
 DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HERE
DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
.....FOR BLOG HOME CLICK HEREFlag and hits
ORGANIC SPECTROSCOPY

SUBSCRIBE

 Subscribe in a reader
Subscribe in a reader
Enter your email address:
Delivered by FeedBurner
Subscribe to New Drug Approvals by Email![]()

![]()



![]()
![]()





Recent Comments
| shivkr2 on SPSR Excellence Award 2025 – S… | |
| Bonkasaurus on Infigratinib phosphate | |
| PALOVAROTENE | ORGAN… on Palovarotene | |
| Pfizer just purchase… on Temanogrel | |
| Pfizer To Cash In On… on Temanogrel |
FDA Approves Botox Cosmetic to Improve the Appearance of Crow’s Feet Lines
WEDNESDAY, September 11, 2013 — The U.S. Food and Drug Administration today approved a new use for Botox Cosmetic (onabotulinumtoxinA) for the temporary improvement in the appearance of moderate to severe lateral canthal lines, known as crow’s feet, in adults. Botox Cosmetic is the only FDA approved drug treatment option for lateral canthal lines.
The FDA approved Botox Cosmetic in 2002 for the temporary improvement of glabellar lines (wrinkles between the eyebrows, known as frown lines), in adults. Botox Cosmetic works by keeping muscles from tightening so wrinkles are less prominent
READ ALL AT

BOTOX Cosmetic (onabotulinum toxin A) For Injection, is a sterile, vacuum-dried purifiedbotulinum toxin type A, produced from fermentation of Hall strain Clostridium botulinumtype A grown in a medium containing casein hydrolysate, glucose, and yeast extract, intended for intramuscular use. It is purified from the culture solution by dialysis and a series of acid precipitations to a complex consisting of the neurotoxin, and several accessory proteins. The complex is dissolved in sterile sodium chloride solution containing Albumin Human and is sterile filtered (0.2 microns) prior to filling and vacuum-drying.
The primary release procedure for BOTOX Cosmetic uses a cell-based potency assay to determine the potency relative to a reference standard. The assay is specific to Allergan’s products BOTOX and BOTOX Cosmetic. One Unit of BOTOX Cosmetic corresponds to the calculated median intraperitoneal lethal dose (LD50) in mice. Due to specific details of this assay such as the vehicle, dilution scheme and laboratory protocols, Units of biological activity of BOTOX Cosmetic cannot be compared to nor converted into Units of any other botulinum toxin or any toxin assessed with any other specific assay method. The specific activity of BOTOX Cosmetic is approximately 20 Units/nanogram of neurotoxin protein complex.
Each vial of BOTOX Cosmetic contains either 50 Units of Clostridium botulinum type A neurotoxin complex, 0.25 mg of Albumin Human, and 0.45 mg of sodium chloride; or 100 Units of Clostridium botulinum type A neurotoxin complex, 0.5 mg of Albumin Human, and 0.9 mg of sodium chloride in a sterile, vacuum-dried form without a preservative.
Since the approval of BOTOX® Cosmetic by the U.S. Food and Drug Administration in 2002, Allergan has virtually changed the face of medical aesthetics. Men and women between the ages of 18 to 65 now have the ability to choose science-based, non-invasive medical aesthetic solutions, including BOTOX® Cosmetic and the JUVÉDERM® family of dermal fillers, to achieve their own results. Over the last seven years, there have been nearly 11.8 million BOTOX® Cosmetic treatments recorded in the United States.1 More importantly, its 97 percent satisfaction rating (survey of 117 patients)2,3 is just one indication of the trust consumers have placed in Allergan.
BOTOX® Cosmetic is a simple, non-surgical procedure for temporarily reducing the appearance of moderate to severe glabellar lines – the vertical frown lines between the eyebrows that look like an “11” – in adult women and men aged 18 to 65. BOTOX® Cosmetic reduces the activity of the muscles that cause the “11s” to form by blocking nerve impulses that trigger wrinkle-causing muscle contractions, creating an improved appearance between the brows. Results can last up to four months and may vary with each patient. Ask your doctor if BOTOX® Cosmetic is right for you.
Gilead Submits New Drug Application to U.S. FDA for Idelalisib for the Treatment of Indolent Non-Hodgkin’s Lymphoma
CAL 101, IDELALISIB
SEPT 2013
Gilead Submits New Drug Application to U.S. FDA for Idelalisib for the Treatment of Indolent Non-Hodgkin’s Lymphoma
FOSTER CITY, Calif.–(BUSINESS WIRE)–Sep. 11, 2013– Gilead Sciences, Inc. today announced that the company has submitted a New Drug Application (NDA) to the U.S. Food and Drug Administration (FDA) for approval of idelalisib, an investigational, targeted, oral inhibitor of PI3K delta, for the treatment of indolent non-Hodgkin’s lymphoma (iNHL). The data submitted in this NDA support the use of idelalisib for patients with iNHL that is refractory (non-responsive) to rituximab and to alkylating-agent-containing chemotherapy.
read all at
Idelalisib ….US FDA Accepts NDA for Gilead’s Idelalisib for the Treatment of Refractory Indolent Non-Hodgkin’s Lymphoma
JANUARY 14, 2014 8:35 AM / LEAVE A COMMENT

