
Home » Posts tagged 'health'
Tag Archives: health
 DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HERE
DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HEREFlag and hits
ORGANIC SPECTROSCOPY

SUBSCRIBE

 Subscribe in a reader
Subscribe in a reader
Enter your email address:
Delivered by FeedBurner
Subscribe to New Drug Approvals by Email![]()

![]()



![]()
![]()





Recent Comments
| shivkr2 on SPSR Excellence Award 2025 – S… | |
| Bonkasaurus on Infigratinib phosphate | |
| PALOVAROTENE | ORGAN… on Palovarotene | |
| Pfizer just purchase… on Temanogrel | |
| Pfizer To Cash In On… on Temanogrel |
Tisolagiline


Tisolagiline
CAS 1894207-44-3
PCH79KLX33
(2S)-2-[[4-[4-(trifluoromethyl)phenyl]phenyl]methylamino]propanamide
322.32 g/mol
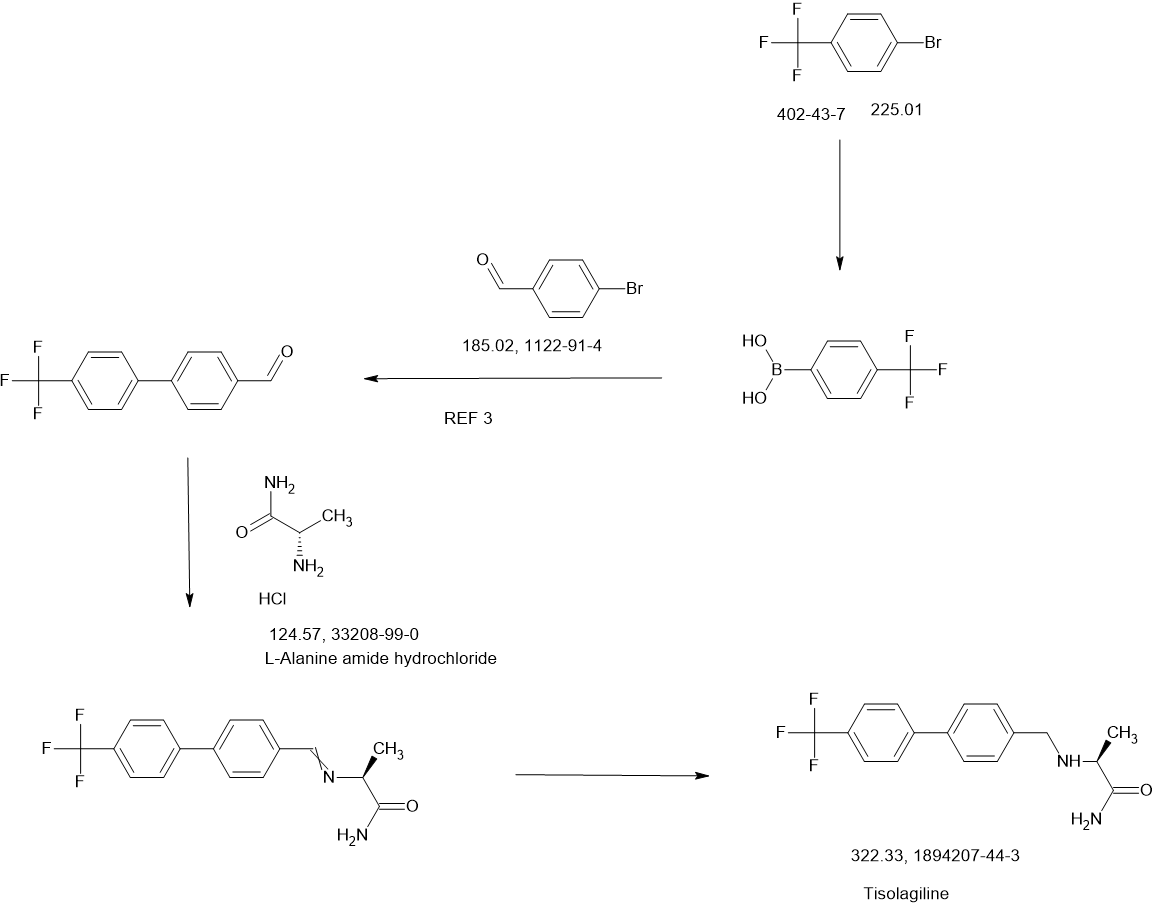
SCHEME
Tisolagiline (INNTooltip International Nonproprietary Name; developmental code names KDS-2010, SeReMABI) is a potent, highly selective, and reversible monoamine oxidase B (MAO-B) inhibitor which is under development for the treatment of Alzheimer’s disease and obesity.[1][2][3][4] It is taken by mouth.[1] Tisolagiline is being developed by NEUROBiOGEN and Scilex Bio.[1][2] As of December 2024, it is in phase 2 clinical trials for Alzheimer’s disease and obesity.[1][2]
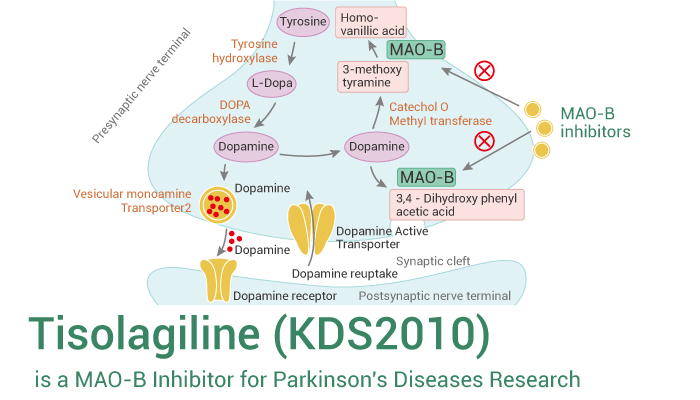
Parkinson’s disease is a progressive disease that ranks second among degenerative neurological diseases, and the incidence rate is estimated to be about 6.3 million patients worldwide, and about 1 in 1,000 people develop Parkinson’s disease. The incidence rate is usually higher in the elderly, but it is now developing in young people as well. Parkinson’s disease is not easy to distinguish from other diseases because the symptoms progress slowly, and it is difficult to detect in the early stages. Clinical characteristics include tremors, rigidity, bradykinesia, postural instability, stooped posture, freezing of gait, depression, sleep disorders, urination disorders, and dementia.
[3]Parkinson’s disease has an unknown cause, but it is known to be a disease that occurs when nerve cells that secrete the neurotransmitter dopamine in the brain are destroyed, resulting in a lack of dopamine. The most widely developed and used drug is levodopa therapy, which is generally administered by administering levodopa, which is converted into dopamine in the body. Levodopa is the most effective treatment for Parkinson’s disease, but there are cases where the drug-related effects decrease or various movement disorders occur during the treatment process. Other drugs used include COMT inhibitors and MAO-B inhibitors, which suppress dopamine metabolism and maintain the concentration of dopamine in the brain.
[4]MAO-B is known to play an important role in dopamine metabolism in the brain and to suppress damage to brain neurons. Although there is no clear evidence that MAO-B inhibitors actually slow down the progression of Parkinson’s disease, it is known that inhibiting MAO-B has an effect of suppressing degeneration or death of dopamine neurons, as it plays an important role in the development of Parkinson’s disease caused by MPTP or similar environmental toxicants. In addition, evidence from animal and clinical trials suggests that MAO-B inhibitors have a brain protective effect, unlike other drugs.
