27
- Medicines for the treatment and/or prevention of cancerPublication Number: CN-117677398-APriority Date: 2021-07-27
- Medicament for treatment and/or prevention of cancerPublication Number: EP-4378478-A1Priority Date: 2021-07-27
- Medicines for the treatment and/or prevention of cancerPublication Number: KR-20240041917-APriority Date: 2021-07-27
- Composition for preventing or treating c-myc-associated diseases through inhibition of expression of ubiquitin-specific protease 47 (usp47), and use thereofPublication Number: WO-2024085603-A1Priority Date: 2022-10-18
- Chimeric small molecules for labeling proteins with immunogenic moieties and methods of use thereofPublication Number: WO-2024081675-A2Priority Date: 2022-10-10
- Macrocyclic heterocycles and uses thereofPublication Number: US-11912708-B2Priority Date: 2022-04-20Grant Date: 2024-02-27
- Macrocyclic heterocycles and uses thereofPublication Number: US-2023339952-A1Priority Date: 2022-04-20
- Macrocyclic heterocycles and uses thereofPublication Number: WO-2023205701-A1Priority Date: 2022-04-20
- Composition for cancer prevention or treatment containing met inhibitor and k-ras inhibitorPublication Number: WO-2024191132-A1Priority Date: 2023-03-10
- Combination therapy and related methodsPublication Number: TW-202436340-APriority Date: 2023-02-06
- Combination therapy and related methodsPublication Number: US-2024343813-A1Priority Date: 2023-02-06
- Combination therapy and related methodsPublication Number: WO-2024167880-A1Priority Date: 2023-02-06
- A composition for preventing or treating c-Myc-related diseases through suppression of expression of USP47, and use thereofPublication Number: KR-20240055632-APriority Date: 2022-10-18
- Ectonucleotide pyrophosphatase/phosphodiesterase 1 (enpp1) inhibitor combinations and uses thereofPublication Number: WO-2025007955-A1Priority Date: 2023-07-06
- Methionine adenosyltransferase 2a (mat2a) inhibitor combinations and uses thereofPublication Number: WO-2024217502-A1Priority Date: 2023-04-19
- Combinations of kras inhibitor and atr inhibitor for the treatment of cancerPublication Number: WO-2024213699-A1Priority Date: 2023-04-14
- Anti-lipocalin-2 antibodies and uses thereofPublication Number: WO-2024191972-A2Priority Date: 2023-03-13
- Composition for Cancer Prevention or Treatment Including MET inhibitors and K-RAS inhibitorsPublication Number: KR-20240138493-APriority Date: 2023-03-10
- A kind of preparation method of 2,5,6-trichloronicotinic acidPublication Number: CN-117263854-APriority Date: 2023-09-15
- Protein tyrosine phosphatase degraders and uses thereofPublication Number: WO-2025030006-A2Priority Date: 2023-08-02
- Protein tyrosine phosphatase inhibitor combinationsPublication Number: WO-2025030008-A1Priority Date: 2023-08-02
- Methods of treating a ras related disease or disorderPublication Number: US-2025041295-A1Priority Date: 2023-07-14
- Methods of treating a ras related disease or disorderPublication Number: WO-2025019318-A2Priority Date: 2023-07-14
///////Garsorasib, D 1553, Chia Tai Tianqing, CHINA 2024, APPROVALS 2024, Anfangning, 2559761-14-5, P491NE9G6Z
Fulzerasib
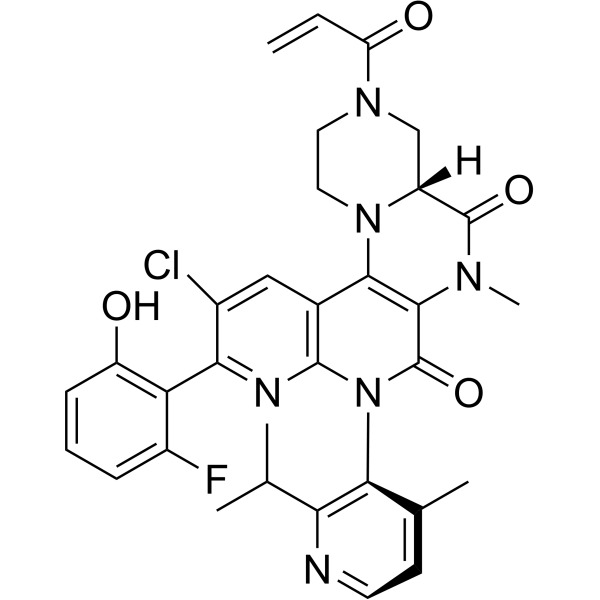
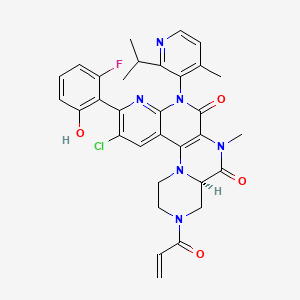
Fulzerasib
GFH925
CAS No. : 2641747-54-6
| Molecular Weight | 617.07 |
|---|---|
| Formula | C32H30ClFN6O4 |
(7R)-16-chloro-15-(2-fluoro-6-hydroxyphenyl)-9-methyl-12-(4-methyl-2-propan-2-ylpyridin-3-yl)-5-prop-2-enoyl-2,5,9,12,14-pentazatetracyclo[8.8.0.02,7.013,18]octadeca-1(10),13,15,17-tetraene-8,11-dione
CHINA 2024, APPROVALS 2024, Innovent Biologics, DUPERT
Fulzerasib (Dupert®; Innovent Biologics/GenFleet Therapeutics) is an orally active small molecule inhibitor of the KRAS G12C mutant protein being developed for the treatment of solid tumors harboring the KRAS G12C oncogenic driver mutation, including non-small cell lung cancer (NSCLC) and colorectal cancer. Fulzerasib received its first approval on 21 August 2024 in China, for the treatment of adults with KRAS G12C-mutated advanced NSCLC who have received at least one line of systemic therapy. This conditional approval was based on the positive results of a single-arm, phase II study. This article summarizes the milestones in the development of fulzerasib leading to this first approval for KRAS G12C-mutated advanced NSCLC.
Fulzerasib (GFH925) is an irreversible KRAS G12C inhibitor, has a synergistic anti-cancer effect with cetuximab (HY-P9905)..
PAPER
https://pubs.acs.org/doi/10.1021/acs.jmedchem.4c03183
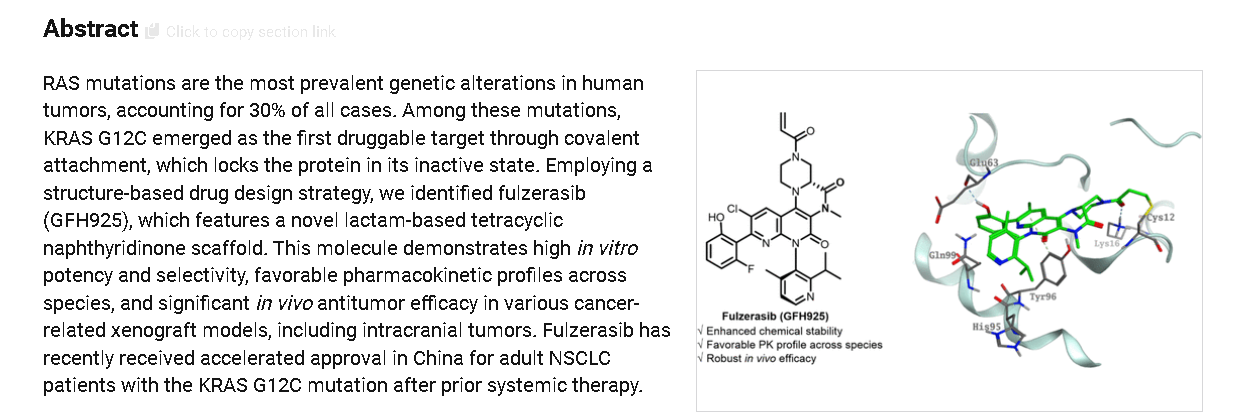
PAT
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2021083167&_cid=P20-MEJIF1-91906-1
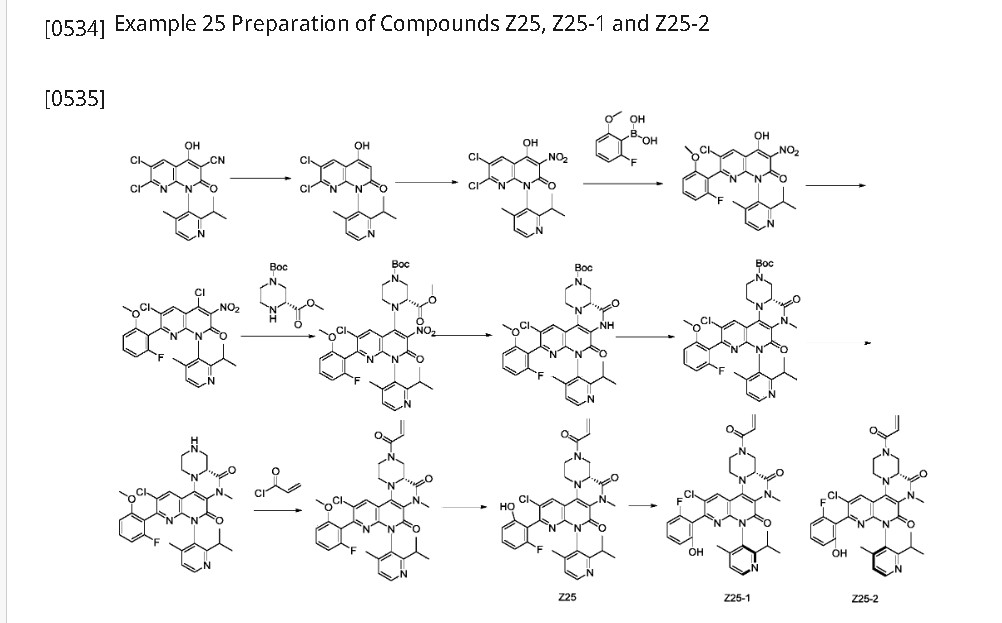
Step 1: Suspend 6,7-dichloro-4-hydroxy-1-(2-isopropyl-4-methylpyridin-3-yl)-2-oxo-1,2-dihydro-1,8-naphthyridine-3-carbonitrile (30.0 g, 77.319 mmol) in a mixture of 1,4-dioxane (120 mL) and water (120 mL). Slowly add concentrated sulfuric acid (120 mL). Stir at 120°C for 36 hours. Pour the cooled reaction mixture into 200 mL of ice water, adjust the pH to 2-3 with sodium carbonate, and extract with ethyl acetate (1000 mL x 2). Combine the ethyl acetate phases, dry over anhydrous sodium sulfate, filter, and vacuum-dry the filtrate to obtain 6,7-dichloro-4-hydroxy-1-(2-isopropyl-4-methylpyridin-3-yl)-1,8-naphthyridine-2(1H)-one (24 g, Y: 85.7%) as a light brown solid. ES-API: [M+H]
[0537]Step 2: 6,7-Dichloro-4-hydroxy-1-(2-isopropyl-4-methylpyridin-3-yl)-1,8-naphthyridin-2(1H)-one (3.16 g, 8.705 mmol) was dissolved in acetic acid (15 mL). Sodium nitrite (100 mg, 1.58 mmol) and concentrated nitric acid (5.0 mL, 74.52 mmol) were added sequentially. The reaction was stirred at room temperature for 30 minutes. The reaction solution was slowly poured into 100 mL of ice water. The precipitated solid was filtered, and the filter cake was washed with 20 mL of ice water and dried under vacuum to obtain 6,7-dichloro-4-hydroxy-1-(2-isopropyl-4-methylpyridin-3-yl)-3-nitro-1,8-naphthyridin-2(1H)-one (3.5 g, Y: 92%) as a yellow solid. ES-API: [M+H]
[0538]Step 3: To a 100 mL three-necked round-bottom flask, add 6,7-dichloro-4-hydroxy-1-(2-isopropyl-4-methylpyridin-3-yl)-3-nitro-1,8-naphthyridin-2(1H)-one (3.5 g, 8.570 mmol), (2-fluoro-6-methoxyphenyl)boronic acid (5.8 g, 34.10 mmol), tetrakistriphenylphosphine palladium (1.15 g, 0.9956 mmol), sodium carbonate (3.5 g, 33.02 mmol), 10 mL of water, and 40 mL of dioxane. Under nitrogen, stir at 100°C for 2-3 hours. After completion, cool the reaction mixture to room temperature, add 80 mL of water and 100 mL of methyl tert-butyl ether, and extract once. The aqueous phase was adjusted to pH 3-5 with 1M hydrochloric acid solution and extracted with ethyl acetate (200 mL x 2). The ethyl acetate phases were combined, dried over anhydrous sodium sulfate, filtered, and the filtrate was dried under vacuum to afford 6-chloro-7-(2-fluoro-6-methoxyphenyl)-4-hydroxy-1-(2-isopropyl-4-methylpyridin-3-yl)-3-nitro-1,8-naphthyridin-2(1H)-one (4.5 g, crude) as a pale yellow solid. ES-API: [M+H]
[0539]Step 4: 6-Chloro-7-(2-fluoro-6-methoxyphenyl)-4-hydroxy-1-(2-isopropyl-4-methylpyridin-3-yl)-3-nitro-1,8-naphthyridin-2(1H)-one (4.6 g, 8.57 mmol) was dissolved in acetonitrile (30 mL). Phosphorus oxychloride (7.5 g, 48.92 mmol) and N,N-diisopropylethylamine (10.5 g, 81.24 mmol) were added sequentially. The reaction mixture was gradually heated to 80°C and stirred for 30 minutes. The reaction solution was concentrated, 30 mL of cold acetonitrile was added, and the mixture was added dropwise to 150 mL of saturated sodium bicarbonate solution under an ice-water bath. The mixture was extracted with ethyl acetate (200 mL x 2). The ethyl acetate phases were combined and washed once with 200 mL of saturated brine. The reaction mixture was dried over anhydrous sodium sulfate and filtered. The organic phase was dried and concentrated, and the crude product was purified by flash silica gel column chromatography (EtOAc/PE: 0-50%) to afford 4,6-dichloro-7-(2-fluoro-6-methoxyphenyl)-1-(2-isopropyl-4-methylpyridin-3-yl)-3-nitro-1,8-naphthyridin-2(1H)-one (3.05 g, Y: 76%) as a yellow solid. ES-API: [M+H]
[0540]Step 5: 4,6-Dichloro-7-(2-fluoro-6-methoxyphenyl)-1-(2-isopropyl-4-methylpyridin-3-yl)-3-nitro-1,8-naphthyridin-2(1H)-one (2.5 g, 4.843 mmol) was dissolved in N,N-dimethylacetamide (25 mL). 1-(tert-butyl)-3-methyl(R)-piperazine-1,3-dicarboxylate (3.5 g, 14.34 mmol) and N,N-diisopropylethylamine (2.0 g, 15.47 mmol) were added sequentially. The reaction mixture was stirred at 120°C for 2 hours. 80 mL of ethyl acetate was added to the reaction mixture, and the mixture was washed three times with 80 mL of saturated brine. The ethyl acetate phase was dried and concentrated, and the crude product was purified on a flash silica gel column (EtOAc/PE: 0-80%) to afford 1-(tert-butyl)-3-methyl (3R)-4-(6-chloro-7-(2-fluoro-6-methoxyphenyl)-1-(2-isopropyl-4-methylpyridin-3-yl)-3-nitro-2-oxo-1,2-dihydro-1,8-naphthyridin-4-yl)piperazine-1,3-dicarboxylate (2.7 g, Y: 77%) as a yellow solid. ES-API: [M+H]
[0541]Step 6: 1-(tert-Butyl)3-methyl(3R)-4-(6-chloro-7-(2-fluoro-6-methoxyphenyl)-1-(2-isopropyl-4-methylpyridin-3-yl)-3-nitro-2-oxo-1,2-dihydro-1,8-naphthyridin-4-yl)piperazine-1,3-dicarboxylate (2.7 g, 3.728 mmol) was dissolved in acetic acid (30 mL), iron powder (835 mg, 14.91 mmol) was added, and the reaction was stirred at 80 °C for 30 minutes. The reaction mixture was concentrated, and 200 mL of ethyl acetate and 100 mL of saturated sodium bicarbonate were added sequentially. The suspension was filtered through celite, and the filter cake was washed with ethyl acetate. The organic phase was separated and washed sequentially with 100 mL of saturated sodium bicarbonate and 150 mL of saturated brine. The mixture was dried and concentrated to give (4aR)-11-chloro-10-(2-fluoro-6-methoxyphenyl)-8-(2-isopropyl-4-methylpyridin-3-yl)-5,7-dioxo-1,2,4,4a,5,6,7,8-octahydro-3H-pyrazino[1′,2′:4,5]pyrazino[2,3-c][1,8]naphthyridine-3-carboxylic acid tert-butyl ester (2.70 g, crude) as a yellow solid. ES-API: [M+H]+ = 663.2.