An antineoplastic agent and p110delta inhibitor
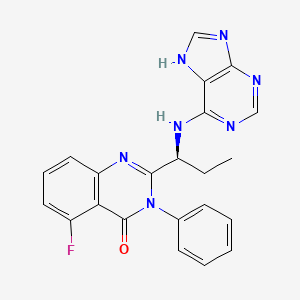
(S)-2-(1-(9H-purin-6-ylamino)propyl)-5-fluoro-3-phenylquinazolin-4(3H)-one
Icos (Originator)
- CAL-101
- GS-1101
- Idelalisib
- UNII-YG57I8T5M0
M.Wt: 415.43
Formula: C22H18FN7O
CAS No.: 870281-82-6
CAL-101 Solubility: DMSO ≥80mg/mL Water <1.2mg/mL Ethanol ≥33mg/mL
5-Fluoro-3-phenyl-2-[(1S)-1-(7H-purin-6-ylamino)propyl]-4(3H)-quinazolinone
idelalisib
Idelalisib (codenamed GS-1101 or CAL-101) is a drug under investigation for the treatment of chronic lymphocytic leukaemia. It is in Phase III clinical trials testing drug combinations with rituximab and/or bendamustine as of 2013. The substance acts as aphosphoinositide 3-kinase inhibitor; more specifically, it blocks P110δ, the delta isoform of the enzyme phosphoinositide 3-kinase.[1][2]
GDC-0032 is a potent, next-generation beta isoform-sparing PI3K inhibitor targeting PI3Kα/δ/γ with IC 50 of 0.29 nM/0.12 nM/0.97nM,> 10 fold over Selective PI3K [beta].
GS-1101 is a novel, orally available small molecule inhibitor of phosphatidylinositol 3-kinase delta (PI3Kdelta) develop by Gilead and is waiting for registration in U.S. for the treatment of patients with indolent non-Hodgkin’s lymphoma that is refractory (non-responsive) to rituximab and to alkylating-agent-containing chemotherapy and for the treatment of chronic lymphocytic leukemia. The compound is also in phase III clinical evaluation for the treatment of elderly patients with previously untreated small lymphocytic lymphoma (SLL) and acute myeloid leukemia. Clinical trials had been under way for the treatment of inflammation and allergic rhinitis; however, no recent development has been reported. Preclinical studies have shown that GS-1101 has desirable pharmaceutical properties. The compound was originally developed by Calistoga Pharmaceuticals, acquired by Gilead on April 1, 2011.
clinical trials, click link
http://clinicaltrials.gov/search/intervention=CAL-101%20OR%20GS-1101%20OR%20Idelalisib
FOSTER CITY, Calif.–(BUSINESS WIRE)–Jan. 13, 2014– Gilead Sciences, Inc. (Nasdaq: GILD) announced today that the U.S. Food and Drug Administration (FDA) has accepted for review the company’s New Drug Application (NDA) for idelalisib, a targeted, oral inhibitor of PI3K delta, for the treatment of refractory indolent non-Hodgkin’s lymphoma (iNHL). FDA has granted a standard review for the iNHL NDA and has set a target review date under the Prescription Drug User Fee Act (PDUFA) of September 11, 2014.
The NDA for iNHL, submitted on September 11, 2013, was supported by a single arm Phase 2 study (Study 101-09) evaluating idelalisib in patients with iNHL that is refractory (non-responsive) to rituximab and to alkylating-agent-containing chemotherapy. Following Gilead’s NDA submission for iNHL, FDA granted idelalisib a Breakthrough Therapy designation for relapsed chronic lymphocytic leukemia (CLL). The FDA grants Breakthrough Therapy designation to drug candidates that may offer major advances in treatment over existing options. Gilead submitted an NDA for idelalisib for the treatment of CLL on December 6, 2013.
About Idelalisib
Idelalisib is an investigational, highly selective oral inhibitor of phosphoinositide 3-kinase (PI3K) delta. PI3K delta signaling is critical for the activation, proliferation, survival and trafficking of B lymphocytes and is hyperactive in many B-cell malignancies. Idelalisib is being developed both as a single agent and in combination with approved and investigational therapies.
Gilead’s clinical development program for idelalisib in iNHL includes Study 101-09 in highly refractory patients and two Phase 3 studies of idelalisib in previously treated patients. The development program in CLL includes three Phase 3 studies of idelalisib in previously treated patients. Combination therapy with idelalisib and GS-9973, Gilead’s novel spleen tyrosine kinase (Syk) inhibitor, also is being evaluated in a Phase 2 trial of patients with relapsed or refractory CLL, iNHL and other lymphoid malignancies.
Additional information about clinical studies of idelalisib and Gilead’s other investigational cancer agents can be found at http://www.clinicaltrials.gov. Idelalisib and GS-9973 are investigational products and their safety and efficacy have not been established.
About Indolent Non-Hodgkin’s Lymphoma
Indolent non-Hodgkin’s lymphoma refers to a group of largely incurable slow-growing lymphomas that run a relapsing course after therapy and can lead ultimately to life-threatening complications such as serious infections and marrow failure. Most iNHL patients are diagnosed at an advanced stage of disease, and median survival from time of initial diagnosis for patients with the most common form of iNHL, follicular lymphoma, is 8 to 10 years. The outlook for refractory iNHL patients is significantly poorer.
About Gilead Sciences
Gilead Sciences is a biopharmaceutical company that discovers, develops and commercializes innovative therapeutics in areas of unmet medical need. The company’s mission is to advance the care of patients suffering from life-threatening diseases worldwide. Headquartered in Foster City, California, Gilead has operations in North and South America, Europe and Asia Pacific.
The delta form of PI3K is expressed primarily in blood-cell lineages, including cells that cause or mediate hematologic malignancies, inflammation, autoimmune diseases and allergies. By specifically inhibiting only PI3K delta, a therapeutic effect is exerted without inhibiting PI3K signalling that is critical to the normal function of healthy cells. Extensive studies have shown that inhibition of other PI3K forms can cause significant toxicities, particularly with respect to glucose metabolism, which is essential for normal cell activity.
In 2011, orphan drug designation was assigned to GS-1101 in the U.S. for the treatment of CLL. In 2013, several orphan drug designations were assigned to the compound in the E.U. and U.S.: for the treatment of follicular lymphoma, for the treatment of mucosa-associated lymphoid tissue lymphoma (MALT), for the treatment of nodal marginal zone lymphoma, for the treatment of splenic marginal zone lymphoma, and for the treatment of chronic lymphocytic leukemia/small lymphocytic lymphoma. Orphan drug designation was also assigned in the U.S. for the treatment of lymphoplasmacytic lymphoma with or without Walenstom’s macroglobulinemia and, in the E.U., for the treatment of Waldenstrom’s macroglobulinemia (lymphoplasmacytic lymphoma).
Later in 2013, some of these orphan drug designations were withdrawn in the E.U.; for the treatment of chronic lymphocytic leukemia / small lymphocytic lymphoma, for the treatment of extranodal marginal-zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma), for the treatment of of nodal marginal-zone lymphoma and for the treatment of splenic marginal-zone lymphoma. In 2013, the FDA granted a breakthrough therapy designation for the treatment of chronic lymphocytic leukemia.
- H. Spreitzer (13 May 2013). “Neue Wirkstoffe – Ibrutinib und Idelalisib”. Österreichische Apothekerzeitung (in German) (10/2013): 34.
- Wu, M.; Akinleye, A.; Zhu, X. (2013). “Novel agents for chronic lymphocytic leukemia”.Journal of Hematology & Oncology 6: 36. doi:10.1186/1756-8722-6-36.PMC 3659027. PMID 23680477.
CAL-101 is an Oral Delta Isoform-Selective PI3 Kinase Inhibitor.
| US8207153 | 6-27-2012 | QUINAZOLINONES AS INHIBITORS OF HUMAN PHOSPHATIDYLINOSITOL 3-KINASE DELTA |
| US2012015964 | 1-20-2012 | QUINAZOLINONES AS INHIBITORS OF HUMAN PHOSPHATIDYLINOSITOL 3-KINASE DELTA |
| US2011306622 | 12-16-2011 | METHODS OF TREATING HEMATOLOGICAL DISORDERS WITH QUINAZOLINONE COMPOUNDS IN SELECTED SUBJECTS |
| US7932260 | 4-27-2011 | Quinazolinones as Inhibitors of Human Phosphatidylinositol 3-Kinase Delta |
| US2011044942 | 2-25-2011 | METHODS OF TREATMENT FOR SOLID TUMORS |
| US2010256167 | 10-8-2010 | QUINAZOLINONES AS INHIBITORS OF HUMAN PHOSPHATIDYLINOSITOL 3-KINASE DELTA |
| US2010202963 | 8-13-2010 | THERAPIES FOR HEMATOLOGIC MALIGNANCIES |
| WO2005113556A1 * | 12 May 2005 | 1 Dec 2005 | Icos Corp | Quinazolinones as inhibitors of human phosphatidylinositol 3-kinase delta |
| WO2005117889A1 * | 12 Nov 2004 | 15 Dec 2005 | Didier Bouscary | Methods for treating and/or preventing aberrant proliferation of hematopoietic |
| WO2005120511A1 * | 4 Jun 2005 | 22 Dec 2005 | Joel S Hayflick | Methods for treating mast cell disorders |
| WO2006089106A2 * | 16 Feb 2006 | 24 Aug 2006 | Icos Corp | Phosphoinositide 3-kinase inhibitors for inhibiting leukocyte accumulation |
| US20060106038 * | 25 May 2005 | 18 May 2006 | Icos Corporation | Methods for treating and/or preventing aberrant proliferation of hematopoietic cells |
The synthesis of a compound in accordance with formula I is first exemplified using steps A-E below, which provide a synthetic procedure for compound 107, the structure of which is shown below.