[5]The most representative MAO-B inhibitor approved is selegiline, which is prescribed as a treatment for Parkinson’s disease, but when taken, it is metabolized into amphetamine in the body, causing liver toxicity, and as an irreversible inhibitor, it has various side effects. Azilect, which contains rasagiline, was first marketed in Israel in 2005 and has recently been released in about 50 countries including Europe and the United States. Azilect does not have amphetamine side effects in the body when taken and is said to be more effective than other dopaminergic drugs. However, rasagiline, like selegiline, is an irreversible MAO-B inhibitor, so although it has an excellent MAO-B inhibition effect, it has the disadvantage of safety issues. Therefore, recently, drugs that are effective and can reversibly inhibit activity are being developed as alternatives to complement these shortcomings, but no notable reversible inhibitors have been prescribed to date.
[6]Meanwhile, obesity is a medical condition in which excessive fat accumulates in the body to the extent that it has a negative impact on health. Excessive weight can appear in combination with various diseases as the remaining energy is accumulated excessively due to the difference between energy consumed and energy used.
[7]Previous studies on the hypothalamus in relation to food regulation have focused on neurons that make up a portion of the brain, which has limited our understanding of the brain’s function in controlling food and obesity. Therefore, in order to comprehensively understand brain function, studies on glial cells, which make up the majority, must also be conducted in parallel. In addition, astrocytes, which are the most numerous among glial cells, have recently emerged as cells that can activate or inhibit surrounding neurons by secreting various signaling substances such as GABA (gamma-aminobutyric acid), glutamate, D-serine, and ATP. Astrocytes in the hypothalamus also interact closely with POMC (pro-opiomelanocortin) neurons and express leptin receptors, which can contribute to leptin signaling.
[8]There are two groups of POMC neurons in the hypothalamus: those that induce appetite reduction and those that induce energy consumption. Under normal circumstances, astrocytes help activate nearby POMC neurons that induce energy consumption. However, in obese states, unlike normal astrocytes, they are transformed into reactive astrocytes due to excessive leptin signals, and putrescine is converted into GABA by MAO-B (mono-aminoxidase B) and secreted. In addition, POMC neurons that induce energy consumption express GABAa receptors outside the synapse containing a4, a5, and a6 subunits due to excessive leptin signals, and are affected by persistent GABA secreted from anti-responsive astrocytes. As a result, POMC neurons are inhibited, energy consumption is reduced, and fat accumulation occurs.
[9]At this time, if MAOBI, the causal enzyme of GABA production, is inhibited, GABA production and secretion are inhibited, the inhibition of POMC neurons is relieved, and they are reactivated to promote energy consumption. However, POMC neurons that induce appetite reduction do not express GABAa receptors outside the synapse, so they are not continuously affected by GABA. Therefore, MAOBI inhibitors selectively act on POMC neurons that induce energy consumption and exhibit the effect of obesity treatment. However, most of the existing MAOBI inhibitors are irreversible inhibitors, and there is a problem that they are accompanied by various side effects. Accordingly, drugs that can reversibly inhibit MAOBI are being researched and developed, but no notable reversible MAOBI inhibitor that can effectively act on obesity has been prescribed to date.
REF
Regulatory Toxicology and Pharmacology (2020), 117, 104733
Toxicological Research (Cham, Switzerland) (2023), 39(4), 693-709
Combinatorial Chemistry & High Throughput Screening (2020), 23(9), 836-841
KR2023027416,
WO2023022256
WO2023022256
WO2016052928
PATENT
WO2016052928
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2016052928&_cid=P20-M8XX0L-81795-1


