
Home » Posts tagged 'organic chemistry' (Page 12)
Tag Archives: organic chemistry
 DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HERE
DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HEREFlag and hits
ORGANIC SPECTROSCOPY

SUBSCRIBE

 Subscribe in a reader
Subscribe in a reader
Enter your email address:
Delivered by FeedBurner
Subscribe to New Drug Approvals by Email![]()

![]()



![]()
![]()





Recent Comments
| shivkr2 on SPSR Excellence Award 2025 – S… | |
| Bonkasaurus on Infigratinib phosphate | |
| PALOVAROTENE | ORGAN… on Palovarotene | |
| Pfizer just purchase… on Temanogrel | |
| Pfizer To Cash In On… on Temanogrel |
NEW DRUG APPROVALS ACHIEVES ONE LAKH VIEWS IN 166 COUNTRIES

DR A .M. CRASTO
THIS BLOG NEW DRUG APPROVALS ACHIEVES ONE LAKH VIEWS IN 166 COUNTRIES …………….16 TH OCT 2013

Watermelon Juice Prevents Aching Muscles


L-citrulline
The amino acid L-citrulline found in the fruit could help athletes avoid muscle soreness after a hard workout
Before taking a long bike ride on a hot summer day, have some watermelon: The juicy fruit may ward off muscle pains. Researchers report that people who drank watermelon juice before exercising felt less sore the next day than those who drank a pink placebo beverage (J. Agric. Food Chem. 2013, DOI: 10.1021/jf400964r). They also found that cells absorb the presumed active ingredient, L-citrulline, more readily from unpasteurized watermelon juice than from plain water spiked with the compound, suggesting the natural source is the optimal delivery medium.
http://cen.acs.org/articles/91/web/2013/07/Watermelon-Juice-Prevents-Aching-Muscles.html

BioDelivery Sciences Announces FDA Acceptance of Bunavail NDA for Filing


buprenorphine

naloxone
RALEIGH, N.C., Oct. 9, 2013 /PRNewswire/ — BioDelivery Sciences International, Inc. announced today that its New Drug Application (NDA) for Bunavail (buprenorphine naloxone buccal film) for the maintenance treatment of opioid dependence has been accepted for filing by the U.S. Food and Drug Administration (FDA), indicating that the application is sufficiently complete to permit a substantive review. Based on timelines established by the Prescription Drug User Fee Act (PDUFA), the review of the Bunavail NDA is expected to be completed by early June 2014.
FDA Approves Sanofi’s Nasacort® Allergy 24HR for Over-the-Counter Use – Nasal Spray Treats Adults and Children with Seasonal and Year-Round Nasal Allergies
Nasacort
Paris, France, October 11, 2013 — Sanofi (EURONEXT: SAN and NYSE: SNY) announced today that the U.S. Food and Drug Administration (FDA) approved Nasacort® Allergy 24HR nasal spray as an over-the-counter (OTC) treatment for seasonal and year-round nasal allergies in adults and children 2 years of age and older. Nasacort is the first and only medicine in its class to be available without a prescription and will be marketed by Sanofi’s consumer healthcare division, Chattem, Inc.
read all at
http://www.pharmalive.com/fda-oks-otc-nasacort-allergy-24hr
Triamcinolone acetonide, USP, the active ingredient in NASACORT AQ Nasal Spray, is a corticosteroid with a molecular weight of 434.51 and with the chemical designation 9-Fluoro11β,16α,17,21-tetrahydroxypregna-1,4-diene-3,20-dione cyclic 16,17-acetal with acetone (C24H31FO6).
 |
NASACORT AQ Nasal Spray is a thixotropic, water-based metered-dose pump spray formulation unit containing a microcrystalline suspension of triamcinolone acetonide in an aqueous medium. Microcrystalline cellulose, carboxymethylcellulose sodium, polysorbate 80, dextrose, benzalkonium chloride, and edetate disodium are contained in this aqueous medium; hydrochloric acid or sodium hydroxide may be added to adjust the pH to a target of 5.0 within a range of 4.5 and 6.0.
Unani medicine
Unani-tibb or Unani Medicine also spelled Yunani Medicine (/juːˈnɑːni/; Yūnānī in Arabic, Hindustani, pashto and Persian) is a form oftraditional medicine widely practiced by Muslims. It refers to a tradition of Graeco-Arabic medicine, which is based on the teachings of Greek physician Hippocrates, and Roman physician Galen, and developed into an elaborate medical System by Arab and Persian physicians, such asRhazes (al-Razi), Avicenna (Ibn Sena), Al-Zahrawi, and Ibn Nafis.
Unani medicine is based on the concept of the four humours: Phlegm (Balgham), Blood (Dam), Yellow bile (Ṣafrā’) and Black bile (Saudā’).
The word Unani or Yunani has its origins in the Greek word Ἰωνία (Iōnía) or Ἰωνίη (Iōníe), a place name given to a Greek populated coastal region of Ionian Sea.
History of Unani Medicine