[0542]Step 7: To a 150 mL sealed tube was added tert-butyl (4aR)-11-chloro-10-(2-fluoro-6-methoxyphenyl)-8-(2-isopropyl-4-methylpyridin-3-yl)-5,7-dioxo-1,2,4,4a,5,6,7,8-octahydro-3H-pyrazino[1′,2′:4,5]pyrazino[2,3-c][1,8]naphthyridine-3-carboxylate (2.7 g, 3.728 mmol), 30 mL of acetone, anhydrous potassium carbonate (2.2 g, 15.94 mmol), and iodomethane (5.4 g, 38.03 mmol). The tube was sealed and the reaction was stirred at 55°C for 18 hours. The reaction mixture was added with 150 mL of ethyl acetate, washed three times with 100 mL of saturated brine, dried, and concentrated. The crude product was purified on a flash silica gel column (EtOAc/PE: 0-80%) to obtain (4aR)-11-chloro-10-(2-fluoro-6-methoxyphenyl)-8-(2-isopropyl-4-methylpyridin-3-yl)-6-methyl-5,7-dioxo-1,2,4,4a,5,6,7,8-octahydro-3H-pyrazino[1′,2′:4,5]pyrazino[2,3-c][1,8]naphthyridine-3-carboxylic acid tert-butyl ester (2.2 g, Y: 87%) as a yellow solid. ES-API: [M+H]
[0543]Step 8: Tert-butyl (4aR)-11-chloro-10-(2-fluoro-6-methoxyphenyl)-8-(2-isopropyl-4-methylpyridin-3-yl)-6-methyl-5,7-dioxo-1,2,4,4a,5,6,7,8-octahydro-3H-pyrazino[1′,2′:4,5]pyrazino[2,3-c][1,8]naphthyridine-3-carboxylate (517 mg, 0.7549 mmol) was dissolved in dichloromethane (8 mL) and trifluoroacetic acid (2 mL) was added. After stirring at room temperature for 2 hours, the reaction mixture was concentrated to afford (4aR)-11-chloro-10-(2-fluoro-6-methoxyphenyl)-8-(2-isopropyl-4-methylpyridin-3-yl)-6-methyl-2,3,4,4a,6,8-hexahydro-1H-pyrazino[1′,2′:4,5]pyrazino[2,3-c][1,8]naphthyridine-5,7-dione (530 mg, crude), which was used directly in the next reaction. ES-API: [M+H]
[0544]Step 9: (4aR)-11-chloro-10-(2-fluoro-6-methoxyphenyl)-8-(2-isopropyl-4-methylpyridin-3-yl)-6-methyl-2,3,4,4a,6,8-hexahydro-1H-pyrazino[1′,2′:4,5]pyrazino[2,3-c][1,8]naphthyridine-5,7-dione (530 mg, 0.7549 mmol) was dissolved in dichloromethane (15 mL) and triethylamine (3.0 mL, 21.62 mmol) was added. The reaction mixture was cooled to 0°C and acryloyl chloride (100 mg, 1.1048 mmol) was added dropwise. The reaction was stirred at 0°C for 15 minutes. 80 mL of dichloromethane was added to the reaction solution, and the mixture was washed with 100 mL of saturated aqueous NaHCO₃
and 80 mL of saturated brine, dried, and concentrated. The crude product was purified on a flash silica gel column (EtOAc/PE: 0-60%) to obtain (4aR)-3-acryloyl-11-chloro-10-(2-fluoro-6-methoxyphenyl)-8-(2-isopropyl-4-methylpyridin-3-yl)-6-methyl-2,3,4,4a,6,8-hexahydro-1H-pyrazino[1′,2′:4,5]pyrazino[2,3-c][1,8]naphthyridine-5,7-dione (280 mg, Y: 59%) as a yellow solid. ES-API: [M+H]
[0545]Step 10: In an ice-water bath, (4aR)-3-acryloyl-11-chloro-10-(2-fluoro-6-methoxyphenyl)-8-(2-isopropyl-4-methylpyridin-3-yl)-6-methyl-2,3,4,4a,6,8-hexahydro-1H-pyrazino[1′,2′:4,5]pyrazino[2,3-c][1,8]naphthyridine-5,7-dione (280 mg, 0.444 mmol) was added to dry dichloromethane (6.0 mL), and then boron tribromide (5.0 mL, 5.0 mmol) was added. The mixture was warmed to room temperature and reacted overnight. Under ice-water bath conditions, the reaction solution was added dropwise to a saturated sodium bicarbonate solution, extracted twice with dichloromethane (80 mL), dried, and concentrated. The crude product was purified by flash silica gel column chromatography (EtOAc/PE: 0-60%) to give (4aR)-3-acryloyl-11-chloro-10-(2-fluoro-6-hydroxyphenyl)-8-(2-isopropyl-4-methylpyridin-3-yl)-6-methyl-2,3,4,4a,6,8-hexahydro-1H-pyrazino[1′,2′:4,5]pyrazino[2,3-c][1,8]naphthyridine-5,7-dione (Z25, 233 mg, Y: 85%).
[0546]Step 11: Compound Z25 was separated by preparative chiral HPLC (column type: IA: 10 μm, 30*250 mm, mobile phase: hexane:EtOH = 60:40, flow rate: 25 ml/min, column temperature) to obtain: an atropisomer compound Z25-1 (76.8 mg, peak 1, retention time 2.531 min, Y: 34%).
1 H NMR (500 MHz, DMSO-d
6 )δ10.03(d,J=18.4Hz,1H),8.52(d,J=7.3Hz,1H),8.43(d,J=4.7Hz,1H),7.23(d,J=9.6Hz,2H),7.08(dd,J=16 .6,10.5Hz,1H),6.74–6.62(m,2H),6.15(d,J=16.8Hz,1H),5.75(d,J=10.7Hz,1H),4.73(d,J=14.2Hz,1H),4.4 6 (d, J = 12.9 Hz, 1H), 4.00 (s, 1H), 3.61 (d, J = 10.0 Hz, 1H), 3.51 (s, 1H), 3.34 (s, 3H), 3.22 (s, 1H), 2.64 (t, J = 11.5 Hz, 1H), 2.48–2.42 (m, 1H), 1.98 (d, J = 5.1 Hz, 3H), 1.03 (t, J = 6.9 Hz, 3H), 0.86 (t, J = 7.9 Hz, 3H). ES-API: [M+H]
+ = 617.2. And another atropisomer compound Z25-2 (70 mg, peak 2, retention time 3.683 min, Y: 31%).
1 H NMR (500MHz, CDCl
3 )δ8.64–8.59(m,1H),8.35(s,1H),8.07(s,1H),7.27–7.20(m,2H),7.14–7.02(m,1H),6.75–6.63(m,2H),6.39(dd,J=17.0,2.0Hz,1H),5.88 –5.77(m,1H),4.91(d,J=14.0Hz,1H),4.83(d,J=13.0Hz,1H),3.72–3.58(m,2H),3.50(s,3H),3.43(d,J=12.0Hz,1H),3.1 6(t,J=13.0Hz,1H),2.91(t,J=12.0Hz,1H),2.82-2.73(m,1H),1.93(s,3H),1.24(d,J=7.0Hz,3H),1.12(d,J=7.0Hz,3H). ES-API: [M+H]
+ =617.2. The isomers were detected by analytical chiral HPLC (column type: IA: 5 μm, 4.6*150 mm, mobile phase: hexane:EtOH=60:40, flow rate: 1 ml/min, column temperature=30°C).
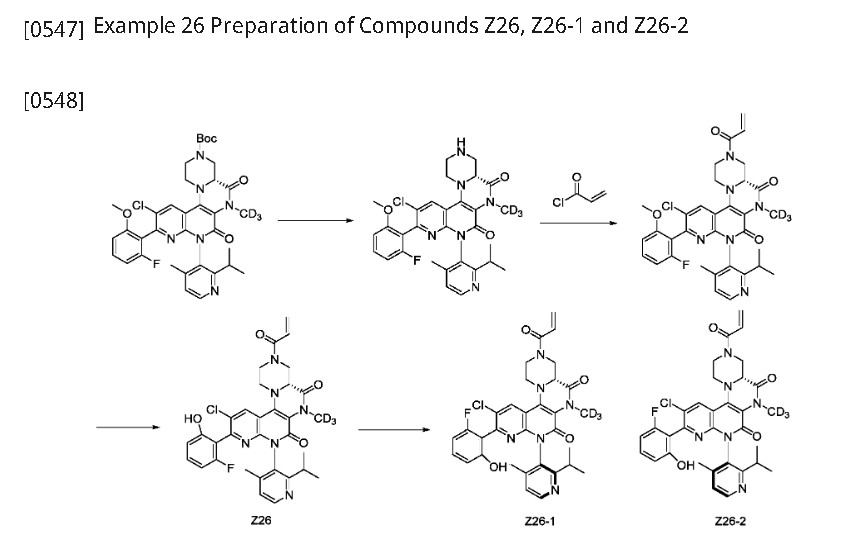
Step 1: (4aR)-11-chloro-10-(2-fluoro-6-methoxyphenyl)-8-(2-isopropyl-4-methylpyridin-3-yl)-6-(methyl-d3)-5,7-dioxo-1,2,4,4a,5,6,7,8-octahydro-3H-pyrazino[1′,2′:4,5]pyrazino[2,3-c][1,8]naphthyridine-3-carboxylic acid tert-butyl ester (511 mg, 0.7549 mmol) was dissolved in dichloromethane (8 mL) and trifluoroacetic acid (2 mL) was added. After stirring at room temperature for 2 hours, the reaction mixture was concentrated to give (4aR)-11-chloro-10-(2-fluoro-6-methoxyphenyl)-8-(2-isopropyl-4-methylpyridin-3-yl)-6-(methyl-d3)-2,3,4,4a,6,8-hexahydro-1H-pyrazino[1′,2′:4,5]pyrazino[2,3-c][1,8]naphthyridine-5,7-dione (520 mg, crude), which was used directly in the next reaction. ES-API: [M+H]
[0550]Step 2: (4aR)-11-chloro-10-(2-fluoro-6-methoxyphenyl)-8-(2-isopropyl-4-methylpyridin-3-yl)-6-(methyl-d3)-2,3,4,4a,6,8-hexahydro-1H-pyrazino[1′,2′:4,5]pyrazino[2,3-c][1,8]naphthyridine-5,7-dione (520 mg, 0.7549 mmol) was dissolved in dichloromethane (10 mL) and triethylamine (3.0 mL, 21.62 mmol) was added. The reaction mixture was cooled to 0°C and acryloyl chloride (100 mg, 1.1048 mmol) was added dropwise. The reaction was stirred at 0°C for 15 minutes. 80 mL of dichloromethane was added to the reaction solution, and the mixture was washed with 100 mL of saturated aqueous NaHCO₃
and 80 mL of saturated brine, dried, and concentrated. The crude product was purified on a flash silica gel column (EtOAc/PE: 0-60%) to obtain (4aR)-3-acryloyl-11-chloro-10-(2-fluoro-6-methoxyphenyl)-8-(2-isopropyl-4-methylpyridin-3-yl)-6-(methyl-d₃)-2,3,4,4a,6,8-hexahydro-1H-pyrazino[1′,2′:4,5]pyrazino[2,3-c][1,8]naphthyridine-5,7-dione (232 mg, Y: 48%) as a yellow solid. ES-API: [M+H]
[0551]Step 3: Under ice-water bath conditions, (4aR)-3-acryloyl-11-chloro-10-(2-fluoro-6-methoxyphenyl)-8-(2-isopropyl-4-methylpyridin-3-yl)-6-(methyl-d3)-2,3,4,4a,6,8-hexahydro-1H-pyrazino[1′,2′:4,5]pyrazino[2,3-c][1,8]naphthyridine-5,7-dione (240 mg, 0.3791 mmol) was added to dry dichloromethane (6.0 mL), and boron tribromide (5.0 mL, 5.0 mmol) was added. The temperature was warmed to room temperature and the reaction was allowed to react overnight. Under ice-water bath conditions, the reaction solution was added dropwise to a saturated sodium bicarbonate solution, extracted twice with dichloromethane (80 mL), dried, and concentrated. The crude product was purified on a flash silica gel column (EtOAc/PE: 0-60%) to give (4aR)-3-acryloyl-11-chloro-10-(2-fluoro-6-hydroxyphenyl)-8-(2-isopropyl-4-methylpyridin-3-yl)-6-(methyl-d3)-2,3,4,4a,6,8-hexahydro-1H-pyrazino[1′,2′:4,5]pyrazino[2,3-c][1,8]naphthyridine-5,7-dione (Z26, 187 mg, Y: 79%). [M+H]
[0552]Step 4: Compound Z26 (187 mg, 0.302 mmol) was separated by preparative chiral HPLC (column type: IA: 10 μm, 30*250 mm, mobile phase: hexane:EtOH = 60:40, flow rate: 25 ml/min, column temperature) to obtain: an atropisomer compound, arbitrarily designated as Z26-1 (68.8 mg, peak 1, retention time 2.525 min, Y: 36.7%).