Using L-Alaninamide hydrochloride or D-Alaninamide hydrochloride, a reductive amination reaction was performed with the compound of step (a) to obtain an imine compound (step b, reaction scheme 1b), which was then reduced with sodium cyanoborohydride to obtain an amine compound (step c, reaction scheme 1c).
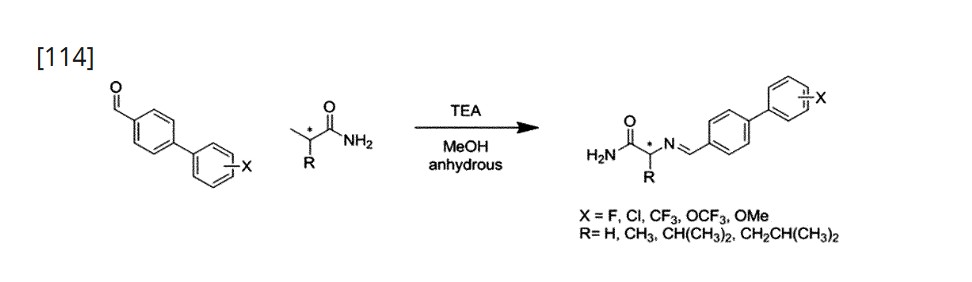
[112]Add 1.2 equivalents of Glycinamide hydrochloride or L-Alaninamide hydrochloride or D-Alaninamide hydrochloride or L-Valinamide hydrochloride or L-Leucinamide hydrochloride to anhydrous methanol at a concentration of 0.92 molar, and then add 1.5 equivalents of triethylamine. When the solution becomes transparent, add 1.0 equivalent of the aldehyde synthesized in step (a). After two hours, wash with ethyl acetate and distilled water. Dry the organic layer with sodium sulfate and concentrate in vacuo. Dissolve the concentrated reaction solution in anhydrous methanol at a concentration of 1.0 molar, and add 4.0 equivalents of sodium cyanoborohydride at 0 ℃. Then, react at room temperature for 18 hours, and after completion of the reaction, wash the reaction solution with ethyl acetate and distilled water. The organic layer was dried over sodium sulfate, concentrated in vacuo, and separated and purified using silica gel column chromatography.
References
- ^ Jump up to:a b c d “KDS 2010”. AdisInsight. 6 February 2025. Retrieved 24 February 2025.
- ^ Jump up to:a b c “Delving into the Latest Updates on KDS-2010 with Synapse”. Synapse. 23 January 2025. Retrieved 24 February 2025.
- ^ Nam MH, Sa M, Ju YH, Park MG, Lee CJ (April 2022). “Revisiting the Role of Astrocytic MAOB in Parkinson’s Disease”. International Journal of Molecular Sciences. 23 (8): 4453. doi:10.3390/ijms23084453. PMC 9028367. PMID 35457272.
4.4. KDS2010 A recently developed KDS2010, which is ~12,500-fold more selective to MAOB than MAOA, differentiates the role of MAOB from MAOA and reports that MAOB does not contribute to DA degradation [39]. KDS2010 is a potent (IC50 = 7.6 nM), and selective MAOB inhibitor named shows no known off-target effect (no other enzymes or channels causing >40% inhibition) or toxicity for 4 weeks of repeated dosing in non-human primates [16,41]. KDS2010 was turned out to be highly effective for alleviating the PD-related motor symptoms and PD-like pathology, including reactive astrogliosis, excessive astrocytic GABA, and nigrostriatal DAergic neuronal loss in multiple rodent models of PD [41]. Its clinical efficacy is still waiting to be tested in future studies.
- ^ Duarte P, Cuadrado A, León R (2021). “Monoamine Oxidase Inhibitors: From Classic to New Clinical Approaches”. Handbook of Experimental Pharmacology. 264: 229–259. doi:10.1007/164_2020_384. ISBN 978-3-030-68509-6. PMID 32852645.
KDS2010 is a novel compound highly potent and selective reversible MAO-B inhibitor (Fig. 2). It has demonstrated learning and memory improvements, promotion of synaptic transmission, and reduction of astrogliosis and astrocytic GABA levels in APP/presenilin 1 mice (Park et al. 2019).
| Clinical data | |
|---|---|
| Other names | KDS-2010; KDS2010; SeReMABI |
| Drug class | Reversible monoamine oxidase B (MAO-B) inhibitor |
| Identifiers | |
| showIUPAC name | |
| CAS Number | 1894207-44-3 |
| PubChem CID | 132023446 |
| ChemSpider | 128942408 |
| UNII | PCH79KLX33 |
| ChEMBL | ChEMBL5314546 |
| Chemical and physical data | |
| Formula | C17H17F3N2O |
| Molar mass | 322.331 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| showSMILES | |
| showInChI | |
///////////Tisolagiline, PCH79KLX33
Avenciguat



Avenciguat, 1579514-06-9
BI-685509, 582.7 g/mol, C34H38N4O5
UNII ZA7KTB4PSP
5-ethoxy-1-[6-[3-methyl-2-[[5-methyl-2-(oxan-4-yl)-3,4-dihydro-1H-isoquinolin-6-yl]methoxy]phenyl]pyridin-2-yl]pyrazole-4-carboxylic acid
Avenciguat (BI-685509) is a potent and orally active sGC activator. Avenciguat restores cyclic guanosine monophosphate (cGMP) and improves functionality of nitric oxide (NO) pathways. Avenciguat can be used in research of chronic kidney disease (CKD) and diabetic kidney disease (DKD).
Avenciguat is under investigation in clinical trial NCT05282121 (A Study to Test Whether BI 685509 Alone or in Combination With Empagliflozin Helps People With Liver Cirrhosis Caused by Viral Hepatitis or Non-alcoholic Steatohepatitis (NASH) Who Have High Blood Pressure in the Portal Vein (Main Vessel Going to the Liver)).
Avenciguat (development name BI 685509) is a soluble guanylate cyclase activator developed by Boehringer Ingelheim for kidney disease,[1][2] and cirrhosis.[3][4][5]
SCHEME