The Origin of Unani system of medicine Is from Greece. The term ‘UNANI’ is derived from the word ‘UNAN’ or “YUNAN” which means Greece in Arabic Its also know as Greco-Arab medicine. the treatment of Unani is based on teachings of Hippocrates It was the work of the Greek philosopher-physician Hippocrates {Buqrat In Arabic} (460-377 B.C.), who freed medicine from the realm of superstition and magic and gave it the status of science. He considered illness to be natural rather than a supernatural phenomenon, and he felt that medicine should be administered without ritual ceremonies or magic.By his method of careful study and comparison of symptoms, he laid the foundation for clinical medicine.
Hippocrates
After Hippocrates Many scholars enriched the system of Unani Medicine. Of them Galen {Jalinus in Arabic} (131-200 A.D.) stands out as the one who established its foundation on which Arab physicians like Rhazes {Al-Razi in Arabic} (850-932 A.D.) and Avicenna {Ibn-Sena in Arabic} (980-1037 A.D.) constructed an imposing edifice. Galen introduced and practiced the Unani system of medicine in pre-Islamic Egypt, researched, experimented and developed hundreds of new medicines and cures for almost all types of diseases.
 Unani medicine was the first to establish that disease was a natural process and that symptoms were the reactions of the body to the disease. It believes in the humeral theory which presupposes the presence of the four humors – Dam (blood), Balgham(phlegm), Safra (yellow bile) and Sauda (black bile) in the body. Each humor has its own temperament – blood is hot and moist, phlegm cold and moist, yellow bile hot and dry and black bile cold and dry. Every person attains a temperament according to the preponderance in them of the humors which represent the person’s healthy state, which are expressed as sanguine, phlegmatic, choleric and melancholic.
Unani medicine was the first to establish that disease was a natural process and that symptoms were the reactions of the body to the disease. It believes in the humeral theory which presupposes the presence of the four humors – Dam (blood), Balgham(phlegm), Safra (yellow bile) and Sauda (black bile) in the body. Each humor has its own temperament – blood is hot and moist, phlegm cold and moist, yellow bile hot and dry and black bile cold and dry. Every person attains a temperament according to the preponderance in them of the humors which represent the person’s healthy state, which are expressed as sanguine, phlegmatic, choleric and melancholic.
It was further enriched by imbibing the best of contemporary systems of medicine in the middle eastern and far eastern countries like Egypt, Syria, Iraq, Persia, India, China and other Middle East and Far East countries enriched the Unani system. That is why this system is known, in different parts of the world, with different names such as Greco-Arab Medicine, Ionian Medicine, Arab Medicine, Islamic Medicine, Traditional Medicine, Oriental Medicine, etc.
A Unani physician does not prescribe the strongest drug at the beginning of the treatment. He selects the drug according to the degree of variation from the normal healthy condition and observes the effect produced by the treatment. At the same time, he instructs the patient to observe some restrictions in diet and lifestyle.“Besides the use of herbs for treatment, Unani medicine employs a variety of other techniques intended to cleanse the body and restore humor balance. These techniques include: mushil (purging), taareeq (sweating), hammam (bath therapy), munzij (ripening), mahajim (cupping) and riyazat (exercise).
Though the threads which comprise Unani healing can be traced all the way back to Ancient Iranian Medicine, the basic knowledge of Unani medicine as a healing system was developed by Muslim scholar Hakim Ibn Sina (known as Avicenna in the west) in his medical encyclopedia The Canon of Medicine. The time of origin is thus dated at circa 1025 AD, when Avicenna wrote The Canon of Medicine in Persia. While he was primarily influenced by Greek and Islamic medicine, he was also influenced by the Indian medical teachings of Sushruta and Charaka.