(107) is idelalisib
……………….
Synthesis of 2-fluoro-6-nitro-N-phenyl-benzamide (108)
Step A: A solution of 2-fluoro-6- nitrobenzoic acid (100 g, 0.54 mol) and dimethylformamide (5 mL) in dichloromethane (600 mL) was treated dropwise with oxalyl chloride (2 M in dichloromethane, 410 mL, 0.8 mol, 1.5 eq) over 30 min. After stirring 2 h at room temperature, the reaction was concentrated to an orange syrup with some solids present. The syrup was dissolved in dry dioxane (80 mL) and slowly added to a suspension of aniline (49 mL, 0.54 mol, 1 eq) and sodium bicarbonate (90 g, 1.08 mol, 2 eq) in a mixture of dioxane (250 mL) and water (250 mL) at 6 0C. The temperature reached 27°C at the end of the addition. After 30 min, the reaction mixture was treated with water (1.2 L). The precipitate was collected by vacuum filtration, washed with water (300 mL) , air dried in the funnel, and dried in vacuo at 50°C for 24 h to afford an off-white solid product (139 g, 99%). 1H NMR (300 MHz, DMSO-d6) δ 10.82 (s, IH), 8.12 (d, J = 7.7 Hz, IH), 7.91-7.77 (m, 2H), 7.64 (d, J = 7.7 Hz, 2H), 7.38 (t, J = 7.9 Hz, 2H), 7.15 > (t, J = 7.4 Hz, IH), ESI-MS m/z 261 (MH+). The reaction described above and compound 108 are shown below.

