
Home » Uncategorized (Page 228)
Category Archives: Uncategorized
 DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HERE
DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HEREFlag and hits
ORGANIC SPECTROSCOPY

SUBSCRIBE

 Subscribe in a reader
Subscribe in a reader
Enter your email address:
Delivered by FeedBurner
Subscribe to New Drug Approvals by Email![]()

![]()



![]()
![]()





Recent Comments
| shivkr2 on SPSR Excellence Award 2025 – S… | |
| Bonkasaurus on Infigratinib phosphate | |
| PALOVAROTENE | ORGAN… on Palovarotene | |
| Pfizer just purchase… on Temanogrel | |
| Pfizer To Cash In On… on Temanogrel |
PHASE1,Progenics Pharmaceuticals’ Novel Small Molecule Drugs Targeting PSMA Successfully Visualize Prostate Cancer, 123-I-MIP-1095

Name: 123-I-MIP-1095
Synonym: 123-I-MIP-1095; [123I]-MIP-1095; iodine I 123 IMP-1095; 2-(3-{l-carboxy-5-[3-(4-iodo-phenyl)-ureido]-pentyl}-ureido)-pentanedioic acid.; [123I]-(S)-2-(3-((S)-1-carboxy-5-(3-(4-iodophenyl)ureido)pentyl)ureido)pentanedioic acid
IUPAC/Chemical name:
2-(3-(1-carboxy-5-(3-(4-iodophenyl)ureido)pentyl)ureido)pentanedioic acid
Chemical Formula: C19H25123IN4O8
Exact Mass: 560.07284
Molecular Weight: 560.33
123-I-MIP-1095
An iodine 123-radiolabled small molecule that exhibits high affinity for prostate-specific membrane antigen (PSMA) with potential use in molecular imaging. 123-I-MIP-1095, a radiolabeled glutamate-urea-lysine analogue, selectively binds PSMA, which allows imaging of PSMA-expressing prostate cancer cells with gamma scintigraph. PSMA is a transmembrane glycoprotein highly expressed by malignant prostate epithelial cells and vascular endothelial cells of various solid tumors.
![]()
| Synonym: | iodine I 123 IMP-1095 | ||
| Chemical structure: | 2-(3-{l-carboxy-5-[3-(4-iodo-phenyl)-ureido]-pentyl}-ureido)-pentanedioic acid | ||
March 5, 2013
Progenics Pharmaceuticals, Inc. (Nasdaq:PGNX) reported positive clinical data from a study of two novel radiolabeled small molecules targeting prostate-specific membrane antigen (PSMA). The imaging agents — 123I-MIP-1072 and 123I-MIP-1095 — had a high sensitivity of lesion detection in bone, tissue and the prostate gland with minimal retention in non-target tissue. The research was published as the cover article in the March issue of The Journal of Nuclear Medicine.
“Existing imaging techniques are limited in their ability to diagnose and stage prostate cancer,” said John J. Babich, Ph.D., senior author of the article “First-in-Man Evaluation of Two High-Affinity PSMA-Avid Small Molecules for Imaging Prostate Cancer.” “The approach described in this paper has the potential to assess disease status more accurately. It could help clinicians select optimal treatments and lead to better patient outcomes.”
Separate phase 1 studies were conducted under an exploratory investigational new drug (IND) application to measure the potential effectiveness of the small molecules in diagnosing and staging prostate cancer. In the first study, seven patients with documented prostate cancer were administered doses of 123I-MIP-1072 and 123I-MIP-1095, two weeks apart. In the second study, six healthy volunteers received 123I-MIP-1072 only. Whole body planar imaging and single photon emission computed tomography (SPECT)/computed tomography (CT) were performed for each group, and pharmacokinetics, tissue distribution, excretion, safety and organ radiation dose were analyzed.
Based on the data reported, Progenics is conductinga global, multi-center phase 2 trial investigating a next generation radiolabeled small molecule targeting PSMA, MIP-1404.
Mark R. Baker, chief executive officer of Progenics, said, “We recently acquired all of the rights to the compounds described in this Journal of Nuclear Medicine paper, as well as to the phase 2 stage imaging agent MIP-1404, through Progenics’ acquisition of Molecular Insight Pharmaceuticals. It is gratifying to see this expansion of our oncology pipeline demonstrating progress so soon.”
Robert J. Israel, M.D., Progenics’ senior vice president of medical affairs and clinical research, said, “We believe that MIP-1404 has excellent potential as a diagnostic radiopharmaceutical. Results to date from the study compounds and MIP-1404 show PSMA as a robust target for prostate cancer molecular imaging, and that a radiolabeled small molecule, which binds PSMA with high affinity, has the potential to detect prostate cancer throughout the body. Cancer treatment guidelines call for imaging prostate cancer with conventional bone scans or MRI. A more accurate method of imaging prostate cancer could be of great value.”
Mr. Baker further added, “Thought leaders in prostate cancer care are focused on avoiding unnecessary surgery and other invasive procedures due to the complications associated with them. Clinicians generally prefer “watchful waiting” when the cancer appears to be indolent. At the same time, some therapeutics to treat aggressive prostate cancer have recently been approved or are under development, such as Progenics’ own PSMA ADC, which currently is in phase 2 testing. Patients and their physicians would benefit from feedback on how therapeutic agents are impacting the course of cancer, and guidance on how and when to use therapeutic agents. It is clear that an improved way to visualize prostate cancer, with a high degree of specificity and sensitivity, would better inform both “watchful waiting” and the treatment of aggressive disease. We believe that data from the ongoing phase 2 trial of MIP-1404 will demonstrate its capabilities to assist prostate cancer patients and their physicians in making these critical decisions.”
About Prostate Cancer
Prostate cancer is the most common form of cancer affecting men in the United States and is the second leading cause of cancer deaths among men each year. The American Cancer Society estimates that in 2013, 238,590 new cases of prostate cancer will be diagnosed and approximately 29,720 American men will die from the disease. Accurate diagnosis and staging of prostate cancer is critical to determining appropriate patient management.
About Progenics
Progenics Pharmaceuticals, Inc. is discovering and developing innovative medicines for oncology, with a pipeline that includes product candidates in preclinical through late-stage development. Progenics’ first commercial product, Relistor® (methylnaltrexone bromide) for opioid-induced constipation, is marketed and in further development by Salix Pharmaceuticals, Ltd. for markets worldwide other than Japan, where Ono Pharmaceutical Co., Ltd. holds an exclusive license for the subcutaneous formulation. For additional information, please visit http://www.progenics.com.
Dalbavancin (Durata Therapeutics) success in Phase III DISCOVER 2 trial for ABSSSI