Unani medicine first arrived in India around 12th or 13th century with establishment of Delhi Sultanate (1206-1527) and Islamic rule over North India and subsequently flourished under Mughal Empire. Alauddin Khilji (r. 1296-1316) had several eminent Unani physicians (Hakims) in his royal courts In the coming year this royal patronage meant development of Unani practice in India, but also of Unani literature with the aid of Indian Ayurvedic physicians.
Diagnosis and treatment
Fortunately, Unani classical literature consists of thousands of books and contains vast knowledge and mention of experiences on all aspects of medicine. According to Unani medicine, management of any disease depends upon the diagnosis of disease. In the diagnosis, clinical features, i.e., signs, symptoms, laboratory features and mizaj (temperament) are important.
Any cause and or factor is countered by Quwwat-e-Mudabbira-e-Badan (the power of body responsible to maintain health), the failing of which may lead to quantitatively or qualitatively derangement of the normal equilibrium of akhlat (humors) of body which constitute the tissues and organs. This abnormal humor leads to pathological changes in the tissues anatomically and physiologically at the affected site and exhibits the clinical manifestations.
After diagnosing the disease, Usoole Ilaj (principle of management) of disease is determined on the basis of etiology in the following pattern:
- Izalae Sabab (elimination of cause)
- Tadeele Akhlat (normalization of humors)
- Tadeele Aza (normalization of tissues/organs)
For fulfillment of requirements of principle of management, treatment is decided as per the Unani medicine which may be one or more of the following:
- Ilaj-Bil-Tadbeer wa Ilaj-Bil-Ghiza (Regimenal Therapy). The disease may be treated by the modification of six essential pre-requisites of health (Asbab-e-Sitta Zarooriya in Unani Tibbi terminology). Asbab-e-Sitta Zarooriya may be modified by the use of one or more regimens: i.e., Dalak, Riyazat, Hammam, Taleeq, Takmeed, Hijamat (Cupping Therapy), Fasd, Lakhlakha, Bakhur, Abzan, Shamoomat (Aromatherapy), Pashoya, Idrar, Ishal, Qai, Tareeq, Elam, Laza-e-Muqabil, Imalah and alteration of food. According to the norms of C.C.I.M. New Delhi, Department of Ilaj-Bil-Tadbeer has been established in almost all Unani Tibbi Colleges of India. In the State Unani Medical College, Allahabad, U.P. and State Takmeel-Ul-Tibb College, Lucknow, Department of Ilaj-Bil-Tadbeer is known as Moalijat Khususi. Moaliajt Khususi is the old nomenclature of Ilaj-Bil-Tadbeer, suggested by C.C.I.M. New Delhi. Ilaj-Bil-Tadbeer is synonym to Panchkarma in Ayurveda.
- Ilaj-Bil-Advia (Pharmacotherapy). For this purpose Mamulate Matab Nuskha (prescription) is formulated which contain the single and or compound (murakkābāt) Unani drugs[12] having desired actions as per requirements.
- Ilaj-Bil-Yad (Surgery)
As an alternative form of medicine, Unani has found favor in India where popular products like Roghan Baiza Murgh (Egg Oil) and Roghan Badaam Shirin (Almond Oil) are commonly used for hair care. Unani practitioners can practice as qualified doctors in India, as the government approve their practice. Unani medicine is very close to Ayurveda. Both are based on theory of the presence of the elements (in Unani, they are considered to be fire, water, earth and air) in the human body. (The elements, attributed to the philosopher Empedocles, determined the way of thinking in Medieval Europe.) According to followers of Unani medicine, these elements are present in different fluids and their balance leads to health and their imbalance leads to illness.
The theory postulates the presence of blood, phlegm, yellow bile and black bile in the human body. Each person’s unique mixture of these substances determines his Mizaj(Temperament). a predominance of blood gives a sanguine temperament; a predominance of phlegm makes one phlegmatic; yellow bile, bilious (or choleric); and black bile, melancholic.
Education and recognition
In India, there are 40 Unani medical colleges where the Unani system of medicine is taught. After five and half year courses, the graduates are awarded BUMS (Bachelor of Unani Medicine and Surgery). There are about eight Unani medical colleges where a postgraduate degree (Mahir-e-Tib and Mahir Jarahat) is being awarded to BUMS doctors. All these colleges are affiliated to reputed universities and recognized by the governments.