………………………..
Synthesis of(S) – [1- (2-fluoro-6-nitro-benzoyl) -phenyl-aminocarbonyl] – propyl-carbamic acid tert-butyl ester (109)
Step B: A suspension of compound 108 (0.5 mol) and dimethylformamide (5 mL) in thionyl chloride (256 mL, 2.5 mol, 5 eq) was stirred at 85°C for 5 hours. The reaction mixture was concentrated in vacuo to a brown syrup. The syrup was dissolved in dichloromethane (200 mL) and was slowly added to a solution of N-BOC-L-2-aminobutyric acid (112 g, 0.55 mol, 1.1 eq) and triethylamine (77 mL, 0.55 mol, 1.1 eq) in dichloromethane (600 mL) at 10 0C. After stirring at room temperature for 3 h, salts were removed by filtration, and the solution was washed with 100 mL of water, saturated sodium bicarbonate, water, 5% citric acid, and saturated sodium chloride. The organic phase was dried with magnesium sulfate and concentrated to a red syrup. The syrup was dissolved in dichloromethane (450 mL) and purified by flash chromatography on a silica gel plug (15 x 22 cm, 4 L dry silica) eluted with hexanes/ethyl acetate (10%, 8 L; 15%, 8 L; 20%, 8 L; 25%, 4 L) to yield the compound 109 as an off-white solid (147 g, 66%). 1H NMR (300 MHz, DMSO-d6) δ 8.13 (d, J = 8.0 Hz, IH), 7.84 (t, J = 8.6 Hz, IH), 7.78- 7.67 (m, IH), 7.65-7.49 (m, 3H), 7.40-7.28 ( m, 2H), 7.19 (d, J = 7.5 Hz, IH), 4.05 (broad s, IH), 1.75- 1.30 (m, 2H), 1.34 (s, 9H), 0.93 (broad s, 3H). ESI- MS m/z 446.3 (MH+) . The reaction described above and compound 109 are shown below.