Durata Therapeutics, Inc. has announced preliminary, top-line results for its DISCOVER 2 (“Dalbavancin for Infections of the Skin COmpared to Vancomycin at an Early Response”) Phase III study of dalbavancin, which is under investigation for the treatment of acute bacterial skin and skin structure infections (ABSSSI) caused by susceptible gram-positive bacteria, including methicillin resistant Staphylococcus aureus (MRSA). DISCOVER 2 results follow the recent release of data from DISCOVER 1, which also met its primary and secondary endpoints.
Preliminary top-line data show that dalbavancin achieved its primary endpoint of non-inferiority (10% non-inferiority margin) at 48-72 hours after initiation of therapy, as determined by the cessation of spread of the lesion, as well as the resolution of fever. Researchers were comparing two intravenous (IV) doses of dalbavancin given one week apart with twice-daily vancomycin doses for 14 days. Patients…
View original post 78 more words
Ziopharm Oncology will be releasing its Phase III results for its drug Palifofsamide towards the end of March 2013

(Zymafos; ZIO-201) is a cytotoxic, active metabolite of the alkylating agent ifosfamide, which causes irreparable DNA interstrand cross-linking in cancer cells. This prevents DNA replication and cell division, leading to cell death.
In contrast to ifosfamide, palifosfamide is not metabolised to the toxins acrolein and chloracetaldehyde, which are associated with haemorrhagic cystitis, and neuro- and nephro-toxicities respectively. Also, palifosfamide is not a substrate for aldehyde dehydrogenase (ALDH), an important mediator of drug resistance

Cyclophosphamide and ifosfamide are nitrogen mustard alkylating agents that act by crosslinking DNA strands at the guanine N-7 position, resulting in cell death. Both of these are prodrugs that are metabolised in the liver to phosphoramide mustard active metabolites, but their use is limited by toxic side-effects. They are also prone to tumour resistance, which results from numerous mechanisms, including DNA repair.
In an attempt to overcome some of these problems, Ziopharm Oncology has developed palifosfamide tromethamine, which is a salt formulation of isophosphoramide mustard, the active metabolite of isofosfamide.1

isofosamide
In a Phase I trial, it was given in combination with doxorubicin to 13 patients with advanced refractory tumours – eight with soft tissue sarcoma and the remainder with small cell lung cancer – for whom there was no available standard therapy.2 It was given on the first three days of a three-week cycle, with a starting dose of 150mg/m2, and doxorubicin given on the first day at a starting dose of 60mg/m2. The doses were escalated to a maximum tolerated dose of 150mg/m2 for palifosfamide and 75mg/m2 for doxorubicin. It was well tolerated, and three of the 12 assessable patients had a partial response, two of whom were from the sarcoma group, and the median progression free survival was 20 weeks.
references
1. S. Jung and B. Kasper, IDrugs 2010, 13, 38
2. L.J. Camacho et al. J. Clin. Oncol. 2009, 27 (Suppl.), Abst. 10577
3. C.F. Verschraegen et al. J. Clin. Oncol. 2010, 28 (Suppl.), A
Palifosfamide, A Novel Molecule for the Treatment of Soft Tissue Sarcoma
Palifosfamide (Zymafos™ or ZIO-201) references a novel composition (tris formulation) that is the functional active metabolite of ifosfamide (IFOS), a bi-functional DNA alkylator being investigated as a potential therapy for the treatment of soft tissue sarcoma (STS). Palifosfamide is formulated by combining the tris (hydroxymethyl) amino methane (tris) salt of palifosfamide and a number of excipients to create the final drug product. Preclinical development of palifosfamide has included in vitro and in vivo studies demonstrating activity against various sarcomas, breast cancers, other solid tumors and leukemias, including several that are resistant to IFOS. Several clinical studies have been initiated in a variety of cancer types. A Phase I study in advanced cancers, using the original lysine formulation, has been completed. A two-stage Phase I/II Study in advanced sarcomas, introducing the tris salt formulation, has completed enrollment and data retrieval is ongoing. A Phase I study in combination with doxorubicin evaluating patients with advanced, refractory solid tumors for whom treatment with doxorubicin is considered medically acceptable, has completed enrollment and data retrieval is ongoing. Based on the result of the Phase I combination study, an international randomized Phase II study comparing palifosfamide in combination with doxorubicin versus doxorubicin alone in 1st and 2nd line patients with advanced STS has been completed. phase 3 on now also
What is Soft Tissue Sarcoma, and what are the currently available treatments?
Soft-tissue sarcomas (STS) represent a rare and diverse group of tumors that are not very well understood. Although soft-tissue sarcomas account for <1% of all cancers, they represent a high percentage of cancer-related deaths worldwide (Ref. 3, Ref. 4, Ref. 5). STS tumors can occur anywhere within the body, originating in various soft tissues including fat, smooth or striated muscle, nerve/nerve sheath, vascular tissue, and other connective tissues; the extremities are the most common site of origin, accounting for approximately 50% of cases
Novo’s long-acting insulin, name-insulin degludec , Tresiba makes way to UK