Ref
PAPER
Journal of Pharmacology and Experimental Therapeutics (2023), 384(3), 382-39
PATENT
Boehringer Ingelheim International GmbH
WO2014039434
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2014039434&_cid=P12-M29UB4-37937-1

PATENT
US20230293513
WO2020011804
| Clinical data | |
|---|---|
| Other names | BI 685509 |
| Legal status | |
| Legal status | Investigational |
| Identifiers | |
| showIUPAC name | |
| CAS Number | 1579514-06-9 |
| PubChem CID | 89992620 |
| UNII | ZA7KTB4PSP |
| Chemical and physical data | |
| Formula | C34H38N4O5 |
| Molar mass | 582.701 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| showSMILES | |
| showInChI | |
^ Cherney, David Z. I.; de Zeeuw, Dick; Heerspink, Hiddo J. L.; Cardona, Jose; Desch, Marc; Wenz, Arne; Schulze, Friedrich; Nangaku, Masaomi (August 2023). “Safety, tolerability, pharmacodynamics and pharmacokinetics of the soluble guanylyl cyclase activator BI 685509 in patients with diabetic kidney disease: A randomized trial”. Diabetes, Obesity and Metabolism. 25 (8): 2218–2226. doi:10.1111/dom.15099. PMID 37232058. S2CID 258909393.
^ Reinhart, Glenn A.; Harrison, Paul C.; Lincoln, Kathleen; Chen, Hongxing; Sun, Peng; Hill, Jon; Qian, Hu Sheng; McHugh, Mark C.; Clifford, Holly; Ng, Khing Jow; Wang, Hong; Fowler, Danielle; Gueneva-Boucheva, Kristina; Brenneman, Jehrod B.; Bosanac, Todd; Wong, Diane; Fryer, Ryan M.; Sarko, Chris; Boustany-Kari, Carine M.; Pullen, Steven S. (March 2023). “The Novel, Clinical-Stage Soluble Guanylate Cyclase Activator BI 685509 Protects from Disease Progression in Models of Renal Injury and Disease”. Journal of Pharmacology and Experimental Therapeutics. 384 (3): 382–392. doi:10.1124/jpet.122.001423. PMID 36507845. S2CID 254387173.
^ Lawitz, Eric J.; Reiberger, Thomas; Schattenberg, Jörn M.; Schoelch, Corinna; Coxson, Harvey O.; Wong, Diane; Ertle, Judith (November 2023). “Safety and pharmacokinetics of BI 685509, a soluble guanylyl cyclase activator, in patients with cirrhosis: A randomized Phase Ib study”. Hepatology Communications. 7 (11). doi:10.1097/HC9.0000000000000276. PMC 10615399. PMID 37889522.
^ Jones, Amanda K.; Chen, Hongxing; Ng, Khing Jow; Villalona, Jorge; McHugh, Mark; Zeveleva, Svetlana; Wilks, James; Brilisauer, Klaus; Bretschneider, Tom; Qian, Hu Sheng; Fryer, Ryan M. (July 2023). “Soluble Guanylyl Cyclase Activator BI 685509 Reduces Portal Hypertension and Portosystemic Shunting in a Rat Thioacetamide-Induced Cirrhosis Model”. Journal of Pharmacology and Experimental Therapeutics. 386 (1): 70–79. doi:10.1124/jpet.122.001532. PMID 37230799. S2CID 258909514.
^ Reiberger, Thomas; Berzigotti, Annalisa; Trebicka, Jonel; Ertle, Judith; Gashaw, Isabella; Swallow, Ros; Tomisser, Andrea (24 April 2023). “The rationale and study design of two phase II trials examining the effects of BI 685509, a soluble guanylyl cyclase activator, on clinically significant portal hypertension in patients with compensated cirrhosis”. Trials. 24 (1): 293. doi:10.1186/s13063-023-07291-3. PMC 10123479. PMID 37095557.
////////////Avenciguat, 1579514-06-9, BI 685509,
VALILTRAMIPROSATE