1 H NMR (500 MHz, DMSO-d
6 )δ10.03(d,J=17.9Hz,1H),8.51(d,J=7.4Hz,1H),8.43(d,J=4.7Hz,1H),7.29–7.18(m,2H),7.08(dd,J =17.0,10.6Hz,1H),6.74–6.61(m,2H),6.15(d,J=16.6Hz,1H),5.75(d,J=11.5Hz,1H),4.73(d,J=13.5 Hz, 1H), 4.46 (d, J = 12.3 Hz, 1H), 4.00 (s, 1H), 3.61 (d, J = 10.5 Hz, 1H), 3.50 (s, 1H), 3.22 (s, 1H), 2.65 (t, J = 12.5 Hz, 1H), 2.49–2.42 (m, 1H), 1.98 (d, J = 5.0 Hz, 3H), 1.02 (d, J = 7.0 Hz, 3H), 0.86 (t, J = 7.9 Hz, 3H). ES-API: [M+H]
+ = 620.3. Another atropisomer, arbitrarily designated Z26-2 (63.2 mg, peak 2, retention time 3.683 min, Y: 33.79%), was obtained.
1 H NMR (400 MHz, CDCl
3 )δ8.62(d,J=4.8Hz,1H),8.35(s,1H),8.07(s,1H),7.24–7.20(m,2H),7.16–7.01(m,1H),6.74–6.6 3(m,2H),6.39(dd,J=16.8,2.0Hz,1H),5.82(dd,J=10.4,2.0Hz,1H),4.91(d,J=13.6Hz,1H),4.83(d δ (d, J = 13.6 Hz, 1H), 3.71–3.57 (m, 2H), 3.42 (d, J = 12.0 Hz, 1H), 3.16 (t, J = 12.8 Hz, 1H), 2.91 (t, J = 12.0 Hz, 1H), 2.81–2.70 (m, 1H), 1.92 (s, 3H), 1.22 (d, J = 6.8 Hz, 3H), 1.10 (d, J = 6.8 Hz, 3H). ES-API: [M+H]
+ = 620.3. The isomeric compounds were detected by analytical chiral HPLC (column type: IA: 5 μm, 4.6*150 mm, mobile phase: hexane:EtOH = 60:40, flow rate: 1 ml/min, column temperature = 30°C).
PAT
- US12054497, Compound Z25-1
- US12054497, Compound Z25-2
- US12054497, Compound Z26-1
- US12054497, Compound Z26-2
PAT
CN112390818
https://patentscope.wipo.int/search/en/detail.jsf?docId=CN319676055&_cid=P20-MEJIKL-96783-1
| Example 25 Preparation of Z25 |
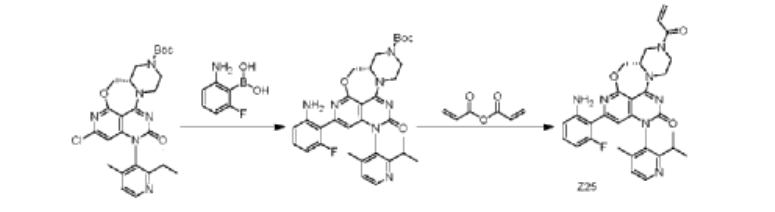
| Step 1: To a 100 mL three-necked round-bottom flask was added (S)-2-chloro-12-(2-isopropyl-4-methylpyridin-3-yl)-11-oxo-5a,6,8,9,11,12-hexahydro-4-oxo-3,7,9a,10,12-pentaazabenzo[4,5]cycloheptyl[1,2,3-de]naphthalene-7(5H)-carboxylic acid tert-butyl ester (1.4 g, 2.66 mmol), (2-amino-6-fluorophenyl)boronic acid (0.6 g, 3.87 mmol), Sphos-Pd-G2 (0.2 g, 0.21 mmol), Sphos (120 mg, 0.29 mmol), potassium phosphate (1.2 g, 5.66 mmol), 10 mL of dioxane, and 2 mL of water. The system was purged with nitrogen three times and then protected with nitrogen. The reaction was continued at 120°C for 2 h. 30 mL of ethyl acetate was added to the reaction solution, which was washed three times with 30 mL of saturated brine, dried, and concentrated. The crude product was purified on a flash silica gel column to give the target product, (S)-2-(2-amino-6-fluorophenyl)-12-(2-isopropyl-4-methylpyridin-3-yl)-11-oxo-5a,6,8,9,11,12-hexahydro-4-oxa-3,7,9a,10,12-pentaazabenzo[4,5]cyclohepta[1,2,3-de]naphthalene-7(5H)-carboxylic acid tert-butyl ester (845 mg, yield: 41%). ES-API: [M+H]+ = 602.2. |
| Step 2: Dissolve (S)-tert-butyl 2-(2-amino-6-fluorophenyl)-12-(2-isopropyl-4-methylpyridin-3-yl)-11-oxo-5a,6,8,9,11,12-hexahydro-4-oxa-3,7,9a,10,12-pentaazabenzo[4,5]cyclohepta[1,2,3-de]naphthalene 7(5H)-carboxylate (800 mg, 1.33 mmol) in dichloromethane (8 mL), and add trifluoroacetic acid (2 mL). Stir at room temperature for 2 hours. The reaction mixture is concentrated to obtain the target intermediate, which is dissolved in dichloromethane (15 mL) and triethylamine (800 mg, 87.1 mmol) is added. Cool the reaction mixture to 0°C, and add acrylic anhydride (160 mg, 1.27 mmol) dropwise. Stir the reaction mixture at 0°C for 15 minutes. The reaction mixture was added with 40 mL of dichloromethane, washed with 50 mL of saturated aqueous NaHCO₃ and 40 mL of saturated brine, dried, and concentrated. The crude product was purified on a flash silica gel column to obtain the target product, Z25(S)-7-acryloyl-2-(2-amino-6-fluorophenyl)-12-(2-isopropyl-4-methylpyridin-3-yl)-5,5a,6,7,8,9-hexahydro-4-oxa-3,7,9a,10,12-pentaazabenzo[4,5]cyclohepta[1,2,3-de]naphthalen-11(12H)-one (250 mg, yield: 34%). ES-API: [M+H] ⁺ = 556.2. 1 H NMR (500MHz, DMSO) δ8.55 (d, J=4.9Hz, 1H), 7.32 (d, J=4.9Hz, 1H), 7.04 (dd, J= 14.8,8.0Hz,1H),6.95-6.80(m,1H),6.52(d,J=8.3Hz,1H),6.36-6.13(m,4H) ,6.06-5.95(m,1H),5.78(d,J=10.3Hz,1H),4.82-4.04(m,7H),3.56(s,1H),3 .25-3.18(m,1H),2.84-2.70(m,1H),1.98(d,J=5.2Hz,3H),1.15-0.95(m,6H). |
| Example 26 Preparation of Z26 |

| Step 1: To a solution of 7-chloro-1-(2-isopropyl-4-methylpyridin-3-yl)pyrido[4,3-d]pyrimidine-2,4(1H,3H)-dione (130 mg, 0.39 mmol) in acetonitrile (3 mL) were added phosphorus oxychloride (1 mL) and N,N-diisopropylethylamine (1 mL) sequentially. The mixture was stirred at 90°C for 2 h. The reaction mixture was concentrated to afford crude 4,7-dichloro-1-(2-isopropyl-4-methylpyridin-3-yl)pyrido[4,3-d]pyrimidin-2(1H)-one (130 mg). ES-API: [M+H] + = 349.3. |
| Step 2: To a solution of 4,7-dichloro-1-(2-isopropyl-4-methylpyridin-3-yl)pyrido[4,3-d]pyrimidin-2(1H)-one (130 mg, 0.37 mmol) in acetonitrile (3 mL) was added N,N-diisopropylethylamine (144 mg, 1.12 mmol) and tert-butyl piperazine-1-carboxylate (70 mg, 0.37 mmol) under ice-cooling. The mixture was stirred for 30 minutes. The reaction mixture was poured into 20 mL of water and extracted with ethyl acetate (20 mL x 3). The mixture was dried over anhydrous sodium sulfate and concentrated. The mixture was then purified on a flash silica gel column (0-100% ethyl acetate/petroleum ether) to obtain tert-butyl 4-(7-chloro-1-(2-isopropyl-4-methylpyridin-3-yl)-2-oxo-1,2-dihydropyrido[4,3-d]pyrimidin-4-yl)piperazine-1-carboxylate (140 mg) as a white solid. ES-API: [M+H] + = 499.1. |
| Step 3: Under nitrogen protection, a mixture of tert-butyl 4-(7-chloro-1-(2-isopropyl-4-methylpyridin-3-yl)-2-oxo-1,2-dihydropyrido[4,3-d]pyrimidin-4-yl)piperazine-1-carboxylate (140 mg, 0.28 mmol), 2-fluoro-6-hydroxyphenylboronic acid (44 mg, 0.42 mmol), chloro(2-dicyclohexylphosphino-2′,6′-dimethoxy-1,1′-biphenyl)(2′-amino-1,1′-biphenyl-2-yl)palladium(II) (13 mg, 0.02 mmol), 2-dicyclohexylphosphino-2′,6′-dimethoxybiphenyl (10 mg, 0.02 mmol) and potassium phosphate (120 mg, 0.84 mmol) in 1,4-dioxane (4 mL) and water (1 mL) was microwaved at 120 ° C for 1 h. The reaction mixture was filtered and washed with ethyl acetate (100 mL). The filtrate was washed with saturated brine (50 mL x 3). The resulting organic phase was dried, concentrated, and purified on a flash silica gel column (0-100% ethyl acetate/petroleum ether) to afford tert-butyl 4-(7-(2-fluoro-6-hydroxyphenyl)-1-(2-isopropyl-4-methylpyridin-3-yl)-2-oxo-1,2-dihydropyridinyl[4,3-d]pyrimidin-4-yl)piperazine-1-carboxylate (100 mg, yield: 62%) as a white solid. ES-API: [M+H] + = 575.2. |
| Step 4: To a solution of tert-butyl 4-(7-(2-fluoro-6-hydroxyphenyl)-1-(2-isopropyl-4-methylpyridin-3-yl)-2-oxo-1,2-dihydropyridinyl[4,3-d]pyrimidin-4-yl)piperazine-1-carboxylate (100 mg, 0.17 mmol) in dichloromethane (4 mL) was added trifluoroacetic acid (1 mL) under ice-cooling. The mixture was stirred at room temperature for 2 h and concentrated to afford 7-(2-fluoro-6-hydroxyphenyl)-1-(2-isopropyl-4-methylpyridin-3-yl)-4-(piperazin-1-yl)pyridin[4,3-d]pyrimidin-2(1H)-one (82 mg, theoretical) as a yellow oil. ES-API: [M+H] + = 475.2. |
| Step 5: Under ice bath, add N,N-diisopropylethylamine (110 mg, 0.85 mmol) to a solution of 7-(2-fluoro-6-hydroxyphenyl)-1-(2-isopropyl-4-methylpyridin-3-yl)-4-(piperazin-1-yl)pyridin[4,3-d]pyrimidin-2(1H)-one (82 mg, 0.17 mmol) in dichloromethane (3 mL). After the reaction solution becomes clear, add acrylic anhydride (21 mg, 0.17 mmol) dropwise and stir for 5 minutes. The reaction solution is washed with saturated sodium bicarbonate solution (5 mL). The organic phase is dried, concentrated, and purified by preparative HPLC (ammonium bicarbonate system) to obtain a light yellow solid Z26 (12.44 mg, purity: 100%, yield: 14% ) . NMR (500MHz, DMSO) δ12.86(s,1H),9.26(s,1H),8.59(d,J=4.9Hz,1H),7.35(d,J=4.9Hz,1H),7.29(d d,J=15.0,8.2Hz,1H),6.86(dd,J=16.7,10.4Hz,1H),6.77(d,J=8.3Hz,1H),6.73-6.66(m,2H),6.21( dd,J=16.6,2.3Hz,1H),5.77(dd,J=10.4,2.3Hz,1H),4.07(d,J=5.0Hz,4H),3.88(d,J=36.8Hz,4H),2 .76(dt,J=13.6,6.8Hz,1H),1.96(s,3H),1.10(d,J=6.7Hz,3H),1.04(d,J=6.7Hz,3H).ES-API:[M+H] + =529.2. |
SYN
Fulzerasib is an orally active KRAS G12C inhibitor developed by Innovent Biologics. It selectively targets the KRAS G12C mutation in NSCLC [36,37]. In 2024, the NMPA approved Fulzerasib (brand name: Dupert) for treating adult patients with advanced NSCLC harboring the KRAS G12C mutation who have progressed after prior systemic therapy. Fulzerasib irreversibly binds to the KRAS G12C mutant protein, locking it in an inactive GDP-bound state, thereby inhibiting downstream signaling pathways such as MAPK and PI3K. This action effectively suppresses cancer cell proliferation and survival. The clinical efficacy of Fulzerasib was demonstrated in a Phase II trial (NCT05009303) involving patients with advanced NSCLC and KRAS G12C mutations [38]. In the clinical trial, Fulzerasib demonstrated an ORR of 49.1 % and a disease control rate (DCR) of 90.5 %, with a median PFS of 9.7 months, reflecting robust antitumor efficacy. The agent exhibited favorable tolerability, characterized by manageable toxicity. Treatment-related adverse events were predominantly mild to moderate in severity, with the most frequently reported being diarrhea, nausea, and elevated liver enzymes [38]. The safety profile was consistent with other KRAS G12Cinhibitors, making it a viable therapeutic option.