 DEGLUDEC
DEGLUDEC
B29N(epsilon)-omega-carboxypentadecanoyl-gamma-L-glutamyl desB30 human insulin
Insulin degludec is a ultralong-acting basal insulin analogue being developed by Novo Nordisk under the brand name Tresiba. It is injected subcutaneously three-times a week to help control the blood sugar level of those with diabetes. It has a duration of action that lasts up to 40 hours, unlike the 18 to 26 hours provided by current marketed long-acting insulins such as insulin glargine and insulin detemir.

Insulin degludec is a modified insulin that has one single amino acid deleted in comparison to human insulin, and is conjugated to hexadecanedioic acid via gamma-L-glutamyl spacer at the amino acid lysine at position B29.
MARCH 05, 2013
Patients with diabetes in the UK can now get access to a new treatment option following the roll out of Novo Nordisk’s ultra-long-acting insulin Tresiba in the country, marking its first launch in Europe.
Tresiba (insulin degludec) is a once-daily basal insulin which, conveniently, can be administered at any time of the day and, thereby, is the first to offer diabetics flexibility in the timing of taking insulin, according to the firm.
The European Commission issued a green light for the drug – as well as sister product Ryzodeg (insulin degludec/insulin aspart) – for the treatment of diabetes in adults back in January.
Approval came on the back of studies comparing Tresiba to Sanofi’s blockbuster Lantus (insulin glargine), in which Novo’s drug demonstrated a significantly lower risk of overall and nocturnal hypoglycaemia, which is particularly important as patients are less aware of the symptoms, while successfully achieving equivalent reductions in HbA1c.
In fact, clinical data showed a 25% reduction in nocturnal hypoglycaemia for patients with type I diabetes taking Tresiba, while for insulin-naiive patients with Type II diabetes there was a 36% reduction compared to Lantus, the company said, although noting hypoglycaemia is still the most common side effect linked with its drug.
“With our current insulin treatments, it is important for people with diabetes to take their long-acting insulin at around the same time each day. However, the pharmacokinetics of insulin degludec mean that, on occasions when this is not possible, people with diabetes can alter the time they take their insulin without compromising their diabetes control or putting themselves at increased risk of hypoglycaemia,” commented Professor Richard Holt, Professor in Diabetes and Endocrinology at the University of Southampton.
“Good control of diabetes is essential to reduce the risk of long-term complications, so flexibility, when needed, is important,” he added.
Competitive edge?
In addition, its associated cut in the risk of nocturnal hypoglycaemia could give the drug another competitive edge, given that almost 50% of severe hypoglycaemic episodes – which have a significant impact not only on the patient but on the economy – occur at night.
The estimated UK cost for severe hypoglycaemia hit £30.4 million and £41.8 million for moderate hypoglycaemia in 2010/11, and each severe hypoglycaemic episode involving hospitalisation costs the NHS an estimated £2,153 per person.
The drug does come with a weighty price-tag, costing £72.00 per pack of 5 x 3 ml U100 FlexTouch pens, compared to the £41.50 per pack (5 x 3ml pre-filled pens) of Lantus. But a spokesperson for Novo stressed to PharmaTimes UK News that its price “reflects the clinical benefits and innovation that insulin degludec brings to patients”.
The National Institute for Health and Clinical Excellence will include Tresba its updated NICE Clinical Guidelines on diabetes, which are expected in 2014, the spokesperson confirmed.
Last month Novo was dealt a huge blow when US regulators knocked back Tresiba, after being reluctant to approve the drug without additional data on its cardiovascular effects.
The move came as somewhat of a surprise, given that advisers to the US Food and Drug Administration actually supported its approval, albeit with the proviso that a post-marketing cardiovascular outcomes trial be carried out.
NDA-US Marketing by Ranbaxy, Alembic has announced that it has received an NDA approval for extended release version of Pfizer’s anti depressant drug Pristiq, Desvenlafaxine Base

DESVENLAFAXINE
read at
5 march 2013
Alembic has announced that it has received an NDA approval for extended release version of Pfizer’s anti depressant drug Pristiq. Pristiq sell approximately $550m in the US. Alembic has outlicensed rights to Ranbaxy for marketing in the US. The company will start marketing the product immediately.
Alembic will manufacture and supply the drug to Ranbaxy for marketing in the US. Vadodara-based pharma player, Alembic Pharmaceuticals Limited has received the approval from the US Food and Drug Administration (USFDA) for a bioequivalent version of Pristiq by Pfizer.
Phase 3 , breast cancer, Ridaforolimus (MK-8669; AP23573; formerly Deforolimus) Merck, license,Ariad Pharmaceuticals