VALILTRAMIPROSATE
1034190-08-3
- (S)-3-(2-Amino-3-methylbutanamido)propane-1-sulfonic acid
- BLU8499
- WHO 11912
| Molecular Weight | 238.30 |
|---|---|
| Formula | C8H18N2O4S |
| CAS No. | 1034190-08-3 |
ALZ-801
Synonyms: valiltramiprosate, NRM-8499, homotaurine prodrug, 3-APS
This is a prodrug of homotaurine, a modified amino acid previously developed under the names tramiprosate and Alzhemed™. ALZ-801 is converted to homotaurine in vivo, but is more easily absorbed and lasts longer in the blood than tramiprosate.
Tramiprosate was reported to inhibit Aβ42 aggregation into toxic oligomers (Gervais et al., 2007; Kocis et al., 2017). Both ALZ-801 and tramiprosate are metabolized to 3-sulfopranpanoic acid (3-SPA), which is normally found in brain and also inhibits Aβ42 aggregation (Hey et al., 2018). A more recent study found that homotaurine activates GABA receptors, and suggests an alternative mechanism of action for ALZ-801 (Meera et al., 2023).
After tramiprosate failed in Phase 3, its maker, NeuroChem, marketed it as a nutritional supplement. Years later, a subgroup analysis of the trial data indicated a potential positive effect in participants who carried two copies of ApoE4 (Abushakra et al., 2016; Abushakra et al., 2017). Alzheon licensed ALZ-801 from NeuroChem and is developing it for Alzheimer’s disease.
ALZ-801 is a potent and orally available small-molecule β-amyloid (Aβ) anti-oligomer and aggregation inhibitor, valine-conjugated proagent of Tramiprosate with substantially improved PK properties and gastrointestinal tolerability compared with the parent compound. ALZ-801 is an advanced and markedly improved candidate for the treatment of alzheimer’s disease.
SCHEME

REF 1
US20080146642
https://patents.google.com/patent/US20080146642A1/en
HCL WATER, Dowex™ Marathon™ C ion-exchange column
General/Typical Procedure: [0311] (i) The solid material was dissolved in water (25 mL). The solution was passed through a Dowex™ Marathon™ C ion-exchange column (strongly acidic, 110 g (5 eq), prewashed). The strong acidic fractions were combined and treated with concentrated HCl (10 mL). The mixture was stirred at 50° C. for 30 minutes, and then was concentrated to dryness. The residual material was co-evaporated with EtOH (ethanol) to completely remove water. EtOH (100 mL) was added to the residue. The mixture was stirred at reflux for 1 h, and then cooled to room temperature. The solid material was collected by filtration. The solid material was dissolved in water (10 mL). The solution was added drop wise to EtOH (100 mL). The product slowly crystallized. The suspension was stirred at room temperature for 30 minutes. The solid material was collected by filtration and it was dried in a vacuum oven (60° C.). ID A2. 1H NMR (D2O).δ. 0.87-0.90 (m, 6H), 1.83 (qt, J = 7.2 Hz, 2H), 2.02-2.09 (m, 1H), 2.79 (t, J = 7.8 Hz, 2H), 3.20-3.29 (m, 2H), 3.60 (d, J = 6.3 Hz, 2H); 13C NMR (D2O).δ. 17.20, 17.77, 24.11, 30.00, 38.29, 48.63, 58.96, 169.35; m/z 237 (M-1).
- [1]. John A. Hey, et al. Discovery and Identification of an Endogenous Metabolite of Tramiprosate and Its Prodrug ALZ-801 that Inhibits Beta Amyloid Oligomer Formation in the Human Brain. CNS Drugs. 2018; 32(9): 849–861.[2]. Hey JA, et al. Clinical Pharmacokinetics and Safety of ALZ-801, a Novel Prodrug of Tramiprosate in Development for the Treatment of Alzheimer’s Disease. Clin Pharmacokinet. 2018 Mar;57(3):315-333. [Content Brief]
////////VALILTRAMIPROSATE, ALZ-801, ALZ 801, BLU 8499, WHO 11912
ATUZAGINSTAT