Synthesis of(S) – [1- (5-fluoro-4-oxo-3-phenyl-3 , 4-dihydro-quinazolin-2- yl) -propyl] -carbamic acid tert-butyl ester (110)
Step C: A solution of compound 109 (125 mmol, 1 eq) in acetic acid (500 mL) was treated with zinc dust (48.4 g, 740 mmol, 6 eq) added in 3 portions, and the reaction mixture was allowed to cool to below 35°C between additions. After stirring for 2 h at ambient temperature, solids were filtered off by vacuum filtration and washed with acetic acid (50 mL) . The filtrate was concentrated in vacuo, dissolved in EtOAc (400 mL) , washed with water (300 mL) , and the water layer was extracted with EtOAc (300 mL) . The combined organic layers were washed with water (200 mL) , sat’d sodium bicarbonate (2 x 200 mL) , sat’d NaCl (100 mL) , dried with MgSO4, and concentrated to a syrup. The syrup was dissolved in toluene (200 mL) and purified by flash chromatography on a silica gel plug (13 x 15 cm, 2 L dry silica) eluted with hexanes/ethyl acetate (10%, 4 L; 15%, 4 L; 17.5%, 8 L; 25%, 4 L) to yield compound 110 as an off-white foamy solid (33.6 g, 69%). 1H NMR (300 MHz, DMSO-d6) δ 7.83 (td, J = 8.2, 5.7 Hz, IH), 7.64-7.48 (m, 5H), 7.39 (broad d, J = 7.6 Hz, IH), 7.30 (dd, J = 8.3 Hz, IH), 7.23 (d, J = 7.6 Hz, IH), 4.02-3.90 (m, IH), 1.76-1.66 (m, IH), 1.62-1.46 (m, IH), 1.33 (s, 9H), 0.63 (t, J= 7.3 Hz, 3H). ESI-MS m/z 398.3 (MH+). The reaction described above and compound 110 are shown below.

…………..
Syn of (S) -2- (1-amino-propyl) -5-fluoro-3-phenyl-3H-quinazolin-4- one (111)
Step D: A solution of compound 110 (85 mmol) in dichloromethane (60 mL) was treated with trifluoroacetic acid (60 mL) . The reaction mixture was stirred for 1 h, concentrated in vacuo, and partitioned between dichloromethane (150 mL) and 10% K2CO3 (sufficient amount to keep the pH greated than 10) . The aqueous layer was extracted with additional dichloromethane (100 raL) , and the combined organic layers were washed with water (50 mli) and brine (50 mL) . After drying with Mg SO4, the solution was concentrated to provide compound 111 as an off-white solid (22 g, 88%) . 1H NMR (300 MHz,
CDCl3) δ 7.73-7.65 (m, IH), 7.62-7.49 (m, 4H), 7.32- 7.22 (m, 2H), 7.13-7.06 (m, IH), 3.42 (dd, J= 7.5, 5.2 Hz, IH), 1.87-1.70 (m, IH), 1.58-1.43 (m, IH), 0.80 (t, J = 7.4 Hz, 3H) . ESI-MS m/z 298.2 (MH+) . The reaction described above and compound 111 are shown below.