In India, the Central Council of Indian Medicine (CCIM) a statutory body established in 1971 under Department of Ayurveda, Yoga and Naturopathy, Unani, Siddha and Homoeopathy (AYUSH), Ministry of Health and Family Welfare, Government of India, monitors higher education in areas of Indian medicine including, Ayurveda, Unani and Siddha. To fight biopiracy and unethical patents, the Government of India, in 2001, set up the Traditional Knowledge Digital Library as repository of formulations of systems of Indian medicine, includes 98,700 Unani formulations.[14][15] Central Council for Research in Unani Medicine (CCRUM) established in 1979, also under AYUSH, aids and co-ordinates scientific research in the Unani system of medicine through a network of 22 nationwide research institutes and units, including two Central Research Institutes of Unani Medicine, at Hyderabad and Lucknow, eight Regional Research Institutes at Chennai, Bhadrak, Patna, Aligarh, Mumbai, Srinagar, Kolkata and New Delhi, six Clinical Research Units at Allahabad, Bangalore, Karimganj, Meerut, Bhopal and Burhanpur, four Drug Standardisation Research Units at New Delhi, Bangalore, Chennai and Lucknow, a Chemical Research Unit at Aligarh, a Literary Research Institute at New Delhi.
Safety issues
According to WHO, “Pharmacovigilance activities are done to monitor detection, assessment, understanding and prevention of any obnoxious adverse reactions to drugs at therapeutic concentration that is used or is intended to be used to modify or explore physiological system or pathological states for the benefit of recipient.” These drugs may be any substance or product including herbs, minerals, etc. for animals and human beings and can even be that prescribed by practitioners of Unani or ayurvedic system of medicine. In recent days, awareness has been created related to safety and adverse drug reaction monitoring of herbal drugs including Unani drugs.
Notable Unani Organizations/institutions
- GOVERNMENT UNANI MEDICAL COLLEGE,CHENNAI, TAMILNADU
JAMIA TIBBIYA DEOBAND (B.U.M.S. & M.D.)
- SHAMIM AHMAD SAEEDI UNANI HOSPITAL FOR JOINTS PAIN
- JAMIA REMEDIES (UNANI DRUGS MANUFACTURING COMPANY, INDIA)
- Baqai Dawakhana pvt ltd,Delhi India
- Awami Laboratories, Lahore, Pakistan
- Hamdard University, Karachi, Pakistan
- Farzana Dawakhana, Karachi, Pakistan
- Central Council for Research in Unani Medicine,India.
- Ajmal Khan Tibbia College, Aligarh Muslim University, Aligarh,U.P.India.
- Ibn Sina Academy of Medieval Medicine and Sciences,India.
- National Institute of Unani Medicine, (Government of India)
- A&U Tibbia College, Karol Bagh, New Delhi, (Government of N.C.T. Delhi),India.
- Faculty of Unani Medicine, Jamia Hamdard, New Delhi,India.
- Government Nizamia Tibbi College and Hospital, Hyderabad, A.P.India.
- Anjuman-i- Islam’s Tibbia College and Hospital, Mumbai, Maharashtra, India.
- ZVM Unani College and Hospital, Pune, M.S.India.
- State Takmeel-ut-tib College and hospital, Lucknow, U.P.(Government of U.P.).India.
- State Unani Medical College & H.A.H.R.D.M. Hospital, Himmatganj, Allahabad, U.P. (Government of U.P.).India.
- Saifia Hamidia Unani Tibbia College & Saeeda Hospital, Ganpati Naka, Burhanpur,M.P.India.
- Tipu Sultan Unani Medical College,Gulbarga, Karnataka.
- Govt. Unani and Ayurvedic Medical College & Hospital, Dhaka, Bangladesh
- Markaz Unani Medical College & Hospital, Calicut, India
- The Institute of Indigenous Medicine, University of Colombo, Sri Lanka
- Government Unani Medical College, Bashaveshwara Nagar, Bangalore-560079
- Mohsin-e-millat Unani Medical College and Hospital (Baijnathpara Raipur,chhattisgarh India)
- HSZH Govt. Unani medical college Bhopal-462003
- Ahmed Garib Unani Medical College Akkalkuwa Nandurbar M.S India
- All India Unani Tibbi Conference, New Delhi.
- Awami Dawakhana Unani,Hyderabad,India.
- Govt.Nizamia Tibbi College, Hyderabad,India.
Tasquinimod for patients with metastatic castrate-resistant prostate cancer (mCRPC) who have not yet received chemotherapy