ATUZAGINSTAT, COR388
cas 2211981-76-7
Cyclopentanecarboxamide, N-[(1S)-5-amino-1-[2-(2,3,6-trifluorophenoxy)acetyl]pentyl]-
Cyclopentanecarboxamide, n-((1s)-5-amino-1-(2-(2,3,6-trifluorophenoxy)acetyl)pentyl)-N-((3s)-7-amino-2-oxo-1-(2,3,6- trifluorophenoxy)heptan-3-yl)cyclopentanecarboxamide
C19H25F3N2O3
386.415
UNII-DGN7ROZ8EN
- OriginatorCortexyme
- DeveloperQuince Therapeutics
- ClassAnti-inflammatories; Antibacterials; Antidementias; Antineoplastics; Antiparkinsonians; Neuroprotectants; Small molecules
- Mechanism of ActionPeptide hydrolase inhibitors
- Phase II/IIIAlzheimer’s disease
- Phase IIPeriodontal disorders
- PreclinicalParkinson’s disease; Squamous cell cancer
- 27 Jan 2023COR 388 licensed to Lighthouse Pharmaceuticals in the US
- 01 Aug 2022Atuzaginstat is available for licensing as of 01 Aug 2022. http://www.quincetx.com
- 01 Aug 2022Cortexyme is now called Quince Therapeutics
You need to be a logged in or subscribed to view this content
This small molecule is an orally available protease inhibitor targeting the lysine proteases of the periodontal pathogen Porphyromonas gingivalis. Known as gingipains, these proteases penetrate gingival tissue and cause inflammation at the site of periodontitis (O’Brien-Simpson et al., 2009). Periodontitis has been linked epidemiologically to cognitive impairment, and P. gingivalis bacterial lipopolysaccharide has been detected in postmortem brain tissue of people with AD (Poole et al., 2013). Oral P. gingivalis has been called a risk factor for Alzheimer’s disease (Kanagasingam et al., 2020).
Cortexyme’s approach is based on the theory that P. gingivalis invades the brain, where gingipains contribute to Alzheimer’s pathology (see Sabbagh and Decourt, 2022). The company reported elevated gingipain in brain tissue from people with AD, and a correlation between levels of gingipain and tau proteins in postmortem middle temporal gyrus from AD and healthy control tissue. P. gingivalis DNA was detected in postmortem cortices from people with AD and healthy controls, and in CSF of AD patients (Jan 2019 news on Dominy et al., 2019). In the same study, they show that in mice, oral P. gingivalis infection led to the appearance of bacterial DNA in the brain, increased brain Aβ42 production, neuroinflammation, and hippocampal degeneration. The first three findings were reported to be reduced by atuzaginstat; results for hippocampal cell death were not reported.
In preclinical work from other labs, infection with P. gingivalis was reported to worsen AD pathology and cognitive impairment in AD transgenic mice, and to cause neuroinflammation, memory impairment, neurodegeneration, micro- and astrogliosis, increased brain Aβ and phospho-tau, and neurofibrillary tangles in wild-type C57Bl6 mice (Ishida et al., 2017; Ilievski et al., 2018; Ding et al., 2018). For a review of the preclinical literature, see Costa et al., 2021.
In human neurons grown in culture, P. gingivalis infection led to tau phosphorylation and degradation, synapse loss, and cell death (Haditsch et al., 2020).
P. gingivalis is associated with cardiovascular disease. In rabbits, oral infection was reported to increase arterial plaque and levels of the inflammatory marker CRP. Both were reversed by treatment with COR388 (2020 AAIC abstract). In aged dogs with periodontal disease, ninety days of COR388 reduced oral bacterial load and gum pathology (Arastu-Kapur et al., 2020). In addition, older dogs had bacterial antigens and ribosomal RNA in their brains, consistent with systemic infection seen in humans.
Findings
Two Phase 1 trials of atuzaginstat were completed by June 2019. In a single-dose study of 5 to 250 mg capsules in 34 healthy adults, the compound was safe and well-tolerated. A multiple-dose study assessed safety and tolerability in 24 healthy older adults (mean age of 60 years) and nine with AD (mean age 72). According to a company press release and a poster presentation at the 2018 CTAD conference, healthy adults received 25, 50, or 100 mg COR388 or placebo every 12 hours for 10 days; AD patients took 50 mg or placebo every 12 hours for 28 days. The pharmacokinetic profiles of COR388 in AD and controls were reported to be similar. All volunteers with AD had P. gingivalis DNA fragments in their CSF at baseline. COR388 caused no serious adverse reactions, and no one withdrew. Gingipains also were reported to degrade ApoE, and 28 days of treatment with COR388 was claimed to reduce CSF ApoE fragments (2020 AAIC abstract).
A Phase 2/3 trial (GAIN) evaluating a 48-week course of COR388 in 643 people with mild to moderate AD began in April 2019. Participants took either 40 mg, 80 mg, or placebo twice daily. The primary endpoint was to be ADAS-Cog11 score, and the ADCS-ADL was added later as a co-primary functional endpoint. Further outcomes included CDR-SB, MMSE, NPI, the Winterlight Speech Assessment, MRI brain scans, and change in periodontal disease status. Investigators assessed CSF Aβ and tau, plus P. gingivalis DNA and gingipains in CSF, blood, and saliva, before and after treatment. A dental substudy of 228 participants is assessing effects of COR388 on periodontal disease. This trial involves 93 sites in the U.S. and Europe. The U.S. sites are offering a 48-week open-label extension.
According to a presentation at the 2020 CTAD, GAIN was fully enrolled. At baseline, more than 80 percent of participants had CSF Aβ and tau levels consistent with amyloid positivity or an AD diagnosis. All had detectable antibodies to P. gingivalis in their blood. In the dental substudy, 90 percent had periodontal disease. In December 2020, an independent data-monitoring committee recommended continuing the trial after a planned futility analysis of 300 patients treated for six months (press release).
In February 2021, the FDA placed a partial clinical hold on GAIN because of liver abnormalities in some participants (press release). Dosing in the open-label extension was stopped, but the placebo-controlled portion of GAIN continued. Cortexyme characterized the liver effects as reversible and showing no risk of long-term effects.
In October 2021, Cortexyme announced top-line results indicating the trial had missed its co-primary endpoints of ADAS-Cog11 and ADCS-ADL (press release). The company reported a statistically significant 57 percent slowing of decline on the ADAS-Cog11 in a subgroup with detectable saliva P. gingivalis DNA at baseline who took the higher dose; a 42 percent slowing on the lower dose did not reach statistical significance. This prespecified subgroup analysis included 242 participants; it found no effect on the ADCS-ADL. Improvements in ADAS-Cog and other cognitive endpoints correlated with reductions in saliva P. gingivalis DNA, according to data presented at CTAD 2021 in November. The most common treatment-related adverse events were gastrointestinal, occurring in 12 to 15 percent of treated participants. The treatment groups had dose-related liver enzyme elevations greater than three times the upper limit of normal, in 7 and 15 percent of participants on low and high doses, respectively, with bilirubin elevation reported in two participants on the high dose. The elevations occurred mainly in the first six weeks of treatment, and all resolved without long-term effects. Discontinuations due to transaminase elevations numbered one on placebo, and five and 17 in the 40 mg and 80 mg groups, respectively. The overall dropout rate was 25 percent in the placebo group, and 40 percent in atuzaginstat groups. There were five deaths in the high dose arm, and one in the low dose. All were deemed unrelated to drug. There was no evidence of ARIA or other imaging abnormalities.
At CTAD, the company announced plans for a confirmatory trial, pending discussions with regulators. The plan was to test atuzaginstat in people with mild to moderate AD and evidence of P. gingivalis infection, at the lower dose of 40 mg twice daily, reached by titration to minimize liver effects. The company was also planning a trial in Parkinson’s disease to begin in 2022. These trials were never registered.
In September 2021, Cortexyme began a Phase 1 trial of a second-generation lysin-gingipain inhibitor, COR588 (press release). This compound is expected to require only once-daily dosing. Results were expected in May 2022.
In January 2022, the company announced that the FDA had placed a full clinical hold on atuzaginstat due to concerns about liver toxicity (press release). The company said it intended to develop its backup compound, COR588, for Alzheimer’s disease, pending Phase 1 results. In July 2022, Cortexyme announced that COR588 had met safety and tolerability endpoints in a single- and multiple-ascending dose study in healthy adults (press release).
In August 2022, Cortexyme discontinued the gingipain inhibitor program, and offered it for external licensing (press release). The company changed its name to Quince, and its focus to bone disease. In January 2023, Quince put out word that it had sold Cortexyme’s legacy small molecule protease inhibitor portfolio to Lighthouse Pharmaceuticals, a company co-founded by a former Cortexyme CEO (press release).
For all trials of atuzaginstat, see clinicaltrials.gov.
SCHEME