The synthetic route of Fulzerasib, shown in Scheme 9, initiates with H2SO4-mediated decyanation of Fulz-001, affording Fulz-002 [39]. Nitrosation of Fulz-002 with NaNO2 yields Fulz-003, which undergoes
Suzuki-Miyaura coupling with (2-fluoro-6-methoxyphenyl)boronic acid to construct Fulz-004. Phosphochlorination with POCl3 under DIPEA catalysis converts Fulz-004 to Fulz-005. Nucleophilic displacement with methyl (R)-1-N-Boc-piperazine-3-carboxylate assembles Fulz-006. Fe-mediated tandem Mannich cyclization/nitro reduction transforms Fulz-006 into bicyclic amine Fulz-007. Methylation with MeI generates Fulz-008, followed by TFA-mediated Boc cleavage to afford Fulz-009.
Acrylation with acryloyl chloride produces Fulz-010. Selective O-demethylation followed by chiral HPLC resolution delivers Fulzerasib
[36] Y.N. Lamb, Correction: fulzerasib: first approval, Drugs 85 (2025) 281.
[37] Y.N. Lamb, Fulzerasib: first approval, Drugs 84 (2024) 1665–1671.
[38] Q. Zhou, X. Meng, L. Sun, D. Huang, N. Yang, Y. Yu, M. Zhao, W. Zhuang, R. Guo,
Y. Hu, Y. Pan, J. Shan, M. Sun, Y. Yuan, Y. Fan, J. Huang, L. Liu, Q. Chu, X. Wang,
C. Xu, J. Lin, J. Huang, M. Huang, J. Sun, S. Zhang, H. Zhou, Y.L. Wu, Efficacy and
safety of KRASG12C inhibitor IBI351 monotherapy in patients with advanced
NSCLC: results from a phase 2 pivotal study, J. Thorac. Oncol. 19 (2024)
1630–1639.
[39] F. Zhou, T. Jiang, W. He, L. Cai, H. Yang, Z. Liu, J. Lan, Preparation of
Heteroaromatic Ring Dihydropyrimidinone Derivatives as KRAS Gene Mutation
Inhibitors Useful in the Treatment of Cancer, 2021. CN112390818A.
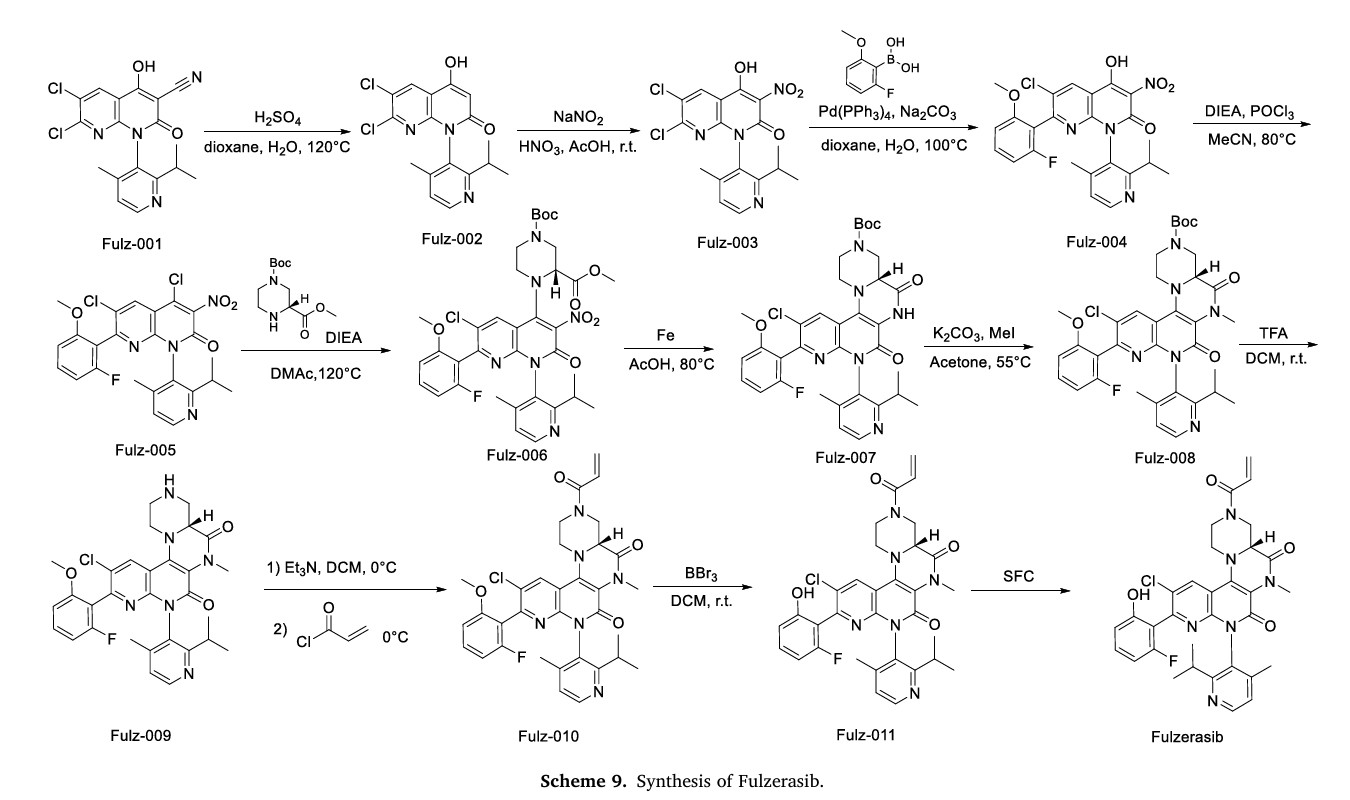
AS ON JUNE2025 4.45 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
……
- [1]. Rafael Rosell, et al. KRAS G12C-mutant driven non-small cell lung cancer (NSCLC). Crit Rev Oncol Hematol. 2024 Mar:195:104228. [Content Brief][2]. Vanesa Gregorc, et al. KROCUS: A phase II study investigating the efficacy and safety of fulzerasib. Free access.June 05, 2024
- New drugs approved by the NMPA in 2024: Synthesis and clinical applicationsPublication Name: European Journal of Medicinal ChemistryPublication Date: 2025-07-05PMID: 40262297DOI: 10.1016/j.ejmech.2025.117643
- Fulzerasib: First ApprovalPublication Name: DrugsPublication Date: 2024-11-26PMID: 39587006DOI: 10.1007/s40265-024-02120-6
- Substituted heterocyclic compounds, their preparation methods and medicinal usesPublication Number: CN-117645614-APriority Date: 2019-10-30
- Substituted heterocyclic fused cyclic compound, preparation method therefor and pharmaceutical use thereofPublication Number: EP-4328229-A2Priority Date: 2019-10-30
- Substituted heterocyclic fused cyclic compound, preparation method therefor and pharmaceutical use thereofPublication Number: US-12054497-B2Priority Date: 2019-10-30Grant Date: 2024-08-06
- Substituted heterocyclic fused cyclic compound, preparation method therefor and pharmaceutical use thereofPublication Number: US-2024158417-A1Priority Date: 2019-10-30
- Substituted heterocyclic fused cyclic compound, preparation method therefor and pharmaceutical use thereofPublication Number: EP-4053118-B1Priority Date: 2019-10-30Grant Date: 2024-10-09
- Substituted heterocyclic and cyclic compounds, their preparation and medical usePublication Number: CN-113853373-BPriority Date: 2019-10-30Grant Date: 2022-08-05
- Substituted heterocyclic ring compound, preparation method and medical application thereofPublication Number: CN-115057872-APriority Date: 2019-10-30
- Substituted heterocyclic fused cyclic compound, preparation method therefor and pharmaceutical use thereofPublication Number: EP-4053118-A1Priority Date: 2019-10-30
- Substituted heterocyclic fused cyclic compound, method for preparing same, and pharmaceutical use thereofPublication Number: KR-20220106765-APriority Date: 2019-10-30
- Substituted heterocyclic fused cyclic compound, preparation method therefor and pharmaceutical use thereofPublication Number: US-2023084095-A1Priority Date: 2019-10-30
- Polymorph of kras inhibitor, preparation method therefor, and use thereofPublication Number: WO-2023116895-A1Priority Date: 2021-12-24
- Polymorph of kras inhibitor, preparation method therefor, and use thereofPublication Number: EP-4455147-A1Priority Date: 2021-12-24
- Polymorph of kras inhibitor, preparation method therefor, and use thereofPublication Number: US-2025051333-A1Priority Date: 2021-12-24
- Key intermediate of kras inhibitor and preparation method thereforPublication Number: WO-2022198904-A1Priority Date: 2021-03-26
- A key intermediate of a KRAS inhibitor and its preparation methodPublication Number: CN-116848111-APriority Date: 2021-03-26
- Pharmaceutical composition, and preparation method therefor and use thereofPublication Number: WO-2024061267-A1Priority Date: 2022-09-21
- Pharmaceutical composition, use thereof, and method for treating cancerPublication Number: WO-2023186075-A1Priority Date: 2022-04-01
- Pharmaceutical composition, use thereof, and method for treating cancerPublication Number: EP-4506004-A1Priority Date: 2022-04-01
- Polymorphs of KRAS inhibitors, methods of making and uses thereofPublication Number: CN-118451081-APriority Date: 2021-12-24
- Polymorph of kras inhibitor and preparation method for polymorph and use thereofPublication Number: TW-202327593-APriority Date: 2021-12-24
////////Fulzerasib, CHINA 2024, APPROVALS 2024, Innovent Biologics, DUPERT, GFH925, GFH 925, IBI351, IBI 351
Golidocitinib
Golidocitinib
CAS 2091134-68-6
- AZD-4205
- AZD4205
- UNII-3BY9Z3M34G
- 3BY9Z3M34G
WeightAverage: 489.584
Monoisotopic: 489.260071274
Chemical FormulaC25H31N9O2
(2R)-N-[3-[2-[(3-methoxy-1-methylpyrazol-4-yl)amino]pyrimidin-4-yl]-1H-indol-7-yl]-2-(4-methylpiperazin-1-yl)propanamide
- (2R)-N-(3-(2-((3-methoxy-1-methylpyrazol-4-yl)amino)pyrimidin-4-yl)-1H-indol-7-yl)-2-(4-methylpiperazin-1-yl)propanamide
- (ALPHAR)-N-(3-(2-((3-METHOXY-1-METHYL-1H-PYRAZOL-4-YL)AMINO)-4-PYRIMIDINYL)-1H-INDOL-7-YL)-ALPHA,4-DIMETHYL-1-PIPERAZINEACETAMIDE
- (2R)-N-[3-[2-[(3-Methoxy-1-methyl-pyrazol-4-yl)amino]pyrimidin-4-yl]-1H-indol-7-yl]-2-(4-methylpiperazin-1-yl)propenamide
- (R)-N-(3-(2-(3-Methoxy-1-methyl-1H-pyrazol-4-ylamino)pyrimidin-4-yl)-1H-indol-7-yl)-2-(4-methylpiperazin-1-yl)propanamide
Approvals 2024, china 2024, DZD 4205, DIZAL, Gao Ruizhe,
Golidocitinib is a pharmaceutical drug for the treatment of cancer. In June 2024, it was given conditional approval in China for the treatment of relapsed or refractory peripheral T-cell lymphoma.[1]
Golidocitinib is classified as a Janus kinase inhibitor.[2][3]
Golidocitinib is an orally available inhibitor of Janus-associated kinase 1 (JAK1), with potential antineoplastic activity. Upon oral administration, golidocitinib inhibits JAK-dependent signaling and may lead to an inhibition of cellular proliferation in JAK1-overexpressing tumor cells. The JAK-STAT (signal transducer and activator of transcription) signaling pathway is a major mediator of cytokine activity and is often dysregulated in a variety of tumor cell types. Additionally, JAK1 may be a primary driver of STAT3 phosphorylation and signaling, which plays a role in neoplastic transformation, resistance to apoptosis, tumor angiogenesis, metastasis, immune evasion, and treatment resistance.