Tasquinimod
Tasquinimod (ABR-215050, CID 54682876) is a novel, oral drug currently being investigated for the treatment of solid tumors. Tasquinimod has been mostly studied in prostate cancer, but its mechanism of action suggests that it could be used to treat other cancers. Castration-resistant prostate cancer (CRPC), formerly called hormone-resistant or hormone-refractory prostate cancer, is prostate cancer that grows despite medical or surgical androgen deprivation therapy. Tasquinimod targets the tumor microenvironment and counteracts cancer development by inhibiting angiogenesis and metastasis and by modulating the immune system. It is now in phase III development, following successful phase II trial outcomes.
Collaborative studies by laboratories at The Johns Hopkins University School of Medicine, Baltimore, Maryland, USA, and Active Biotech Research AB, Lund, Sweden, identified tasquinimod as the lead agent for developing a treatment for prostate cancer.Tasquinimod was one of several second-generation quinoline-3-carboxamide variants synthesized using the drug roquinimex as a starting point, and it performed well in pre-clinical studies of cancer models
Tasquinimod is a novel small molecule that targets the tumor microenvironment by binding to S100A9 and modulating regulatory myeloid cell functions, exerting immunomodulatory, anti-angiogenic and anti-metastatic properties. Tasquinimod may also suppress the tumor hypoxic response, contributing to its effect on the tumor microenvironment. Today the development of tasquinimod is principally focused on the treatment of prostate cancer, but clinical studies in other cancer indications are performed. The ongoing 10TASQ10 trial is a randomized, double-blind, placebo-controlled, global Phase III clinical trial evaluating tasquinimod in patients with metastatic castrate-resistant prostate cancer (mCRPC) who have not yet received chemotherapy.
The aim of the 10TASQ10 study is to confirm tasquinimod’s efficacy, with radiological Progression Free Survival (rPFS) as primary endpoint and overall survival (OS) as key secondary endpoint. The Phase III 10TASQ10 trial met its enrollment target in December 2012 with 1,245 randomized patients as planned in the clinical protocol. The study recruited patients in 37 countries covering more than 200 centers. Active Biotech and Ipsen plan to conduct the primary PFS analysis for the 10TASQ10 trial in 2014, at the same time as the first interim overall survival (OS) analysis.
About Active Biotech
Active Biotech AB (nasdaq omx nordic:ACTI) is a biotechnology company with focus on autoimmune/inflammatory diseases and cancer. Projects in pivotal phase are laquinimod, an orally administered small molecule with unique immunomodulatory properties for the treatment of multiple sclerosis, tasquinimod for prostate cancer and ANYARA primarily for the treatment of renal cell cancer. In addition, laquinimod is also in Phase II development for Crohn’s and Lupus. The company also has one additional project in clinical development, the orally administered compound paquinimod (57-57) for systemic sclerosis. Please visit http://www.activebiotech.com for more information.
About Ipsen
Ipsen is a global specialty-driven pharmaceutical company with total sales exceeding EUR1.2 billion in 2012. Ipsen’s ambition is to become a leader in specialty healthcare solutions for targeted debilitating diseases. Its development strategy is supported by 3 franchises: neurology, endocrinology and uro-oncology. Moreover, the Group has an active policy of partnerships. Ipsen’s R&D is focused on its innovative and differentiated technological platforms, peptides and toxins. In 2012, R&D expenditure totaled close to EUR250 million, representing more than 20% of Group sales. The Group has close to 4,900 employees worldwide. Ipsen’s shares are traded on segment A of Euronext Paris (stock code:IPN)(isin code:FR0010259150) and eligible to the “Service de Reglement Differe” (“SRD”). The Group is part of the SBF 120 index. Ipsen has implemented a Sponsored Level I American Depositary Receipt (ADR) program, which trade on the over-the-counter market in the United States under the symbol IPSEY. For more information on Ipsen, visit http://www.ipsen.com.