Patent
- US10730826, Compound 1a-racemic
- US10730826, Compound 1a-non-racemic
- Ketone inhibitors of lysine gingipainPublication Number: EP-3512846-A1Priority Date: 2016-09-16
- Ketone inhibitors of lysine gingipainPublication Number: US-2019210960-A1Priority Date: 2016-09-16
- Ketone inhibitors of lysine gingipainPublication Number: WO-2018053353-A1Priority Date: 2016-09-16
- Ketone inhibitors of lysine gingipainPublication Number: US-10730826-B2Priority Date: 2016-09-16Grant Date: 2020-08-04
- Ketone inhibitors of lysine gingipainPublication Number: US-2021053908-A1Priority Date: 2016-09-16
PATENT
WO2018053353
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2018053353&_cid=P10-M1OFBK-46119-1



VIII. Examples
Example 1. Preparation of (S)-N-(7-amino-2-oxo-1-(2,3,6-trifluorophenoxy)heptan-3- yl)cyclopentanecarboxamide(1)hydrochloride
[0224] To a mixture of compound 1.4 (23.0 g, 67.2 mmol, 1.00 eq) in THF (200 mL) was added NMM (6.79 g, 67.2 mmol, 7.38 mL, 1.00 eq), isobutyl carbonochloridate (9.17 g, 67.2 mmol, 8.82 mL, 1.00 eq), and diazomethane (5.65 g, 134 mmol, 2.00 eq) at -40 °C under N2 (15 psi). The mixture was stirred at 0 °C for 30 min. LCMS showed the reaction was completed. FLO (200 mL) was added to the reaction and extracted with two 300-mL portions of ethyl acetate. The combined organic phase was washed with two 200-mL portions of brine (200, dried with anhydrous Na2SO4, filtered and concentrated under vacuum to provide crude compound 1.3 (30.0 g, crude) as a yellow oil.
[0225] To a mixture of compound 1.3 (20.0 g, 54.6 mmol, 1.00 eq) in EtOAc (300 mL) was
added hydrogen bromide(29.8 g, 121.7 mmol, 20.0 mL, 33% purity, 2.23 eq) at -20 °C under
N2 (15 psi). The mixture was stirred at -20 °C for 10 min. TLC (petroleum ether : ethyl
acetate = 0:1) showed the reaction was completed. The reaction was basified by addition of
saturated NaHCO3 until the pH of the mixture reached 8, and the mixture was extracted with
three 500-mL portions of EtOAc. The combined organic phase was washed with two 200-mL portions of brine, dried over anhydrous Na2SO4, filtered and concentrated under vacuum
to afford crude compound 1.2 (15.0 g, crude) as a yellow solid.
[0226] To a mixture of compound 1.2 (4.00 g, 9.54 mmol, 1.00 eq) in DMF (40.0 mL) was
added 2,6-difluorophenol (1.49 g, 11.4 mmol, 1.20 eq) and KF (1.66 g, 28.6 mmol, 670 μL,
3.00 eq) at 25 °C. The mixture was stirred at 25 °C for 3 h. TLC (petroleum ether: ethyl
acetate = 1:1) showed the reaction was completed. H2O (150 mL) was added to the mixture
and extracted with two 200-mL portions of ethyl acetate. The combined organic phase was
washed with two 100-mL portions of brine, dried with anhydrous Na2SO4, filtered, and
concentrated under vacuum. The residue was purified by silica gel chromatography
(petroleum ether: ethyl acetate = 100:1, 5:1) to afford compound 1.1 (2.50 g, 5.35 mmol,
56.1 % yield) as a yellow solid.
[0227] To a mixture of compound 1.1 (4.00 g, 8.22 mmol, 1.00 eq) in EtOAc (3.00 mL) was added HCl/EtOAc (40.0 mL) at 25 °C. The mixture was stirred at 25 °C for 2 h. TLC (petroleum ether : ethyl acetate=2:1) showed the reaction was completed. The mixture was concentrated in reduced pressure to provide (.S)-N-(7-amino-2-oxo-1-(2,3,6-trifluorophenoxy)heptan-3-yl)cyclopentanecarboxamide 1 hydrochloride salt (1.34 g, 3.16 mmol) as a light yellow solid. LCMS (ESI): m/z: [M + H] calcd for C19H25N2F3O3: 387.2; found 387.1; RT=2.508 min. 1HNMR (400 MHz, DMSO-d6) δ ppm 1.21 – 1.83 (m, 15 H) 2.60 – 2.81 (m, 3 H) 4.30 (ddd, J=9.70, 7.17, 4.52 Hz, 1 H) 5.02 – 5.22 (m, 2 H) 7.12 – 7.24 (m, 2 H) 7.98 (br s, 3 H) 8.32 (d, J=7.28 Hz, 1 H).
Paper Citations