GOLIDOCITINIB is a small molecule drug with a maximum clinical trial phase of II (across all indications) and has 4 investigational indications.
PAT
US9714236, https://patentscope.wipo.int/search/en/detail.jsf?docId=US193702885&_cid=P11-MEHX78-54823-1
Example 32: (2R)—N-(3-{2-[(3-Methoxy-1-methyl-1H-pyrazol-4-yl)amino]pyrimidin-4-yl}-1H-indol-7-yl)-2-(4-methylpiperazin-1-yl)propanamide
| The procedure described above for Example 32 was repeated using the indicated Intermediates to give Examples 33-42 described in Table 12: |
[TABLE-US-00012]
| TABLE 12 Starting m/z ExampleIntermediatesNMR δ (400 MHz)[M + H]+Yield % 3325 and 38DMSO-d6 with D2O 1.28 (3H, d), 2.2750413 (3H, s), 2.73 (3H, s), 2.85-3.34 (8H, m), 3.44 (1H, q), 3.63 (3H, s), 374 (3H, s), 7.04 (1H, t), 7.19 (1H, d), 7.55 (1H, s), 7.91 (1H, s), 8.08 (2H, s), 8.26 (1H, s) -two exchangeable protons not observed3425 and 37DMSO-d6 1.26 (3H, d), 2.16 (3H, s),50472 2.33 (3H, s), 2.38 (4H, s), 2.57-2.62 (4H, m), 3.33 (1H, q), 3.67 (3H, s), 3.79 (3H, s), 7.00 (1H, t), 7.41 (1H, d), 7.66 (1H, s), 7.96 (2H, t), 8.14 (1H, s), 8.22 (1H, s), 9.65 (1H, s), 11.28 (1H, s)3530 and 37Methanol-d4 1.34 (3H, t), 1.40 (3H, d),51816 2.32 (3H, s), 2.37 (3H, s), 2.50-2.80 (8H, m), 3.38 (1H, q), 3.69 (3H, s), 4.34 (2H, q), 7.05-7.20 (2H, m), 7.69 (1H, s), 7.85 (1H, s), 8.23 (1H, s), 8.17 (1H, d)-three exchangeable protons not observed3626 and 37DMSO-d6 1.26 (3H, d), 2.27 (3H, s),52448 2.24-2.52 (4H, m), 2.53-2.70 (4H, m), 3.30-3.36 (1H, m), 3.69 (3H, s), 3.78 (3H, s), 7.02 (1H, s), 7.40 (1H, d), 7.65 (1H, s), 8.32 (1H, s), 8.48 (1H, s), 9.69 (1H, s), 11.42 (1H, s)3727 and 37DMSO-d6 1.26 (3H, d), 2.17 (3H, s),56849 2.23-2.45 (4H, m), 2.46-2.71 (4H, m), 3.30-3.32 (1H, m), 3.68 (3H, s), 3.78 (3H, s), 7.01 (1H, s), 7.37 (1H, d), 7.64 (1H, s), 8.42 (1H, s), 8.45-8.56 (2H, m), 9.70 (1H, s), 11.36 (1H, s)3825 and 39Chloroform-d 1.19 (3H, d), 1.35 (3H, d),51819 2.10 (1H, m), 2.26 (1H, m), 2.38 (6H, m), 2.69 (2H, t), 2.89 (3H, m), 3.72 (3H, s), 3.91 (1H, q), 4.00 (3H, s), 6.57 (1H, s), 6.80 (1H, d), 7.15 (1H, t), 7.68 (1H, d), 7.84 (1H, s), 8.06-8.36 (2H, m), 9.88 (1H, s), 11.15 (1H, s)3929 and 37Methanol-d4 1.34 (3H, t), 1.43 (3H, d),52225 2.35 (3H, s), 2.50-2.85 (8H, m), 3.41 (1H, q), 3.79 (3H, s), 4.24 (2H, q), 7.10- 7.22 (2H, m), 7.68 (1H, s), 8.13 (1H, d), 8.16 (1H, d), 8.43 (1H, s)-three exchangeable protons not observed4031 and 37Methanol-d4 1.33 (3H, t), 1.42 (3H, d),53822 2.35 (3H, s), 2.63-2.71 (4H, m), 2.77- 2.81 (4H, m), 3.42 (1H, q), 3.76 (3H, s), 4.26 (2H, q), 7.10-7.20 (2H, m), 7.70 (1H, s), 8.28 (2H, m), 8.48 (1H, m)-three exchangeable protons not observed4128 and 37Chloroform-d 1.41 (3H, d), 2.29 (3H, s),48836 2.36 (3H, s), 2.42 (3H, s), 2.67-2.80 (8H, m), 3.38 (1H, q), 3.80 (3H, s), 6.42 (1H, s), 6.82 (1H, d), 7.12 (1H, t), 7.69 (1H, d), 7.88 (1H, s), 8.21 (2H, m), 9.74 (1H, s), 11.18 (1H, s)4228 and 38DMSO-d6 1.27 (3H, d), 2.12 (3H, s),4884 2.17 (3H, s), 2.35 (3H, s), 2.40 (4H, s), 2.57-2.63 (4H, m), 3.72 (3H, s), 7.03 (1H, t), 7.43 (1H, d), 7.81 (1H, s), 7.97 (1H, d), 8.19 (2H, m), 8.37 (1H, s), 9.68 (1H, s), 11.33 (1H, s) |
SYN
CN108368091
https://patentscope.wipo.int/search/en/detail.jsf?docId=CN225024309&_cid=P11-MEHXD5-59000-1
| Example 32: (2R)-N-(3-{2-[(3-methoxy-1-methyl-1H-pyrazol-4-yl)amino]pyrimidin-4-yl}-1H-indol-7-yl)-2-(4-methylpiperazin-1-yl)propanamide |
| |
| 3-{2-[(3-methoxy-1-methyl-1H-pyrazol-4-yl)amino]pyrimidin-4-yl}-1H-indol-7-amine (180 mg, 0.54 mmol, Intermediate 23), (R)-2-(4-methylpiperazin-1-yl)propanoic acid dihydrochloride (158 mg, 0.64 mmol, Intermediate 37) and HATU (408 mg, 1.1 mmol) were stirred together in THF (5 mL) to give an orange solution. Diisopropylethylamine (0.38 mL, 2.2 mmol) was added at 25°C. The resulting suspension was stirred at 25°C for 3 hours. The reaction mixture was diluted with ethyl acetate (100 mL) and washed with saturated NaCl. 2 CO 3 The mixture was stirred for 2 hours at 4 ℃ for 10 minutes.Then the mixture was stirred for 2 hours.Then the mixture was stirred for 3 hours.Then the mixture was stirred for 10 minutes.Then the mixture was stirred for 2 hours.Then the mixture was stirred for 3 hours.Then the mixture was stirred for 3 hours.Then the mixture was stirred for 10 minutes.Then the mixture was stirred for 2 hours.Then the mixture was stirred for 3 hours.Then the mixture was stirred for 3 hours.Then the mixture was stirred for 3 hours.Then the mixture was stirred for 3 hours.Then the mixture was stirred for 4 hours.Then the mixture was stirred for 3 hours.Then the mixture was stirred for 3 hours.Then the mixture was stirred for 4 hours.Then the mixture was stirred for 3 hours.Then the mixture was stirred for 3 hours.Then the mixture was stirred for 3 hours.Then the mixture was stirred for 3 hours.Then the mixture was stirred for 4 hours.Then the mixture was stirred for 3 hours . δ (DMSO, 400 MHz) 1.26 (3H, d), 2.16 (3H, s), 2.25-2.45 (4H, m), 2.51-2.70 (4H, m), 3.71 (3H, s), 3.80 (3H, s), 7.05 (1H, t), 7.13 (1H, d), 7.38 (1H, d), 7.70 (1H, s), 8.16-8.31 (4H, m), 9.62 (1H, s), 11.35 (1H, s) – the α-proton of the amide is obscured by the residual water peak; m/z (ES+), [M+H]+=490. |
| The above procedure for Example 32 was repeated using the indicated intermediates to obtain Examples 33-42 described in Table 12: |
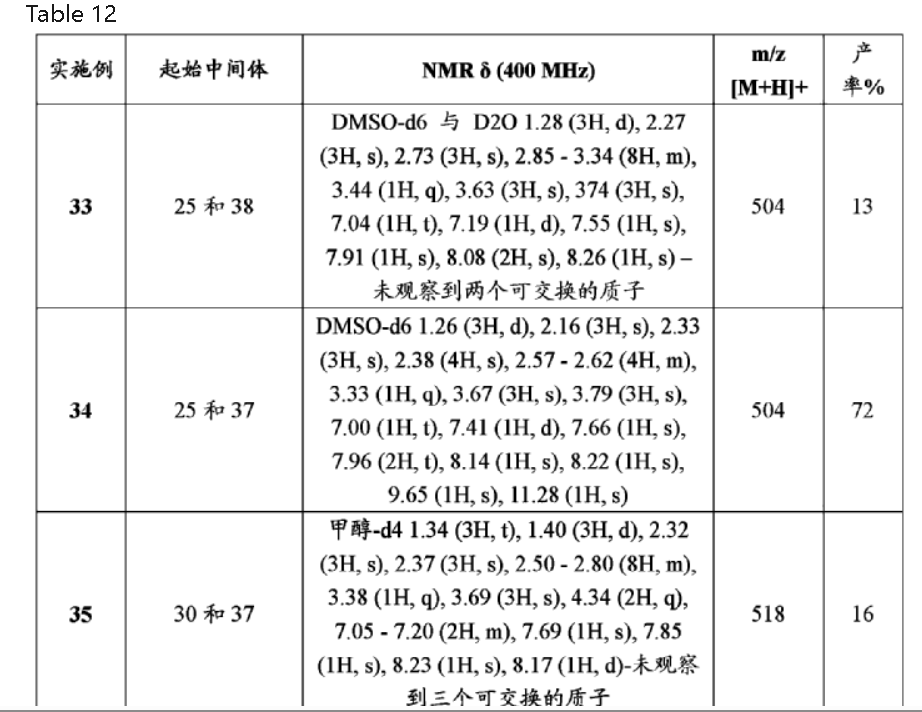
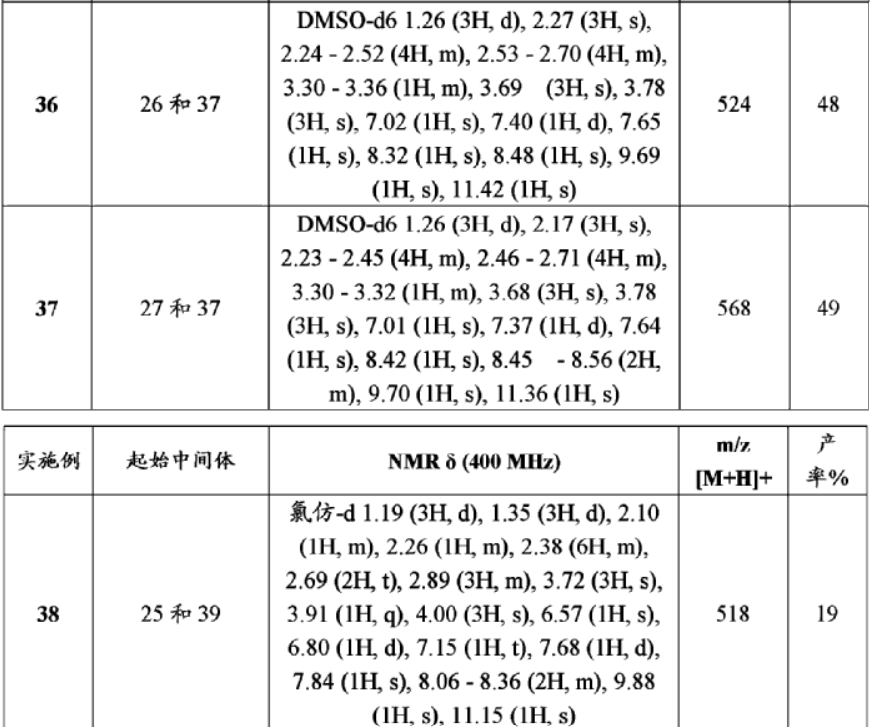
SYN
European Journal of Medicinal Chemistry 291 (2025) 117643
Golidocitinib, also known as DZD4205, is an oral, selective Janus kinase 1 (JAK1) inhibitor developed by Dizal Pharmaceutical. It is designed to target aberrant JAK/STAT signaling pathways implicated in
various malignancies, particularly peripheral T-cell lymphoma (PTCL) [31]. In 2024, Golidocitinib was granted conditional approval by the NMPA under the brand name Gao Ruizhe, for the treatment of adult patients with relapsed or refractory PTCL who have received at least one line of systemic therapy. This agent exerts its therapeutic effects through selective inhibition of JAK1, thereby disrupting the JAK/STAT signaling pathway [32]. This inhibition leads to reduced proliferation and increased apoptosis of malignant T-cells in PTCL [33]. The clinical efficacy of Golidocitinib was demonstrated in the Phase II JACKPOT8 Part B study (NCT04105010), a multinational, single-arm trial evaluating its use in patients with r/r PTCL [34]. The investigation demonstrated an ORR of 44.3 % in patients with PTCL, with sustained efficacy noted across diverse PTCL subtypes. In terms of safety profile, Golidocitinib exhibited favorable tolerability. Hematologic adverse events such as anemia, neutropenia, and thrombocytopenia were the predominant treatment-related toxicities, yet they were effectively controlled through dose modifications and supportive interventions.