In 2011, Active Biotech and Ipsen entered into a broad partnership for the co-development and commercialization of tasquinimod. Under the terms of the agreement, Active Biotech has granted Ipsen exclusive rights to commercialize tasquinimod worldwide, except for North and South America and Japan, where Active Biotech has retained all commercial and marketing rights. Both companies co-develop tasquinimod for the treatment of metastatic castrate-resistant prostate cancer (mCRPC) and Ipsen is developing tasquinimod also in other cancer indications. Active Biotech is responsible for conducting and funding the Phase III 10TASQ10 pivotal clinical trial and will receive up to EUR 200M (whereof EUR 25M upfront and EUR 32M in milestones have been received so far) upon achievement of clinical, regulatory and commercial milestones. In addition, Ipsen will pay Active Biotech tiered double-digit royalties on all sales of TASQ in Ipsen’s territories
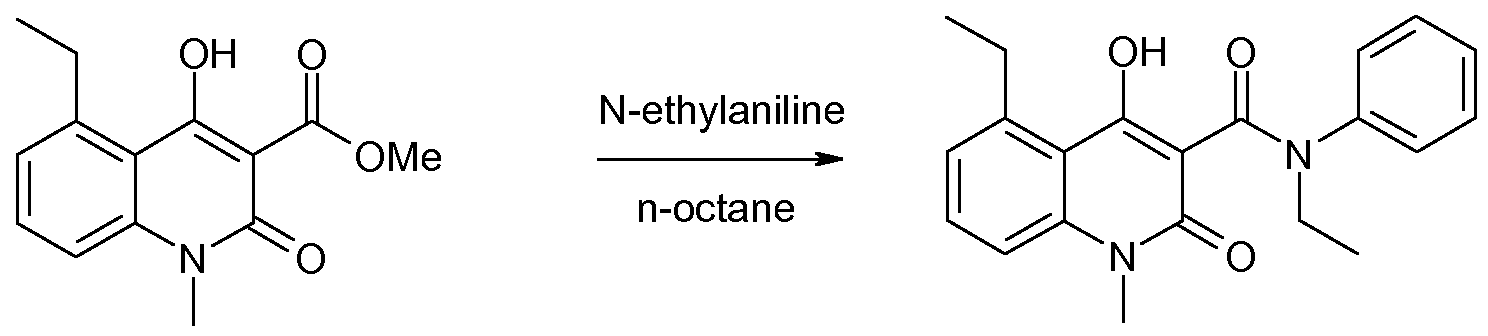
N-alkyl-N-phenyl-quinoline-3-carboxamides such as paquinimod (herein below also referred to as A), laquinimod (herein below also referred to as B), andtasquinimod (herein below also referred to as C), have been prepared by a method involving distillation of the volatiles from a mixture comprising an ester, aniline and an aliphatic solvent such as n-heptane or n-octane.