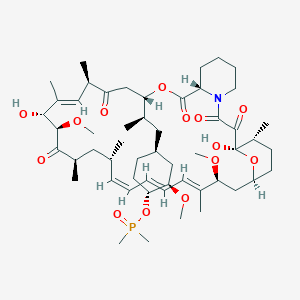
Ridaforolimus
572924-54-0
(1R,2R,4S)-4-[(2R)-2-[(1R,9S,12S,15R,16E,18R,19R,21R,23S,24E,26E,28Z,30S,32S,35R)-1,18-dihydroxy-19,30-dimethoxy-15,17,21,23,29,35-hexamethyl-2,3,10,14,20-pentaoxo-11,36-dioxa-4-azatricyclo[30.3.1.04,9]hexatriaconta-16,24,26,28-tetraen-12-yl]propyl]-2-methoxycyclohexyl dimethylphosphinate
Dimethyl-phosphinic Acid C-43 Rapamycin Ester
42-(dimethylphosphinate) Rapamycin
- AP 23573
- AP23573
- Deforolimus
- MK 8669
- MK-8669
- MK8669
- Ridaforolimus
- Taltorvic
- UNII-48Z35KB15K
An mTOR inhibitor for the treatment of cancer.
Ridaforolimus (MK-8669; AP23573; formerly Deforolimus)
Merck, under exclusive worldwide license agreement with Ariad Pharmaceuticals
Method of Action: Oral inhibitor of mammalian target of rapamycin inhibitor (mTOR)
Indications/Phase of Trial: Maintenance therapy for metastatic soft-tissue sarcoma and bone sarcomas after at least four chemotherapy cycles (under review after receiving Complete Response letter from FDA in June; NME)
Ridaforolimus is an investigational small-molecule inhibitor of the protein mTOR, a protein that acts as a central regulator of protein synthesis, cell proliferation, cell cycle progression and cell survival, integrating signals from proteins, such as PI3K, AKT and PTEN, known to be important to malignancy.
TARGET- mTOR
Ridaforolimus (also known as AP23573 and MK-8669; formerly known as Deforolimus[1]) is an investigational targeted and small-molecule inhibitor of the protein mTOR, a protein that acts as a central regulator of protein synthesis, cell proliferation, cell cycle progression and cell survival, integrating signals from proteins, such as PI3K, AKT and PTEN known to be important to malignancy. Blocking mTOR creates a starvation-like effect in cancer cells by interfering with cell growth, division, metabolism, and angiogenesis.
It has had promising results in a clinical trial for advanced soft tissue and bone sarcoma.
RIDAFOROLIMUS
NMR….http://file.selleckchem.com/downloads/nmr/S102201-Deforolimus-HNMR-Selleck.pdf
HPLC . http://file.selleckchem.com/downloads/hplc/S102201-Deforolimus-HPLC-Selleck.pdf
MSDS..http://www.selleckchem.com/msds/Deforolimus-MSDS.html
| Commercial arrangements |
Ridaforolimus is being co-developed by Merck and ARIAD Pharmaceuticals. On May 5, 2010, Ariad Pharmaceuticals and Merck & Company announced a clinical development and marketing agreement. With this agreement, Ariad received $125 million in upfront payments from Merck and $53 million in milestone payments. Future payments are triggered upon acceptance of the NDA by the FDA with another payment when the drug receives marketing approval. There are similar milestones for acceptance and approval in both Europe and Japan. Other milestone payments are tied to revenue goals for the drug.[2] ARIAD has opted to co-promote ridaforolimus in the U.S. Merck plans to submit a New Drug Application (NDA) for ridaforolimus to the U.S. Food and Drug Administration (FDA) and a marketing application in the European Union in 2011.[3]
Clinical trials
Phase III SUCCEED
On June 6, 2011, Ariad and Merck announced detailed results from the largest randomized study ever in the soft tissue and bone sarcoma population, the Phase III SUCCEED clinical trial. SUCCEED evaluated oral ridaforolimus, in patients with metastatic soft-tissue or bone sarcomas who previously had a favorable response to chemotherapy. In this patient population, ridaforolimus improved progression-free survival (PFS) compared to placebo, the primary endpoint of the study. The complete study results were presented by Sant P. Chawla, M.D., director, Sarcoma Oncology Center, Santa Monica, CA, during the 2011 American Society of Clinical Oncology (ASCO) annual meeting.
The SUCCEED (Sarcoma Multi-Center Clinical Evaluation of the Efficacy of Ridaforolimus) trial was a randomized (1:1), placebo-controlled, double-blind study of oral ridaforolimus administered at 40 mg/day (five of seven days per week) in patients with metastatic soft-tissue or bone sarcomas who previously had a favorable response to chemotherapy. Oral ridaforolimus was granted a Special Protocol Assessment (SPA) by the FDA for the SUCCEED trial.
Based on 552 progression-free survival (PFS) events in 711 patients, (ridaforolimus (N=347), placebo (N=364) determined by an independent radiological review committee, the study achieved its primary endpoint of improvement in PFS, with a statistically significant (p=0.0001) 28 percent reduction in the risk of progression or death observed in those treated with ridaforolimus compared to placebo (hazard ratio=0.72).
Median PFS was 17.7 weeks for those treated with ridaforolimus compared to 14.6 weeks in the placebo group. Furthermore, based on the full analysis of PFS determined by investigator assessment, there was a statistically significant (p<0.0001) 31 percent reduction by ridaforolimus in the risk of progression or death compared to placebo (hazard ratio=0.69). In the investigator assessment analysis, median PFS was 22.4 weeks for those treated with ridaforolimus compared to 14.7 weeks in the placebo group [4
EU WITHDRAWAL IN NOV 2012
Merck, known as MSD outside the U.S. and Canada, announced today that it has formally notified the European Medicines Agency (EMA) of Merck’s decision to withdraw the Marketing Authorisation Application (MAA) for ridaforolimus.
The application for Marketing Authorisation for ridaforolimus was accepted by the EMA in August 2011. At the time of the withdrawal it was under review by the Agency’s Committee for Medicinal Products for Human Use (CHMP). In its letter to the EMA, Merck said that the withdrawal of ridaforolimus was based on the provisional view of the CHMP that the data available to date and provided in the Marketing Authorisation Application were not sufficient to permit licensure of ridaforolimus in the European Union for the maintenance treatment of patients with soft tissue sarcoma or primary malignant bone tumor.
Although the application for these uses was withdrawn, Merck is studying ridaforolimus in combination with other drugs in other tumor types. The withdrawal of the European application of ridaforolimus for the maintenance treatment of patients with soft tissue sarcoma or primary malignant bone tumor does not change Merck’s commitment to the ongoing clinical trials with ridaforolimus.
Description
42-(dimethylphosphinate) Rapamycin (Ridaforolimus) represented by the following formula I:

2. Description of RelatedArt
The mammalian target of Rapamycin (mTOR) is known as a mechanistic target of Rapamycin (H), which is found in the studies of Rapamycin. On the other hand, 42-(dimethylphosphinate) Rapamycin (Ridaforolimus) (I) is a derivative of Rapamycin (II), which is also a kind of mTOR inhibitor. Ridaforolimus (I) can inhibit cell division and possibly lead to tumor cell death. Hence, there are many studies related to solid tumor treatments and blood cancer treatments using Ridaforolimus (I). In addition, in 2011, Merck also applied a certification of this compound against soft tissue and bone cancer.
U.S. Pat. No. 7,091,213 discloses a process for preparing 42-(dimethylphosphinate) Rapamycin (Ridaforolimus) (I), and the process thereof is shown in the following Scheme I.

In this process, a solution of Rapamycin (II) in dichloromethane (DCM) was respectively added with 2,6-di-tert-butyl-4-methylpyridine or 3,5-lutidine as a base, and followed by the addition of a solution of dimethylphosphinic chloride (DMP-Cl) to perform a phosphorylation reaction at 0° C., under a stream of N2(g). The crude product was purified by flash chromatography (eluted with MeOH/DCM/EtOAc/hexane=1:10:3:3) to provide 42-(dimethyl- phosphinate) Rapamycin (Ridaforolimus) (I), which is a phosphorylated compound at 42-hydroxyl position of Rapamycin (II). In addition, this patent also disclosed a side product of 31,42-bis(dimethyl phosphinate) Rapamycin (III), which is a phosphorylated compound at both 31- hydroxyl position and 42- hydroxyl position of Rapamycin (II).
…………………..
SYNTHESIS
Some additional transformations of potential interest to the practitioner are shown below, including the preparation of reagents for generating the described C-43 phosphorus-containing rapalogs:
Preparation of Diakyl/diaryl Chlorophoshates

Preparation of Alkyl Halide Phosphonates

Illustrative routes for using the foregoing sorts of reagents to prepare certain rapalogs of this invention are shown below.

The synthesis of compounds of this invention often involves preparation of an activated form of the desired moiety “J”, such as a phosphoryl chloride as shown above (e.g. (R)(RO)P—Cl or RR′P(═O)—Cl, etc), and reaction of that reagent with rapamycin (or the appropriate rapalog) under conditions yielding the desired product, which may then be recovered from residual reactants and any undesired side products. Protecting groups may be chosen, added and removed as appropriate using conventional methods and materials.
Purification of Compounds of the Invention
A variety of materials and methods for purifying rapamycin and various rapalogs have been reported in the scientific and patent literatures and may be adapted to purification of the rapalogs disclosed herein. Flash chromatography using a BIOTAGE prepacked cartridge system has been particularly effective. A typical protocol is disclosed in the Examples which follow.
Physicochemical Characterization of Compounds of the Invention
The identity, purity and chemical/physical properties of the rapalogs may be determined or confirmed using known methods and materials, including HPLC, mass spectral analysis, X ray crystallography and NMR spectroscopy. High resolution 1D 1H and 31P NMR spectra acquired using a typical relaxation delay of 3 seconds have proved useful, as has reverse phase HPLC analysis (analytical column, 3 micron particle size, 120 ansgstrom pore size, thermostatted to 50° C. with a mobile phase of 50% acetonitrile, 5% methanol and 45% water (all % s by volume), for example, in an isocratic elution system, with elution of product and impurity peaks followed by UV detection at 280 nanometers). Normal phase HPLC may also be used, especially to evaluate the level of residual rapamycin or rapalog by-products. The presence of residual solvent, heavy metals, moisture and bioburden may be assessed using conventional methods.
Example 9
Dimethyl-phosphinic Acid C-43 Rapamycin Ester