The synthetic route of Golidocitinib, shown in Scheme 8, initiates with amino protection of Goli-001 to afford Goli-002 [35]. Bromination of Goli-002 with Br2 yields Goli-003, which undergoes Miyaura bor
ylation with Goli-004 to form Goli-005. Suzuki-Miyaura coupling of Goli-005 with Goli-006 generates Goli-007. Deprotection of Goli-007 produces Goli-008, which undergoes p-TsOH-mediated nucleophilic
substitution with Goli-009 to yield Goli-010. Reduction of Goli-010 affords Goli-011, followed by amidation with Goli-012 to deliver Golidocitinib. Concurrently, Goli-012 is prepared via Tf2 0- Mediated
nucleophilic substitution between Goli-013 and Goli-014.
[31] S.J. Keam, Golidocitinib: first approval, Drugs 84 (2024) 1319–1324.
[32] K. Chen, X. Guan, Z. Yang, Y. Zhou, Z. Liu, X. Deng, D. Liu, P. Hu, R. Chen,
Pharmacokinetic characteristics of golidocitinib, a highly selective JAK1 inhibitor,
in healthy adult participants, Front. Immunol. 14 (2023) 1127935.
[33] M.B. Nierengarten, Golidocitinib favorable for relapsed/refractory T-cell
lymphoma, Cancer 130 (2024) 1191–1192.
[34] Y. Song, L. Malpica, Q. Cai, W. Zhao, K. Zhou, J. Wu, H. Zhang, N. Mehta-Shah,
K. Ding, Y. Liu, Z. Li, L. Zhang, M. Zheng, J. Jin, H. Yang, Y. Shuang, D.H. Yoon,
S. Gao, W. Li, Z. Zhai, L. Zou, Y. Xi, Y. Koh, F. Li, M. Prince, H. Zhou, L. Lin, H. Liu,
P. Allen, F. Roncolato, Z. Yang, W.S. Kim, J. Zhu, Golidocitinib, a selective JAK1
tyrosine-kinase inhibitor, in patients with refractory or relapsed peripheral T-cell
lymphoma (JACKPOT8 part B): a single-arm, multinational, phase 2 study, Lancet
Oncol. 25 (2024) 117–125.
[35] A.B.M. Aastrand, N.P. Grimster, S. Kawatkar, J.G. Kettle, M.K. Nilsson, L.L. Ruston,
Q. Su, M.M. Vasbinder, J.J. Winter-Holt, D. Wu, W. Yang, T. Grecu, J. McCabe, R.
D. Woessner, C.E. Chuaqui, Preparation of Substituted 2-(piperazin-1-yl)-N-[3-[2-
[(1H-pyrazol-4-yl)amino]pyrimidin-4-yl]-1H-indol-7-yl] Propanamide as Selective
JAK1 Inhibitors for Treating Cancers and Immune Disorders, 2017
CN108368091A.
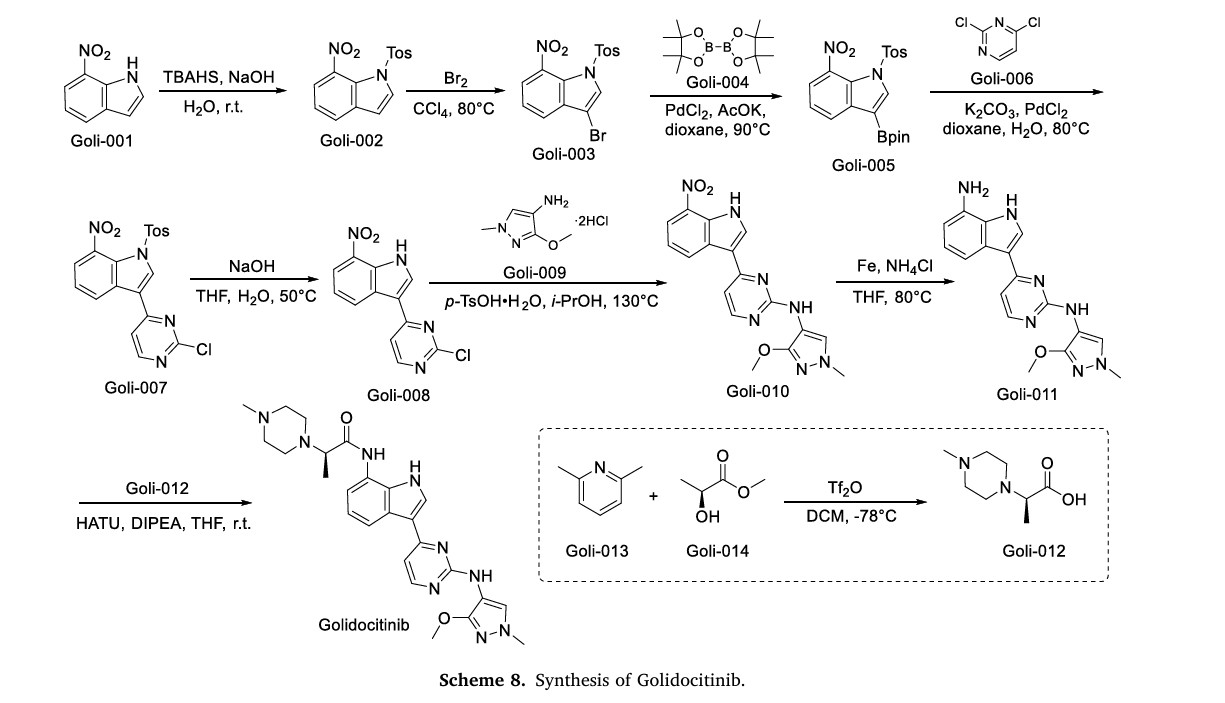
AS ON JUNE2025 4.45 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
……
References
- Keam SJ (October 2024). “Golidocitinib: First Approval”. Drugs. 84 (10): 1319–1324. doi:10.1007/s40265-024-02089-2. PMID 39298087.
- Song Y, Malpica L, Cai Q, Zhao W, Zhou K, Wu J, et al. (January 2024). “Golidocitinib, a selective JAK1 tyrosine-kinase inhibitor, in patients with refractory or relapsed peripheral T-cell lymphoma (JACKPOT8 Part B): a single-arm, multinational, phase 2 study”. The Lancet. Oncology. 25 (1): 117–125. doi:10.1016/S1470-2045(23)00589-2. PMID 38092009.
- Jin J, Zhang L, Zou L, Li Z, Wu H, Zhou K, et al. (2024). “Maintenance Therapy of Golidocitinib, a JAK1 Selective Inhibitor, in Patients with Peripheral T Cell Lymphomas after First-Line Systemic Therapy: Updates of the Phase 2 Study (JACKPOT26)”. Blood. 144: 6368. doi:10.1182/blood-2024-211891.
| Clinical data | |
|---|---|
| Trade names | 高瑞哲 (Gao Ruizhe) |
| Other names | AZD-4205, AZD4205, JAK1-IN-3 |
| Legal status | |
| Legal status | Rx in China |
| Identifiers | |
| IUPAC name | |
| CAS Number | 2091134-68-6 |
| PubChem CID | 126715380 |
| DrugBank | DB18057 |
| ChemSpider | 71117616 |
| UNII | 3BY9Z3M34G |
| KEGG | D12502 |
| ChEMBL | ChEMBL4577523 |
| Chemical and physical data | |
| Formula | C25H31N9O2 |
| Molar mass | 489.584 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| SMILES | |
| InChI | |
- New drugs approved by the NMPA in 2024: Synthesis and clinical applicationsPublication Name: European Journal of Medicinal ChemistryPublication Date: 2025-07-05PMID: 40262297DOI: 10.1016/j.ejmech.2025.117643
- Golidocitinib: First ApprovalPublication Name: DrugsPublication Date: 2024-09-19PMID: 39298087DOI: 10.1007/s40265-024-02089-2
- Recent Developments in the Use of Kinase Inhibitors for Management of Viral InfectionsPublication Name: Journal of Medicinal ChemistryPublication Date: 2021-02-04PMID: 33539089DOI: 10.1021/acs.jmedchem.0c01467
- Discovery of (2R)-N-[3-[2-[(3-Methoxy-1-methyl-pyrazol-4-yl)amino]pyrimidin-4-yl]-1H-indol-7-yl]-2-(4-methylpiperazin-1-yl)propenamide (AZD4205) as a Potent and Selective Janus Kinase 1 InhibitorPublication Name: Journal of Medicinal ChemistryPublication Date: 2020-04-16PMID: 32297743DOI: 10.1021/acs.jmedchem.9b01392
- Sexuality in a healthcare settingPublication Name: Modern healthcare. [Short-term care ed.]Publication Date: 1976-05PMID: 5656
//////////Golidocitinib, approvals 2024, china 2024, DZD 4205, DIZAL, Gao Ruizhe, AZD-4205, AZD4205, UNII-3BY9Z3M34G, 3BY9Z3M34G
Oritinib
Oritinib
- CAS 2035089-28-0
- MESYLATE CAS 2180164-79-6
- SH-1028
- SK593H37SC
- N-[2-[2-(dimethylamino)ethyl-methylamino]-4-methoxy-5-[[4-(6,7,8,9-tetrahydropyrido[1,2-a]indol-10-yl)pyrimidin-2-yl]amino]phenyl]prop-2-enamide
- 539.7 g/mol, C31H37N7O2
- rilertinib
CHINA 2024, Nanjing Sanhome Pharmaceutical.
N-[2-[2-(dimethylamino)ethyl-methylamino]-4-methoxy-5-[[4-(6,7,8,9-tetrahydropyrido[1,2-a]indol-10-yl)pyrimidin-2-yl]amino]phenyl]prop-2-enamide
Oritinib is an investigational new drug currently under investigation for its potential use in cancer treatment.[1][2] As a epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor, oritinib targets specific enzymes involved in the signaling pathways that regulate cell division and survival, which are often dysregulated in cancer cells.[1]
Oritinib (SH-1028), an irreversible third-generation EGFR TKI, overcomes T790M-mediated resistance in non-small cell lung cancer. Oritinib (SH-1028), a mutant-selective inhibitor of EGFR kinase activity, inhibits EGFRWT, EGFRL858R, EGFRL861Q, EGFRL858R/T790M, EGFRd746-750 and EGFRd746-750/T790M kinases, with IC50s of 18, 0.7, 4, 0.1, 1.4 and 0.89 nM, respectively.
PAT
https://patents.google.com/patent/CN115974845B/en
Reaction condition optimization experiment:
The experimental group numbered 1 referred to in table 1 below is the preparation of 1-methyl-3- (2-chloro-4-pyrimidinyl) indole, which was prepared as follows:
To a 10mL reaction tube, 2, 4-dichloropyrimidine (74.5 mg,0.05 mol), zinc triflate (67.3 mg,0.37 equiv), scandium triflate (7.4 mg,0.03 equiv) and 1-methylindole (78.6 mg,1.2 equiv) were added under inert gas atmosphere, and acetonitrile (2.5 mL) were heated to 80℃to react for 24 hours. The reaction was quenched with 30ml of ethyl acetate, the above mixture was added to a separating funnel, 50ml of saturated aqueous sodium carbonate and 50ml of saturated aqueous ammonium chloride were added thereto, and the mixture was shaken for 2 minutes, and the organic phase was taken after the liquid in the separating funnel had settled and separated. The aqueous phase was rinsed with 30ml of ethyl acetate under shaking for 2 times, the whole organic phase was collected, silica gel powder and anhydrous sodium sulfate were added thereto, and the mixture was dried under reduced pressure and packed into a silica gel column. Sequential gradient elution was performed using 250ml (PE: EA: triethylamine 16:4:1), 250ml (PE: EA: triethylamine 15:5:1), 250ml (PE: EA: triethylamine 40:20:3) as developing reagent. The eluent is collected and dried under reduced pressure to obtain pale yellow solid with the yield of 90 percent.
The nuclear magnetic resonance spectrum of 1-methyl-3- (2-chloro-4-pyrimidinyl) indole is as follows:
1H NMR(400MHz,DMSO-d6)δ8.51(d,J=5.9Hz,2H),8.40(dd,1H),7.82(d,J=5.4Hz,1H),7.56(dd,1H),7.28(pd,J=7.1,1.4Hz,2H),3.88(s,3H).
13C NMR(101MHz,DMSO)δ164.55,160.32,158.75,137.84,134.83,125.30,122.81,121.74,121.64,114.43,110.90,110.76,33.31.