- Raha D, Broce S, Haditsch U, Rodriguez L, Ermini F, Detke M, Kapur S, Hennings D, Roth T, Nguyen M, Holsinger LJ, Lynch CC, Dominy S. COR388, a novel gingipain inhibitor, decreases fragmentation of APOE in the central nervous system of Alzheimer’s disease patients: Abstract. Alzheimer’s & Dementia, 07 December 2020
- O’Brien-Simpson NM, Pathirana RD, Walker GD, Reynolds EC. Porphyromonas gingivalis RgpA-Kgp proteinase-adhesin complexes penetrate gingival tissue and induce proinflammatory cytokines or apoptosis in a concentration-dependent manner. Infect Immun. 2009 Mar;77(3):1246-61. Epub 2008 Dec 29 PubMed.
- Poole S, Singhrao SK, Kesavalu L, Curtis MA, Crean S. Determining the presence of periodontopathic virulence factors in short-term postmortem Alzheimer’s disease brain tissue. J Alzheimers Dis. 2013 Jan 1;36(4):665-77. PubMed.
- Kanagasingam S, Chukkapalli SS, Welbury R, Singhrao SK. Porphyromonas gingivalis is a Strong Risk Factor for Alzheimer’s Disease. J Alzheimers Dis Rep. 2020 Dec 14;4(1):501-511. PubMed.
- Sabbagh MN, Decourt B. COR388 (atuzaginstat): an investigational gingipain inhibitor for the treatment of Alzheimer disease. Expert Opin Investig Drugs. 2022 Oct;31(10):987-993. Epub 2022 Sep 1 PubMed.
- Dominy SS, Lynch C, Ermini F, Benedyk M, Marczyk A, Konradi A, Nguyen M, Haditsch U, Raha D, Griffin C, Holsinger LJ, Arastu-Kapur S, Kaba S, Lee A, Ryder MI, Potempa B, Mydel P, Hellvard A, Adamowicz K, Hasturk H, Walker GD, Reynolds EC, Faull RL, Curtis MA, Dragunow M, Potempa J. Porphyromonas gingivalis in Alzheimer’s disease brains: Evidence for disease causation and treatment with small-molecule inhibitors. Sci Adv. 2019 Jan;5(1):eaau3333. Epub 2019 Jan 23 PubMed.
- Ishida N, Ishihara Y, Ishida K, Tada H, Funaki-Kato Y, Hagiwara M, Ferdous T, Abdullah M, Mitani A, Michikawa M, Matsushita K. Periodontitis induced by bacterial infection exacerbates features of Alzheimer’s disease in transgenic mice. NPJ Aging Mech Dis. 2017;3:15. Epub 2017 Nov 6 PubMed.
- Ilievski V, Zuchowska PK, Green SJ, Toth PT, Ragozzino ME, Le K, Aljewari HW, O’Brien-Simpson NM, Reynolds EC, Watanabe K. Chronic oral application of a periodontal pathogen results in brain inflammation, neurodegeneration and amyloid beta production in wild type mice. PLoS One. 2018;13(10):e0204941. Epub 2018 Oct 3 PubMed.
- Ding Y, Ren J, Yu H, Yu W, Zhou Y. Porphyromonas gingivalis , a periodontitis causing bacterium, induces memory impairment and age-dependent neuroinflammation in mice. Immun Ageing. 2018;15:6. Epub 2018 Jan 30 PubMed.
- Costa MJ, de Araújo ID, da Rocha Alves L, da Silva RL, Dos Santos Calderon P, Borges BC, de Aquino Martins AR, de Vasconcelos Gurgel BC, Lins RD. Relationship of Porphyromonas gingivalis and Alzheimer’s disease: a systematic review of pre-clinical studies. Clin Oral Investig. 2021 Mar;25(3):797-806. Epub 2021 Jan 20 PubMed.
- Haditsch U, Roth T, Rodriguez L, Hancock S, Cecere T, Nguyen M, Arastu-Kapur S, Broce S, Raha D, Lynch CC, Holsinger LJ, Dominy SS, Ermini F. Alzheimer’s Disease-Like Neurodegeneration in Porphyromonas gingivalis Infected Neurons with Persistent Expression of Active Gingipains. J Alzheimers Dis. 2020;75(4):1361-1376. PubMed.
- Ermini F, Rojas P, Dean A, Stephens D, Patel M, Haditsch U, Roth T, Rodriguez L, Broce S, Raha D, Nguyen M, Kapur S, Lynch CC, Dominy SS, Holsinger LJ, Hasturk H. Targeting porphyromonas gingivalis to treat Alzheimer’s disease and comorbid cardiovascular disease: abstract. Alzheimer’s & Dementia, 07 December 2020
- Arastu-Kapur S, Nguyen M, Raha D, Ermini F, Haditsch U, Araujo J, De Lannoy IA, Ryder MI, Dominy SS, Lynch C, Holsinger LJ. Treatment of Porphyromonas gulae infection and downstream pathology in the aged dog by lysine-gingipain inhibitor COR388. Pharmacol Res Perspect. 2020 Feb;8(1):e00562. PubMed.
///////ATUZAGINSTAT, COR388, COR 388, Cortexyme, Quince Therapeutics

{kind=link}
{kind=link}