Dimethyl-phosphinic Acid C-43 Rapamycin Ester
To a cooled (0° C.) solution of rapamycin (0.1 g, 0.109 mmol) in 1.8 mL of dichloromethane was added 0.168 g (0.82 mmol) of 2,6-di-t-butyl-4-methyl pyridine, under a stream of N2, followed immediately by a solution of dimethylphosphinic chloride (0.062 g, 0.547 mmol) in 0.2 mL of dichloromethane. The slightly yellow reaction solution was stirred at 0° C., under an atmosphere of N2, for 3.5 h (reaction monitored by TLC). The cold (0° C.) reaction solution was diluted with ˜20 mL EtOAc then transferred to a separatory funnel containing EtOAc (150 mL) and saturated NaHCO3 (100 mL). Upon removing the aqueous layer, the organic layer was washed successively with ice cold 1N HCl (1×100 mL), saturated NaHCO3 (1×100 mL), and brine (1×100 mL), then dried over MgSO4 and concentrated. The crude product was purified by silica gel flash chromatography (eluted with 1:10:3:3 MeOH/DCM/EtOAc/hexane) to provide 0.092 g of a white solid:
1H NMR (300 MHz, CDCl3) d 4.18 (m, 1H), 4.10 (m, 1H), 3.05 (m, 1H), 1.51 (m, 6H);
31P NMR (121 MHz, CDCl3) d 53.6; 1013 m/z (M+Na).
Example 9
Alternative Synthesis
Rapamycin and dichloromethane are charged into a nitrogen-purged reaction flask. The stirred solution is cooled to approximately 0° C. (an external temperature of −5±5° C. is maintained throughout the reaction). A solution of dimethylphosphinic chloride (2.0 molar equivalents) in dichloromethane is then added over a period of approximately 8–13 minutes.
This is followed immediately by the addition of a solution of 3,5-lutidine (2.2 molar equivalents) in dichloromethane over a period of approximately 15–20 minutes. Throughout both additions, the internal temperature of the reaction sssstays below 0° C. The cooled reaction solution is stirred for 1 hour and then transferred, while still cold, to an extractor containing saturated aqueous NaHCO3 and methyl-t-butyl ether (MTBE), ethyl acetate or diethyl ether. In-process samples are removed at 30 and 60 minute time points.
Samples are prepared in a similar fashion to that described for the reaction workup. Reaction progress is monitored by TLC (1:10:3:3 MeOH/DCM/EtOAc/hexanes) and reverse-phase HPLC analyses. The isolated organic layer is successively washed with ice cold 1N HCl, saturated aqueous NaHCO3 (2×), saturated aqueous NaCl, and dried over sodium sulfate. Upon filtration and solvent removal, the residue undergoes solvent exchange with acetone followed by concentration in vacuo to provide crude product, which may be analyzed for purity by normal- and reversed-phase HPLC.
…………………….
SYNTHESIS
The process of the present invention is shown in the following Scheme II.


- “ARIAD Reports First Quarter 2009 Development Progress and Financial Results- Ridaforolimus New USAN Name to Replace Deforolimus”. ARIAD Pharmaceuticals. 2009. Retrieved 2009-05-07.
- “ARIAD – News release”. Phx.corporate-ir.net. Retrieved 2012-10-07.
- “ARIAD – News release”. Phx.corporate-ir.net. 2011-03-17. Retrieved 2012-10-07.
- “ARIAD – News release”. Phx.corporate-ir.net. 2011-06-06. Retrieved 2012-10-07.
|
7-11-2012
|
FULLY HUMAN ANTI-VEGF ANTIBODIES AND METHODS OF USING
|
|
|
10-28-2011
|
METHODS OF TREATMENT
|
|
|
1-21-2011
|
ANTI-IGF1R
|
|
|
1-5-2007
|
Methods for treating neurofibromatosis 1
|
|
|
4-16-2004
|
Phosphorus-containing compounds and uses thereof
|

The European Medicines Agency (EMA) has approved Roche’s PERJETA (pertuzumab) for patients with previously untreated HER2-positive metastatic breast cancer (mBC)

The structure of HER2 and pertuzumab
march 4, 2013
Pertuzumab (also called 2C4, trade name Perjeta) is a monoclonal antibody. The first of its class in a line of agents called “HER dimerization inhibitors”. By binding to HER2, it inhibits the dimerization of HER2 with other HER receptors, which is hypothesized to result in slowed tumor growth.[1] Pertuzumab received US FDA approval for the treatment of HER2-positive metastatic breast cancer on June 8, 2012.[2] Pertuzumab was developed at Genentech and is now owned by Roche which acquired Genentech in 2009.
Clinical trials
Early clinical trials of pertuzumab in prostate, breast, and ovarian cancers have been met with limited success.[3]
The dosage of pertuzumab used in the pivotal phase III CLEOPATRA (Clinical Evaluation of Pertuzumab and Trastuzumab) trial was as follows: IV 840 mg loading dose followed by IV 420 mg every three weeks.[4]
The pharmacokinetics of intravenous pertuzumab appear to be unaffected by age and no drug-drug interaction has been reported with docetaxel. The pharmacokinetics and pharmacodynamics of pertuzumab were summarized in a Feb 2012 review by Gillian Keating.[4]
The combination of pertuzumab plus trastuzumab plus docetaxel, as compared with placebo plus trastuzumab plus docetaxel, when used as first-line treatment for HER2-positive metastatic breast cancer, significantly prolonged progression-free survival, with no increase in cardiac toxic effects in the randomized, double-blind, multinational, phase III CLEOPATRA trial.[5]
Intravenous pertuzumab is currently being evaluated in patients with breast cancer in the following trials: MARIANNE (advanced breast cancer), NEOSPHERE (early breast cancer), TRYPHAENA (HER2-positive stage II/III breast cancer) and APHINITY (HER2-positive nonmetastatic breast cancer).[4]
References
- de Bono, Johann S.; Bellmunt, J; Attard, G; Droz, JP; Miller, K; Flechon, A; Sternberg, C; Parker, C et al. (20 January 2007). “Open-Label Phase II Study Evaluating the Efficacy and Safety of Two Doses of Pertuzumab in Castrate Chemotherapy-Naive Patients With Hormone-Refractory Prostate Cancer”. Journal of Clinical Oncology 25 (3): 257–262. doi:10.1200/JCO.2006.07.0888. PMID 17235043.
- “FDA Approves Perjeta (Pertuzumab) for People With HER2-Positive Metastatic Breast Cancer” (Press release). Genentech. Retrieved 2012-06-09.
- Genentech press release – May 15, 2005
- Keating GM. Pertuzumab: in the first-line treatment of HER2-positive metastatic breast cancer. Drugs 2012 Feb 12; 72 (3): 353-60.Link text
- Baselga J, Cortés J, Kim SB, and the CLEOPATRA Study Group. Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer. N Engl J Med 2012 Jan 12; 366 (2): 109-19. Link text
Phase 3 Boehringer Ingelheim Announces Interim Results Evaluating Virologic Response Rates in HCV/HIV Co-Infected Patients Treated with Faldaprevir