PAT
CN109705118
https://patentscope.wipo.int/search/en/detail.jsf?docId=CN242181067&_cid=P20-MEGI3F-20821-1
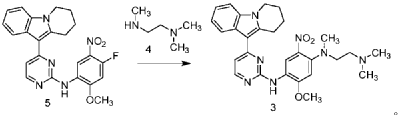
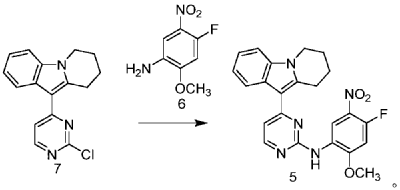
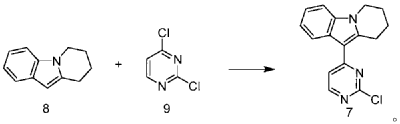
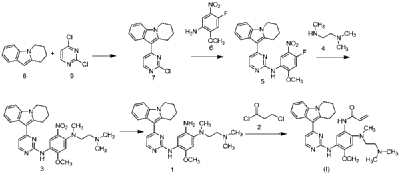
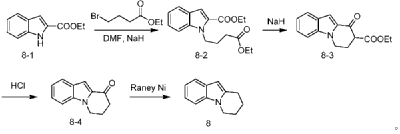
| Step 1: Synthesis of 10-(2-chloropyrimidin-4-yl)-6,7,8,9-tetrahydropyrido[1,2-a]indole |
| |
| In a 100L vertical jacketed glass reactor, add ethylene glycol dimethyl ether (39.15kg) and 2,4-dichloropyrimidine (3.915kg). Cool the solid-liquid mixture to below 10°C, then add anhydrous aluminum chloride (3.855kg) in batches, controlling the addition rate to keep the temperature below 30°C. After the addition is complete, stir at 25±5°C for 30 minutes, then add 6,7,8,9-tetrahydropyrido[1,2-a]indole (4.500kg). Raise the temperature to 60±5°C and react for 3 hours. Monitor by HPLC until the 6,7,8,9-tetrahydropyrido[1,2-a]indole content does not exceed 1.0%, confirming the reaction is complete. The reaction solution was cooled to below 25° C., purified water (90.0 kg) was added, stirred, and filtered. The filter cake was added to acetonitrile (17.8 kg), slurried, filtered, and dried to obtain a yellow powdery solid, a total of 6.652 kg, with a yield of 89.2%. |
| Step 2: Synthesis of N-(4-fluoro-2-methoxy-5-nitrophenyl)-4-(6,7,8,9-tetrahydropyrido[1,2-a]indol-10-yl)pyrimidin-2-amine |
| |
| To a 500L glass-lined reactor, sec-butyl alcohol (80.82kg), 10-(2-chloropyrimidin-4-yl)-6,7,8,9-tetrahydropyrido[1,2-a]indole (6.652kg), 4-fluoro-2-methoxy-5-nitroaniline (4.363kg), and p-toluenesulfonic acid monohydrate (4.816kg) were added to obtain a solid-liquid mixture. The reaction mixture was heated to reflux, and the solid gradually dissolved. As the reaction proceeded, a yellow solid precipitated. After reflux for 7.5 hours, the reaction was monitored by HPLC to confirm completion. Heating was stopped, the reaction mixture was cooled to below 15°C, stirred for 1 hour, and the solid was centrifuged and filtered. Acetonitrile (31.5kg) was added to the filter cake, and the mixture was slurried at 25±5°C for 1.5 hours. The mixture was centrifuged and dried to obtain the title compound, a total of 9.548kg, with a yield of 94.0%. |
| Step 3: Synthesis of N 1 -(2-dimethylaminoethyl)-5-methoxy-N 1 -methyl-2-nitro-N 4 -(4-(6,7,8,9-tetrahydropyrido[1,2-a]indol-10-yl)pyrimidin-2-yl)phenyl-1,4-diamine |
| |
| To a 100 L vertical jacketed glass reactor, add N,N-dimethylacetamide (44.7 kg), N-(4-fluoro-2-methoxy-5-nitrophenyl)-4-(6,7,8,9-tetrahydropyrido[1,2-a]indol-10-yl)pyrimidin-2-amine (9.548 kg), N,N,N’-trimethylethylenediamine (3.380 kg), and N,N-diisopropylethylamine (4.841 kg). Under nitrogen, the reaction mixture was reacted at 85±5°C for 2 hours and monitored by HPLC until the reaction was complete. The reaction solution was cooled to below 70°C, purified water (95.5 kg) was added, filtered, and dried to obtain the title compound, a total of 8.206 kg, with a yield of 72.2%. |
| Step 4: Synthesis of N 1 -(2-(dimethylamino)ethyl)-5-methoxy-N 1 -methyl-N 4 -(4-(6,7,8,9-tetrahydropyrido[1,2-a]indol-10-yl)pyrimidin-2-yl)benzene-1,2,4-triamine |
| |
| A 100 L vertical jacketed reactor was charged with anhydrous ethanol (32.39 kg), purified water (14.32 kg), N 1 -(2-dimethylaminoethyl)-5-methoxy-N 1 -methyl-2-nitro-N 4 -(4-(6,7,8,9-tetrahydropyrido[1,2-a]indol-10-yl)pyrimidin-2-yl)phenyl-1,4-diamine (4.103 kg), reduced iron powder (2.224 kg), and ammonium chloride (2.129 kg). The reaction mixture was refluxed for 1.5 hours and monitored by HPLC until the reaction was complete. The reaction mixture was cooled to below 50°C and filtered through diatomaceous earth to remove the solid. The filtrate was concentrated, and tetrahydrofuran (3.45 kg) and purified water (34.71 kg) were added to the residue. The mixture was slurried, filtered, and dried to obtain 3.244 kg of the title compound in an 84.0% yield. |
| Step 5: Synthesis of N-(2-((2-(dimethylamino)ethyl)(methyl)amino)-4-methoxy-5-((4-(6,7,8,9-tetrahydropyrido[1,2-a]indol-10-yl)pyrimidin-2-yl)amino)phenyl)allylamide |
| |
| Add N,N-dimethylacetamide (48.6 kg) to a 100 L vertical jacketed glass reactor. Raise the temperature to 40°C, then add N₁- ( 2-(dimethylamino)ethyl)-5-methoxy- N₁ -methyl- N₄- (4-(6,7,8,9-tetrahydropyrido[1,2-a]indol-10-yl)pyrimidin-2-yl)benzene-1,2,4-triamine (6.487 kg). Then, begin the dropwise addition of 3-chloropropionyl chloride (1.777 kg). Control the addition rate to no more than 60°C. After the addition is complete, cool the reaction mixture and stir at 40±5°C for 1 hour. Sample the mixture and monitor the reaction by HPLC until complete. Add purified water (0.253 kg) and stir for 30 minutes. |
| The reaction mixture was heated at 80±5°C, triethylamine (13.52 kg) was added, and the temperature was raised to 95±5°C. After reacting for 2 hours, the reaction was complete as determined by HPLC. The temperature was then lowered, and methanol (83.0 kg) was added. The mixture was then cooled and crystallized, filtered, and dried to obtain 4.953 kg of the title compound, with a yield of 68.6% and a purity of 97.37%. |
| Step 6: Purification of N-(2-((2-(dimethylamino)ethyl)(methyl)amino)-4-methoxy-5-((4-(6,7,8,9-tetrahydropyrido[1,2-a]indol-10-yl)pyrimidin-2-yl)amino)phenyl)allylamide |
| Anhydrous ethanol (31.25 kg) was added to a 100 L reactor and heated to above 70°C. The crude N-(2-((2-(dimethylamino)ethyl)(methyl)amino)-4-methoxy-5-((4-(6,7,8,9-tetrahydropyrido[1,2-a]indol-10-yl)pyrimidin-2-yl)amino)phenyl)allylamide prepared in step 5 was added. The reaction mixture was heated and stirred under nitrogen until dissolved. The reaction mixture was cooled to below 10°C, the precipitated solid was centrifuged and dried under vacuum at 60±5°C for more than 12 hours to obtain 4.559 kg of the title compound with a yield of 92.1% and a purity of 98.73%. 1 H NMR (300 MHz, DMSO-d 6 )δ10.20(s,1H),8.65(s,1H),8.34(d,1H),8.11(s,1H),8.06(d,1H),7.43(d, 1H),7.19-7.03(m,3H),6.98(s,1H),6.57-6.41(m,1H),6.28-6.15(m,1H),5.8 2-5.71(m,1H),4.09(t,2H),3.84(s,3H),3.18(t,2H),3.06-2.92(m,2H),2.66 (s,3H),2.47-2.40(m,2H),2.27(s,6H),2.08-1.96(m,2H),1.87-1.74(m,2H). ESI-Ms m/z: 540.3 [M+H] + . |
| Example 2: Synthesis of N-(2-((2-(dimethylamino)ethyl)(methyl)amino)-4-methoxy-5-((4-(6,7,8,9-tetrahydropyrido[1,2-a]indol-10-yl)pyrimidin-2-yl)amino)phenyl)allylamide |
| |
| The preparation method is the same as that in step 5 of Example 1, except that N,N-dimethylacetamide is replaced by N,N-dimethylformamide. The purity of the obtained title compound is 69%. |
| The N-(2-((2-(dimethylamino)ethyl)(methyl)amino)-4-methoxy-5-((4-(6,7,8,9-tetrahydropyrido[1,2-a]indol-10-yl)pyrimidin-2-yl)amino)phenyl)allylamide of the present invention prepared according to the above method has a high yield and purity, mild reaction conditions, easy purification, stable process, easy operation, environmental friendliness, and can meet the requirements of industrial-scale production and application. |
Syn
European Journal of Medicinal Chemistry 291 (2025) 117643
Oritinib represents a third-generation EGFR TKI engineered by Nanjing Sanhome Pharmaceutical. This agent specifically targets both EGFR-sensitizing mutations and the T790 M resistance mutation,
thereby addressing resistance mechanisms linked to prior-generation EGFR-TKIs. In 2024, the NMPA granted approval for Oritinib to treat adult patients with locally advanced or metastatic NSCLC who have experienced disease progression during or following EGFR-TKI therapy and possess confirmed EGFR T790 M mutation-positive status. The mechanism of action of Oritinib involves irreversible binding to mutant EGFR, including the T790 M variant, which in turn suppresses down stream signaling pathways responsible for tumor cell proliferation and survival [28]. The mechanism of Oritinib effectively inhibits tumor growth in patients harboring T790M-mediated resistance to first- and second-generation EGFR-TKIs. Clinical efficacy was established in a Phase II trial (NCT03823807) enrolling patients with EGFR T790 Mmutation-positive NSCLC who had experienced disease progression following prior EGFR-TKI therapy. This study documented an ORR of 60.5 % and a median PFS of 9.6 months, highlighting substantial anti
tumor efficacy in this specific patient cohort. In terms of safety, Oritinib exhibited favorable tolerability. The predominant treatment-related adverse events were rash, diarrhea, and elevated liver enzymes, pri
marily of mild (Grade 1) or moderate (Grade 2) severity. No dose-limiting toxicities were encountered, and the overall safety profile aligned with those observed for other third-generation EGFR-TKIs [29].
The synthetic route of Oritinib Mesylate, shown in Scheme 7, begins with nucleophilic substitution reaction between Orit-001 and Orit-002 to yield Orit-003, which further reacts with Orit-004 via nucleophilic substitution to produce Orit-005 [30]. Orit-005 subsequently undergoes another nucleophilic substitution with Orit-006 to generate Orit-007. Following this, Orit-007 is reduced to form Orit-008. Finally, an amidation reaction between Orit-008 and Orit-009 affords Oritinib.
[28] C. Zhou, A. Xiong, L. Miao, J. Chen, K. Li, H. Liu, Z. Ma, H. Wang, Z. Lu, J. Shen,
P51.03 oritinib (SH-1028), a third-generation EGFR-TKI in advanced NSCLC
patients with positive EGFR T790M: results of a single-arm phase Ib trial,
J. Thorac. Oncol. 16 (2021) S1119–S1120.
[29] C. Zhou, A. Xiong, J. Zhao, W. Li, M. Bi, J. Chen, K. Li, L. Miao, Y. Mao, D. Wang,
7MO oritinib (SH-1028) a third-generation EGFR tyrosine kinase inhibitor in
locally advanced or metastatic NSCLC patients with positive EGFR T790M: results
of a single-arm phase II trial, Ann. Oncol. 33 (2022) S31.
[30] L. Zhao, W. Fu, W. Wu, J. Liu, J. Jin, Method for Preparing Tricyclic Compound as
EGFR Kinase Inhibitor, 2019. CN109705118A.
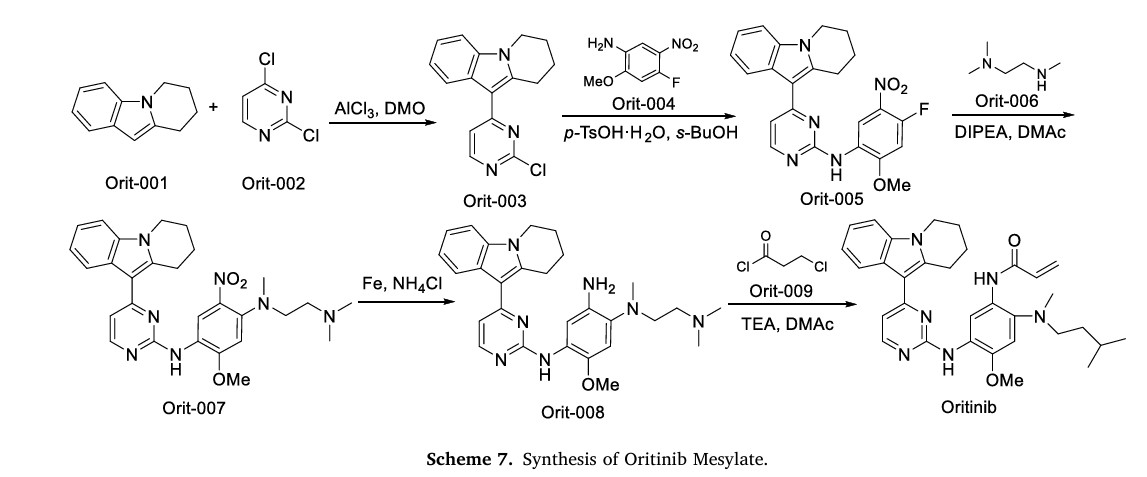
AS ON JUNE2025 4.45 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
……
References
- Xiong A, Ren S, Liu H, Miao L, Wang L, Chen J, et al. (October 2022). “Efficacy and Safety of SH-1028 in Patients With EGFR T790M-Positive NSCLC: A Multicenter, Single-Arm, Open-Label, Phase 2 Trial”. Journal of Thoracic Oncology. 17 (10): 1216–1226. doi:10.1016/j.jtho.2022.06.013. PMID 35798241.