Paquinimod (A) Laquinimod (B) Tasquinimod (C)
This method is described in US patent No. 6,875,869.
The prior art synthetic protocol (Org. Process. Res&Dev. 2007, 11, 674-680) for N-alkyl-N- phenyl-quinoline-3-carboxamides such as paquinimod (A), laquinimod (B), and tasquinimod (C) is exemplified with synthesis of paquinimod in Scheme 1. The route starts with an an- thranilic acid 1 which is transformed into an isatoic anhydride 2. The isatoic anhydride is methylated to give 3, which is condensed with dimethylmalonate to give the corresponding methyl ester 4. The methyl ester is subsequently condensed with the appropriate aniline, to give the desired final compound.

Scheme 1. The synthetic route to N-alkyl-N-phenyl-quinoline-3-carboxamides, exemplified with the synthesis of paquinimod (A) via the corresponding methyl ester 4.
This manufacturing method is short and avoids the use of expensive reagents. All intermediates are stable and easy to isolate in high purity by precipitation and filtration. The main impurity in the final condensation step is remaining alkyl ester. Alternative methods, such as carbodiimide mediated coupling between a carboxylic acid and aniline, or the condensation of N-alkyl-N-phenyl-malonamic acid methyl ester with an isatoic anhydride (US patent No. 5,912,349) are either longer or yield product of lower purity.
The final condensation step is an equilibrium (Scheme 2) that favors the alkyl ester and a action mechanism involving a ketene intermediate 5 has been strongly indicated (J. Org. Chem. 2006, 71, 1658-1667 and J Phys. Chem. A 2008, 112, 4501-4510).
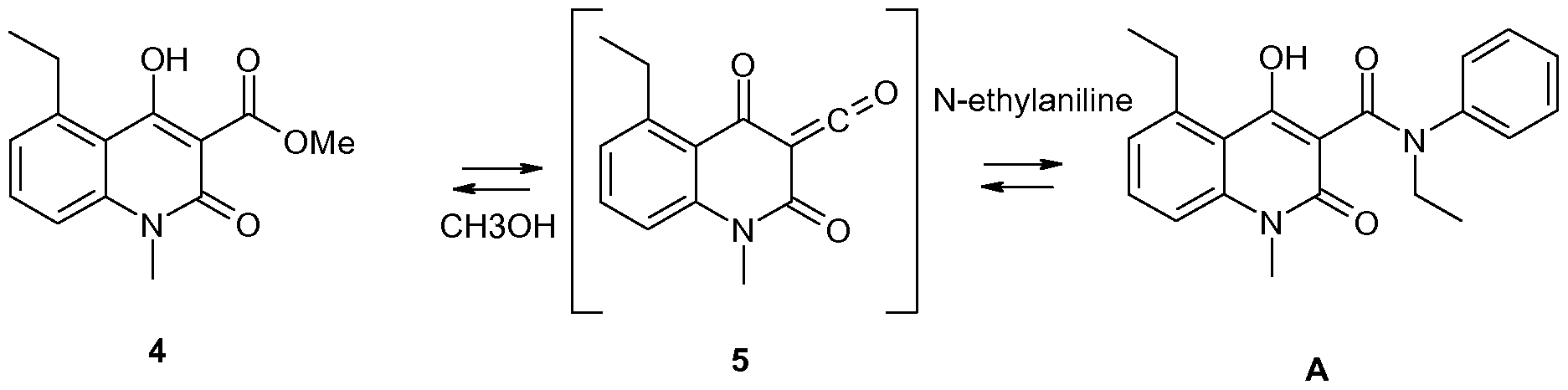
Scheme 2. An intermediate ketene 5 is involved in the equilibrium between 4 and A. Usually formation of amides from esters and anilines requires very high reaction temperatures that also cause extensive byproduct formation. The above-mentioned reaction is enabled at moderate temperatures by the ability of 4 to unimolecularly form the ketene intermediate 5 instead of a tetrahedral intermediate. The method, which is described e.g. in US patent No. 6,875,869, comprises charging the reactor with an appropriate ester and an aniline derivative in an aliphatic solvent such as n-heptane or n-octane.
The equilibrium is driven towards the desired product by distilling off the solvent and any formed alcohol. After complete reaction the mixture is cooled and the precipitated raw product is isolated by filtration. Unlike most other reactions where esters are transformed into thermodynamically more stable amides this particular reaction needs a very efficient removal of formed alcohol in order to give a high yield.
VERCIRNON – GSK1605786A (formerly CCX282-B) Anti-inflammatory intended to treat Crohn’s disease and inflammatory bowel disease
http://www.ama-assn.org/resources/doc/usan/vercirnon.pdf
|
vercirnon
|
|
| Trade Name: | Traficet-EN |
| Synonym: | CCX282-B, GSK1605786, GSK 1605786 |
- C22H21ClN2O4S
- Average mass: 444.931091
4-(2-(4-(tert-butyl)phenylsulfonamido)-5-chlorobenzoyl)pyridine 1-oxide
698394-73-9 [RN]
Anti-inflammatory intended to treat Crohn’s
disease and inflammatory bowel disease
GSK1605786A (formerly CCX282-B) targets chemokine receptor CCR9, which is expressed selectively on intestinal lymphocytes and dendritic cells. CCR9 mediates migration of immune cells to the intestine, and blockade of the receptor inhibits migration.
GSK1605786A is being studied in CD at a dose of 500 mg by mouth once daily or 500 mg by mouth twice daily versus placebo. Final data is anticipated to be collected mid-2012 for a study evaluating efficacy over a 12-week treatment period.
A study reviewing maintenance of remission is expected to be complete in July 2014 and a long-term safety study is scheduled for completion in July 2015.
GSK-1605786 (CCX-282; Traficet-EN), a selective antagonist of the CC chemokine receptor (CCR9), is being developed by GlaxoSmithKline plc under license from ChemoCentryx Inc for the potential treatment of inflammatory bowel disease, including Crohn’s disease and celiac disease. CCR9 is a tissue-specific lymphocyte trafficking molecule that selectively attracts both B- and T-cells to the small gut. Inhibition of CCR9 by GSK-1605786 may inhibit B- and T-cell entry to the small gut and ameliorate inflammation while leaving immune function at other anatomical sites unaffected. GSK-1605786 was assessed as a treatment for moderate-to-severe Crohn’s disease in the phase II/III PROTECT-1 trial and as a treatment for celiac disease in a phase II trial. Data suggest that GSK-1605786 is efficacious in patients with Crohn’s disease with the advantage of being orally bioavailable.