Faldaprevir
BI 201335
http://clinicaltrials.gov/ct2/show/NCT01343888
CAS Number: 801283-95-4
Molecular Formula: C40H49BrN6O9S
Molecular Weight: 869.82 g.mol
RIDGEFIELD, Conn., March 4, 2013
Boehringer Ingelheim Pharmaceuticals, Inc. announced the first interim results in HCV/HIV co-infected patients from the company’s ongoing hepatitis C (HCV) clinical trial program, HCVerso™. These results, from the Phase 3 trial STARTVerso™ 4, were presented today at the 20th annual Conference on Retroviruses and Opportunistic Infections (CROI) in Atlanta, GA.
The interim results showed that 80% of HCV/HIV co-infected patients achieved early treatment success (ETS)*, as defined by the study protocol, when given an investigational HCV regimen that included faldaprevir (BI 201335). Results were consistent across patients regardless of HIV therapy or prior HCV treatment status, including patients who were HCV treatment-naive or had previously relapsed during HCV treatment with pegylated interferon and ribavirin (PegIFN/RBV). Patients who achieved ETS were eligible for randomization to a shortened duration of treatment (24 weeks versus 48 weeks). Investigators also reported on-treatment virologic response at week 12, which showed that 84% of all study patients had undetectable levels of hepatitis C virus.
For more information, please visit http://us.boehringer-ingelheim.com

Faldaprevir, also known as BI 201335, is an investigational, oral protease inhibitor that is specifically designed to target viral replication in the liver. The ongoing multi-study Phase 3 STARTVerso™ trial program, evaluating faldaprevir combined with PegIFN/RBV in treatment-naive, treatment-experienced and HIV co-infected patients with chronic genotype-1 HCV, is near clinical completion. BI 207127 is an investigational NS5B non-nucleoside polymerase inhibitor that has shown the potential to eliminate interferon from HCV treatment when combined in a regimen with faldaprevir and RBV. Phase 2 trials of this interferon-free regimen have been completed and Phase 3 HCVerso™ trials investigating this regimen are now underway.
Faldaprevir and BI 207127 are investigational compounds and not approved by the FDA. Their safety and efficacy have not been established.
Hepatitis C is a blood-born infectious disease and a leading cause of chronic liver disease,transplant and failure that affects as many as 150 million people globally. In the United States, an estimated 4.1 million Americans have been infected with HCV, of which approximately 3.2 million have chronic HCV infection. Since 1999 there has been a significant increase in deaths due to chronic HCV, accounting for 15,000 deaths in the United States in 2007.
NDA –Sefelsa (gabapentin) Extended Release Tablets – formerly Serada