- “Rilertinib – Nanjing Sanhome Pharmaceutical”. AdisInsight. Springer Nature Switzerland AG.
| Clinical data | |
|---|---|
| Other names | SH-1028 |
| Identifiers | |
| IUPAC name | |
| CAS Number | 2035089-28-0 |
| PubChem CID | 122666966 |
| ChemSpider | 115007246 |
| UNII | SK593H37SC |
| Chemical and physical data | |
| Formula | C31H37N7O2 |
| Molar mass | 539.684 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| SMILES | |
| InChI | |
- New drugs approved by the NMPA in 2024: Synthesis and clinical applicationsPublication Name: European Journal of Medicinal ChemistryPublication Date: 2025-07-05PMID: 40262297DOI: 10.1016/j.ejmech.2025.117643
- Safety, efficacy, and pharmacokinetics of SH‐1028 in EGFR T790M‐positive advanced non–small cell lung cancer patients: A dose‐escalation phase 1 studyPublication Name: CancerPublication Date: 2023-02-22PMID: 36813747DOI: 10.1002/cncr.34697
- SH-1028, An Irreversible Third-Generation EGFR TKI, Overcomes T790M-Mediated Resistance in Non-Small Cell Lung CancerPublication Name: Frontiers in PharmacologyPublication Date: 2021-04-27PMCID: PMC8111447PMID: 33986687DOI: 10.3389/fphar.2021.665253
- [1]. Luwei Han, et al. SH-1028, An Irreversible Third-Generation EGFR TKI, Overcomes T790M-Mediated Resistance in Non-Small Cell Lung Cancer. Front Pharmacol. 2021 Apr 27;12:665253. [Content Brief]
/////////Oritinib, CHINA 2024, APPROVALS 2024, 2035089-28-0, SH 1028, SK593H37SC, rilertinib, Oritinib mesylate, Nanjing Sanhome Pharmaceutical,
Envonalkib
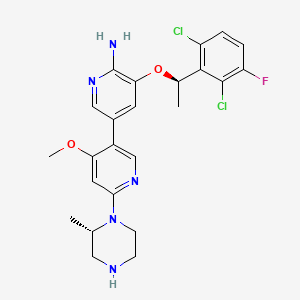
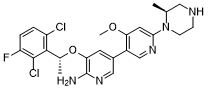
Envonalkib
- CAS 1621519-26-3
- QB7KTQ7VW9
- 5-((1R)-1-(2,6-Dichloro-3-fluorophenyl)ethoxy)-4′-methoxy-6′-((2S)-2-methyl-1-piperazinyl)(3,3′-bipyridin)-6-amine
- 506.4 g/mol, C24H26Cl2FN5O2
TQ-B3139, Chia Tai Tianqing, Anluoqing, cancer
ENVONALKIB is a small molecule drug with a maximum clinical trial phase of II and has 1 investigational indication.
SYN
https://patentscope.wipo.int/search/en/WO2014117718
Example 27: 5-[(2,6-dichloro-3-fluorophenyl)ethoxy-4′-methoxy-6′ …

Step 1: 5-((R)-1-(2,6-dichloro-3-fluorophenyl)ethoxy)-4′-methoxy-6′-((S)-2-methyl-4-tert-butoxycarbonylpiperazin-1-yl)-3,3′-bipyridin-6-amine
To dioxane (10 mL) and water (1.5 mL) were added tert-butyl (S)-4-(5-bromo-4-methoxypyridin-2-yl)-3-methylpiperidin-1-carboxylate (106 mg, 0.275 mmol), (R)-3-(1-(2,6-dichloro-3-fluorophenyl)ethoxy)-5-(4,4,5,5-tetramethyl-1,3,2-dioxaborolan-2-yl)-2-aminopyridine (140 mg, 0.33 mmol), tetrakis(triphenylphosphine)palladium (32 mg, 0.0275 mmol) and cesium carbonate (179 mg, 0.55 mmol), the atmosphere was replaced with nitrogen, and the reaction was carried out at 100 ° C. overnight. After cooling, the mixture was separated by silica gel column chromatography to give 5-(2,6-dichloro-3-fluorophenyl)ethoxy)-4′-methoxy-6-(5-(2-methyl-4-tert-butoxycarbonylpiperidin-1-yl)-3,3′-bipyridin-6-amine) (70 mg) in a yield of 42%. MS m/z [ESI]: 606.2 [M+1].
Step 2: 5-((R)-1-(2,6-dichloro-3-fluorophenyl)ethoxy)-4′-methoxy-6′-((S)-2-methylpiperazin-1-yl)-3,3′-bipyridin-6-amine
To a stirred dichloromethane solution (10 mL) of 5-((R)-1-(2,6-dichloro-3-fluorophenyl)ethoxy)-4′-methoxy-6′-((S)-2-methyl-4-tert-butoxycarbonylpiperidin-1-yl)-3,3′-bipyridin-6-amine (67 mg, 0.11 mmol) was added trifluoroacetic acid (1 mL) and stirred for 1 hour. The pH was adjusted to greater than 13 with sodium hydroxide solution, and the mixture was extracted with dichloromethane. The organic phase was dried over anhydrous sodium sulfate, filtered, and the filtrate was concentrated. The product was separated and purified by column chromatography (with dichloromethane:methanol = 8:1 as eluent) to give 5-((R)-1-(2,6-dichloro-3-fluorophenyl)ethoxy)-4′-methoxy-6′-((S)-2-methylpiperidin-1-yl)-3,3′-bipyridin-6-amine (30 mg). Yield: 55%, MS m/z [ESI]: 506.1[M+1]. 1H-NM (400 MHz, CDC1 3 ):5= 7.94(1H, s), 7.71(1H, s), 7.28-7.32(lH, m), 7.07(1H, t, J=8.4Hz), 6.97(1H, s), 6.04-6.13(2H, m), 4.86 (2H : s), 4.57-4.59(lH, m), 4.03 (1H, d, J=14Hz), 3.76(3H, s), 3.07-3.33(4H, m), 2.88-3.00(lH, m), 1.84(3H, d, J=6.8Hz), 1.34 (3H, d, J=6.8Hz).
SYN
CN107949560
SYN
https://patentscope.wipo.int/search/en/detail.jsf?docId=US154015806&_cid=P11-MEF9W1-27198-1
Example 27: 5-((R)-1-(2,6-dichloro-3-fluorophenyl)ethoxy)-4′-methoxy-6′-((S)-2-methylpiperazin-1-yl)-[3,3′-bipyridin]-6-amine
General Synthetic Methods:
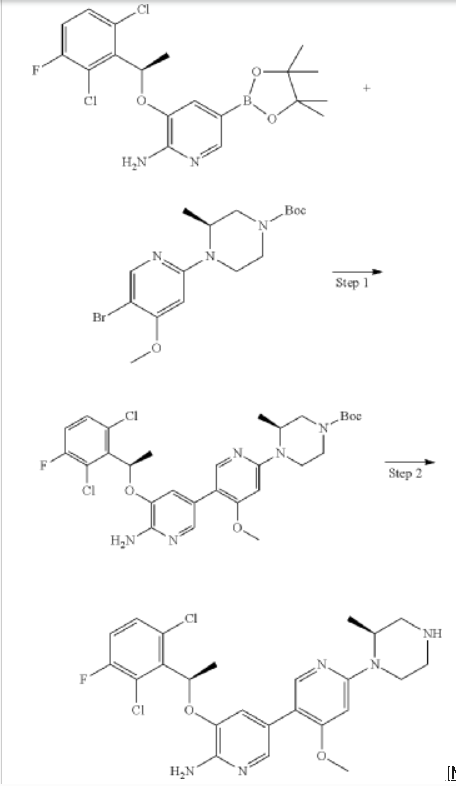
Step 1: (S)-tert-butyl 4-(6′-amino-5′-((R)-1-(2,6-dichloro-3-fluorophenyl)ethoxy)-4-methoxy-[3,3′-bipyridin]-6-yl)-3-methylpiperazine-1-carboxylate
Step 2: 5-((R)-1-(2,6-dichloro-3-fluorophenyl)ethoxy)-4′-methoxy-6′-((S)-2-methylpiperazin-1-yl)-[3,3′-bipyridin]-6-amine
SYN
European Journal of Medicinal Chemistry 291 (2025) 117643
Envonalkib, also known as TQ-B3139, is a novel small-molecule TKI, developed by Chia Tai Tianqing Pharmaceutical Group. It targets ALK, ROS1, and c-Met kinases, exhibiting potent antitumor activity against cancers harboring these genetic alterations. In 2024, the NMPA approved Envonalkib under the brand name Anluoqing for the treatment of adult patients with ALK-positive locally advanced or metastatic NSCLC who have not received prior ALK inhibitor therapy [24]. Envonalkib exerts its therapeutic effects through selective inhibition of the kinase activities of ALK, ROS1, and c-Met, thereby interrupting the downstream signaling pathways that are crucial for tumor cell proliferation and survival [25]. The inhibition of these targets results in cell cycle arrest and apoptosis in cancer cells。The clinical efficacy of Envonalkib was evidenced in a Phase III randomized, open-label, multicenter clinical trial (NCT04009317), which compared Envonalkib with crizotinib in treatment-naïve patients with ALK-positive advanced NSCLC [25,26]. In the reported study, Envonalkib demonstrated a me dian PFS of 24.87 months, which was markedly superior to the 11.60 months achieved with crizotinib (hazard ratio [HR] = 0.47, p < 0.0001). Notably, in patients harboring brain metastases, Envonalkib exhibited a
central nervous system objective response rate (CNS-ORR) of 78.95 %, a substantial improvement over the 23.81 % observed with crizotinib. In terms of safety profile, Envonalkib was generally well-tolerated. Treat ment-related adverse events (TRAEs) of Grade ≥3 were noted in 55.73 % of patients receiving Envonalkib, contrasting with the 42.86 % incidence in the crizotinib cohort. The predominant TRAEs encompassed elevated liver enzymes, neutropenia, and gastrointestinal symptoms, all of which
were amenable to effective management through appropriate support ive care measures. The regulatory approval of Envonalkib thus in troduces a novel therapeutic modality for patients with ALK-positive NSCLC, effectively addressing a significant unmet medical need within this patient population [25].
The synthesis of Envonalkib, illustrated in Scheme 6, initiates with Mitsunobu coupling of Envo-001 and Envo-002, affording Envo-003 [27]. Sequential reduction and NBS-bromination converts Envo-003 to
Envo-005 via Envo-004. Miyaura borylation of Envo-005 constructs Envo-006, which undergoes Suzuki-Miyaura cross-coupling with Envo-007 followed by deprotection to deliver Envonalkib. In parallel,
Envo-009 reacts with Envo-010 through Buchwald-Hartwig cross coupling to form Envo-011. This intermediate is brominated to produce Envo-007, which is used in the Suzuki-Miyaura coupling with Envo-006
[24] X. Li, Y. Xia, C. Wang, S. Huang, Q. Chu, Efficacy of ALK inhibitors in Asian
patients with ALK inhibitor-naïve advanced ALK-Positive non-small cell lung
cancer: a systematic review and network meta-analysis, Transl. Lung Cancer Res.
13 (2024) 2015–2022.
[25] Y. Yang, J. Min, N. Yang, Q. Yu, Y. Cheng, Y. Zhao, M. Li, H. Chen, S. Ren, J. Zhou,
W. Zhuang, X. Qin, L. Cao, Y. Yu, J. Zhang, J. He, J. Feng, H. Yu, L. Zhang, W. Fang,
Envonalkib versus crizotinib for treatment-naive ALK-Positive non-small cell lung
cancer: a randomized, multicenter, open-label, phase III trial, Signal Transduct
Target Ther 8 (2023) 301.
[26] R. Garcia-Carbonero, A. Carnero, L. Paz-Ares, Inhibition of HSP90 molecular
chaperones: moving into the clinic, Lancet Oncol. 14 (2013) e358–e369.
[27] F. Gong, X. Li, R. Zhao, X. Zhang, X. Xu, X. Liu, D. Xiao, Y. Han, Process for
Preparation of Pyridine Substituted 2-aminopyridine Protein Kinase Inhibitor
Crystal, 2017. CN107949560B.

AS ON JUNE2025 4.45 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
……
- New drugs approved by the NMPA in 2024: Synthesis and clinical applicationsPublication Name: European Journal of Medicinal ChemistryPublication Date: 2025-07-05PMID: 40262297DOI: 10.1016/j.ejmech.2025.117643
- Efficacy of ALK inhibitors in Asian patients with ALK inhibitor-naïve advanced ALK-positive non-small cell lung cancer: a systematic review and network meta-analysisPublication Name: Translational Lung Cancer ResearchPublication Date: 2024-08-31PMCID: PMC11384493PMID: 39263024DOI: 10.21037/tlcr-24-604
- Envonalkib versus crizotinib for treatment-naive ALK-positive non-small cell lung cancer: a randomized, multicenter, open-label, phase III trialPublication Name: Signal Transduction and Targeted TherapyPublication Date: 2023-08-14PMCID: PMC10423717PMID: 37574511DOI: 10.1038/s41392-023-01538-w
- Pharmacokinetic, pharmacodynamic, and behavioural studies of deschloroketamine in Wistar ratsPublication Name: British Journal of PharmacologyPublication Date: 2021-10-31PMID: 34519023DOI: 10.1111/bph.15680
//////////Envonalkib, china 2024, approvals 2024, TQ-B3139, TQ B3139, Chia Tai Tianqing, Anluoqing, cancer, QB7KTQ7VW9
DR ANTHONY MELVIN CRASTO

ORGANIC SPECTROSCOPY


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}