GT Biologics obtains FDA orphan drug designation for paediatric Crohn’s drug
GT Biologics, a developer of live biotherapeutics for the treatment of autoimmune diseases, has received orphan drug designation from the US Food and Drug Administration (FDA) for its lead product candidate, Thetanix.
read all at
read all on
Bacteroides thetaiotaomicron
http://microbewiki.kenyon.edu/index.php/Bacteroides_thetaiotaomicron
Chelsea Therapeutics Announces FDA Advisory Committee to Review Northera(Droxidropa, 23651-95-8)

droxidropa
CHARLOTTE, N.C., Oct. 9, 2013 (GLOBE NEWSWIRE) — Chelsea Therapeutics International, Ltd. today announced that the U.S. Food and Drug Administration (FDA) has notified the Company that the New Drug Application (NDA) seeking approval to market Northera (droxidopa), an orally active synthetic precursor of norepinephrine, for the treatment of symptomatic neurogenic orthostatic hypotension (NOH) will be reviewed by the Cardiovascular and Renal Drug Advisory Committee (CRDAC). The meeting is tentatively scheduled for January 14, 2014 read more here————
http://www.drugs.com/nda/northera_131009.html
old article cut paste
FDA Deems Resubmission a Complete Response; PDUFA Date Set as
February 14, 2014
CHARLOTTE, N.C., Sept. 4, 2013 (GLOBE NEWSWIRE) — Chelsea Therapeutics International, Ltd. (Nasdaq:CHTP) today announced that the U.S. Food and Drug Administration (FDA) has acknowledged receipt of the New Drug Application (NDA) resubmission seeking approval to market NORTHERA(TM) (droxidopa), an orally active synthetic precursor of norepinephrine
read all at
http://www.pharmalive.com/chelsea-therapeutics-announces-fda-acceptance-of-northera-nda-resubmission
L-DOPS (L-threo-dihydroxyphenylserine; Droxidopa; SM-5688) is a psychoactive drug and synthetic amino acid precursor which acts as a prodrug to the neurotransmitters norepinephrine (noradrenaline) and epinephrine (adrenaline).[1] Unlike norepinephrine and epinephrine themselves, L-DOPS is capable of crossing the protective blood–brain barrier (BBB).[1]
Neurogenic orthostatic hypotension (NOH),[2] as well as NOH associated with multiple system atrophy (MSA), familial amyloid polyneuropathy (FAP), pure autonomic failure (PAF), and Parkinson’s disease (PD).
Intradialytic hypotension (IDH) or hemodialysis-induced hypotension.
Hypotension associated with fibromyalgia syndrome (FMS) and chronic fatigue syndrome (CFS).[3]
History
L-DOPS was developed by Sumitomo Pharmaceuticals under the trade name Droxidopa for the treatment of hypotension, including NOH,[2] and NOH associated with various disorders such as MSA, FAP, and PD, as well as IDH. The drug has been used in Japan and some surrounding Asian areas for these indications since 1989. Following a merge with Dainippon Pharmaceuticals in 2006, Dainippon Sumitomo Pharma licensed L-DOPS to Chelsea Therapeutics to develop and market it worldwide except in Japan, Korea, China, and Taiwan.
Clinical trials
Though L-DOPS has been used in Japan and Southeast Asia already for some time, it is also currently in clinical trials at the phase III point in the United States (U.S.), Canada, Australia, and throughout Europe. Provided L-DOPS successfully completes clinical trials, it could be approved for the treatment of NOH as early as 2011.[4] Additionally, phase II clinical trials for IDH are also underway. Chelsea Therapeutics obtained orphan drug status (ODS) for L-DOPS in the U.S. for NOH, and that of which associated with PD, PAF, and MSA, and is the pharmaceutical company developing it in that country.
- Goldstein, DS (2006). “L-Dihydroxyphenylserine (L-DOPS): a norepinephrine prodrug”. Cardiovasc Drug Rev 24 (3-4): 189–203. doi:10.1111/j.1527-3466.2006.00189.x. PMID 17214596.
- Mathias, Christopher J (2008). “L-dihydroxyphenylserine (Droxidopa) in the treatment of orthostatic hypotension”. Clin Auton Res 18 (Supplement 1): 25–29.doi:10.1007/s10286-007-1005-z.
- Crofford, LJ (2008). “Pain management in fibromyalgia”. Curr Opin Rheumatol 20 (3): 246–250. doi:10.1097/BOR.0b013e3282fb0268. PMID 18388513.
- Search of: “Droxidopa” – List Results – ClinicalTrials.gov
- Robertson, David (2008). “The pathophysiology and diagnosis of orthostatic hypotension”. Clin Auton Res 18 (Supplement 1): 2–7. doi:10.1007/s10286-007-1004-0.