GABAPENTIN
Sefelsa (gabapentin) Extended Release Tablets – formerly Serada
Company: Depomed, Inc.
Treatment for: Menopausal Hot Flashes
Sefelsa (gabapentin) is an investigational extended-release formulation of gabapentin in development for the treatment of menopausal hot flashes.
- Depomed Provides Update on Sefelsa FDA Advisory Committee – March 4, 2013
- Depomed Announces Serada NDA Acceptance and FDA Advisory Committee Meeting – October 15, 2012
- Depomed Announces Submission Of Serada NDA – August 17, 2012
- Depomed Announces Intent to File NDA for Serada for Treatment of Menopausal Hot Flashes – April 18, 2012
NEWARK, Calif., March 4, 2013
Depomed, Inc., a specialty pharmaceutical company, announced today that the Reproductive Health Drugs Advisory Committee (RHDAC) of the U.S. Food and Drug Administration (FDA) voted 2-12 against approval for Sefelsa, Depomed’s investigational, oral, twice daily formulation of gabapentin, to treat moderate to severe vasomotor symptoms due to menopause. Sefelsa is the proposed trade name for the medication and was formerly referred to as Serada. Based on the outcome of committee meeting, the company will not have a conference call today as previously indicated.
“Depomed today is a product-focused, growth-oriented specialty pharmaceutical company with a growing franchise of treatments for pain and potentially other CNS indications. With revenues from two marketed products, Gralise and Zipsor, significant royalty income from our partnered products and technology, a strong balance sheet and potential to turn cash flow positive in the second half of this year, we believe that 2013 has the potential to be a landmark year in our company’s history,” said Jim Schoeneck, President and Chief Executive Officer of Depomed. “We recognize and appreciate the concerns that were raised by the members of the Advisory Committee. Based on today’s meeting we believe the hurdles for approval of a non-hormonal treatment for hot flashes remain high. Until we believe there is a positive direction for Sefelsa, we will cease all spending relating to the product candidate.”
Data presented at today’s Advisory Committee Meeting included results from the Phase 3 clinical program, which enrolled 1706 patients in three studies.
The FDA will consider the Advisory Committee recommendation in its review of the New Drug Application (NDA) for Sefelsa that Depomed submitted on July 31, 2012, though the FDA is not bound to follow it. The Prescription Drug User Fee Act (PDUFA) date for Sefelsa is May 31, 2013. The PDUFA date is the goal date for the FDA to complete its review of the NDA.
About Vasomotor Symptoms
Vasomotor symptoms include hot flashes and night sweats. A hot flash is a sudden flushing and sensation of heat caused by dilation of skin capillaries. Currently, the leading prescription drug product for the treatment of hot flashes associated with menopause is hormone replacement therapy (HRT). HRT involves the administration of the hormone estrogen, either alone or in combination with the hormone progestin.
About Depomed
Depomed, Inc. is a specialty pharmaceutical company with three approved and marketed products. Gralise® (gabapentin) is a once-daily treatment approved for the management of postherpetic neuralgia (PHN). Zipsor® (diclofenac potassium) Liquid Filled Capsules is a non-steroidal anti-inflammatory drug (NSAID) indicated for relief of mild to moderate acute pain in adults. Glumetza® (metformin hydrochloride extended release tablets) is approved for use in adults with type 2 diabetes and is commercialized by Santarus, Inc. in the United States. Depomed formulates its products and product candidates with its proven, proprietary Acuform® drug delivery technology, which is designed to improve existing oral medications, allowing for extended release of medications to the upper gastrointestinal tract when dosed with food. Additional information about Depomed may be found on its website, www.depomed.com.
Gabapentin (Neurontin) is a pharmaceutical drug, specifically a GABA analog. It was originally developed for the treatment of epilepsy, and currently is also used to relieve neuropathic pain. There are, however, concerns regarding the quality of the trials conducted for a number of conditions.[1]
Web Site: http://www.depomed.com
- Vedula, SS; Bero L; Scherer RW; Dickersin K (November 2009). “Outcome reporting in industry-sponsored trials of gabapentin for off-label use”. The New England Journal of Medicine 361 (20): 1963–71. doi:10.1056/NEJMsa0906126. PMID 19907043.
- “Gabapentin”. The American Society of Health-System Pharmacists. http://www.drugs.com/monograph/gabapentin.html. Retrieved 3 April 2011.
- Vedula, SS; Bero L; Scherer RW; Dickersin K (November 2009). “Outcome reporting in industry-sponsored trials of gabapentin for off-label use”. The New England Journal of Medicine 361 (20): 1963–71. doi:10.1056/NEJMsa0906126. PMID 19907043.
- Moore, RA; Wiffen PJ; Derry S; McQuay HJ (2011-03-16). Moore, R Andrew. ed. “Gabapentin for chronic neuropathic pain and fibromyalgia in adults”. Cochrane database of systematic reviews (Online) (3): CD007938. doi:10.1002/14651858.CD007938.pub2. PMID 21412914.
- Ho, KY; Gan TJ; Habib AS (2006-12-15). “Gabapentin and postoperative pain–a systematic review of randomized controlled trials”. Pain 126 (1–3): 91–101. doi:10.1016/j.pain.2006.06.018. PMID 16846695.

Phase3 Rindopepimut ,CDX-110 Celldex Therapeutics’ brain cancer vaccine

http://clinicaltrials.gov/ct2/show/NCT01480479
MAR 2013
Rindopepimut
Immunotherapeutic vaccine called Rindopepimut showed positive results in prolonging survival in patients with newly diagnosed EGFRvIII-positive glioblastoma (GB), one of the most aggressive forms of brain cancer
Celldex Therapeutics’ brain cancer vaccine, rindopepimut, also known as CDX-110, targets EGFRvIII, an activated mutation of the epidermal growth factor receptor (EGFR). This mutation is found in about 31% of cases of glioblastoma multiforme, a form of fast-growing brain cancer and the most common type of primary brain tumor. It can contribute to tumor growth, and is linked with poor long-term survival. It is not seen in normal tissue.
In the ACT III Phase II trial, which involved people with newly diagnosed EGFRvIII-positive glioblastoma, 65 patients were given rindopepimut in combination with standard-of-care treatment (temozolomide), after having undergone surgery and standard chemotherapy and radiation therapy.
focus on is Rindopepimut, an immunotherapy treatment that targets EGFRvIII. As it’s not found at significant levels in normal tissues but expressed in 30ish% of primary glioblastoma, it’s an ideal target that has produced promising results to date. The drug candidate has shown consistent benefit for patients across three phase 2 studies- that’s no fluke! It’s currently in a global phase 3 trial in patients with newly diagnosed glioblastoma with results due in a couple years
| Phase 3 Study of Rindopepimut in Patients With Newly Diagnosed Glioblastoma (ACT IV) | |
 |
|
| Design: | Phase 3, double-blind, study of rindopepimut compared with KLH control |
| Status: | Currently enrolling at multiple centers in the US; additional centers outside the US planned to be activated in 2012 |
ABOUT THE CLINICAL TRIAL
This 2-arm, randomized, Phase 3 study will investigate the efficacy and safety of the addition of rindopepimut to the current standard of care, temozolomide, in patients with recently diagnosed EGFRvIII positive glioblastoma. All patients will be administered temozolomide. Half the patients will be randomly assigned to receive rindopepimut (given along with GM-CSF as a vaccine adjuvant) and half the patients will be randomly assigned to receive a keyhole limpet hemocyanin (KLH). Patients will be treated in a blinded fashion (neither the patient nor the doctor will know which arm of the study the patient is on). Patients will be treated until disease progression or intolerance to therapy and all patients will be followed for survival.
All patients enrolled in the study will be closely monitored to determine if their cancer is responding to treatment and for any side effects that may occur.