………………
syn of (S) -5-fluoro-3-phenyl-2- [1- (9H-purin-6-ylamino) -propyl] – 3H-quinazolin-4-one (107)
Step E: A suspension of compound 111(65.6 mmol, 1 eq) , 6-bromopurine (14.6 g, 73.4 mmol, 1.1 eq) , and DIEA (24.3 mL, 140 mmol, 2 eq) in tert- butanol (40 mL) was stirred for 24 h at 800C. The reaction mixture was concentrated in vacuo and treated with water to yield a solid crude product that was collected by vacuum filtration, washed with water, and air dried. Half of the obtained solid crude product was dissolved in MeOH (600 mL) , concentrated onto silica gel (300 mL dry) , and purified by flash chromatography (7.5 x 36 cm, eluted with 10 L of 4% MeOH/CH2Cl2) to yield a solid product. The solid product was then dissolved in EtOH (250 mL) and concentrated in vacuo to compound 107 idelalisib as a light yellow solid (7.2 g, 50%).
1H NMR (300 MHz, 80 0C, DMSO-d5) δ 12.66 (broad s, IH), 8.11 (s, IH), 8.02 (broad s, IH), 7.81-7.73 (m, IH),7.60-7.42 (m, 6H), 7.25-7.15 (m, 2H), 4.97 (broad s, IH), 2.02-1.73 (m, 2H), 0.79 (t, J= 7.3 Hz, 3H).
ESI-MS m/z 416.2 (MH+).
C, H, N elemental analysis (C22Hi8N7OF-EtOH- 0.4 H2O).
Chiral purity 99.8:0.2 (S:R) using chiral HPLC (4.6 x 250 mm Chiralpak ODH column, 20 °C, 85:15 hexanes : EtOH, 1 rnL/min, sample loaded at a concentration of 1 mg/mL in EtOH) . The reaction described above and compound 107 idelalisib are shown below.

| WO2001030768A1 * | 26 Oct 2000 | 3 May 2001 | Gustave Bergnes | Methods and compositions utilizing quinazolinones |
| WO2001081346A2 * | 24 Apr 2001 | 1 Nov 2001 | Icos Corp | Inhibitors of human phosphatidyl-inositol 3-kinase delta |
| WO2003035075A1 * | 27 Aug 2002 | 1 May 2003 | Icos Corp | Inhibitors of human phosphatidyl-inositol 3-kinase delta |
| WO2005016348A1 * | 13 Aug 2004 | 24 Feb 2005 | Jason Douangpanya | Method of inhibiting immune responses stimulated by an endogenous factor |
| WO2005016349A1 * | 13 Aug 2004 | 24 Feb 2005 | Thomas G Diacovo | Methods of inhibiting leukocyte accumulation |
| WO2005067901A2 * | 7 Jan 2005 | 28 Jul 2005 | Carrie A Northcott | Methods for treating and preventing hypertension and hypertension-related disorders |
3 Herbs you Need to Know for Healing Depression: Interview with Sarah Josey
Depression is a condition that reportedly affects one in ten Americans. It is a conversation often avoided, but I was lucky enough to interview Sarah Josey Herbalist, Nutritionist and Founder of Golden Poppy Herbal Apothecary. She shared three herbs that everyone should know about when it comes to depression and one to avoid, while on medication. Watch video.
Find out more about Sarah Josey and Golden Poppy Herbal Apothecary at http://www.goldenpoppyherbs.com/
Join the conversation below. Have you tried any of these herbs? Let me know in the comments.
SAMIDIRECT -Healthy, Wealthy & Wise, FREE OF COST CONSULTATION on Diabetes, Cancer, Arthritis, Osteoporosis, Heart- Liver -Lung & Kidney problems, Low Immunity, Alzheimer, Weight Management, Weak Memory, Neutritional Deficiency, UTI problems
![]()

Healthy, Wealthy & Wise
For over 25 years the Sami Group has been unlocking the mystery of herbs, extracting the goodness, and gifting the world with good health.
Now the Sami Group provides YOU an opportunity to unlock the mystery of Success, Wealth & Better living.
FREE OF COST CONSULTATION on Diabetes, Cancer, Arthritis, Osteoporosis, Heart- Liver -Lung & Kidney problems, Low Immunity, Alzheimer, Weight Management, Weak Memory, Neutritional Deficiency, UTI problems etc.
(REVOLUTIONARY AYURVEDIC SOLUTIONS with ISO 22000 Certified Indian MNC after 25 years of R & D by 120 Scientists.
Numberless Testimonials.)
http://www.samidirect.com/products/
Do visit the website www.samidirect.com & have the study in detail. Have a look at the Sami Direct Corporate Video on you tube. If you get the wonderful potential of the brightest future…do call me for ‘How to get started?’




…..









DISTRIBUTOR ENQUIRY WELCOME
CONTACT MR JAY DESAI
REGARDS
+91 9699952526
Mumbai, INDIA
email-jaydesai1502@gmail.com
 |
Bussines Sami Direct Seminar ppt.ppt1.pdf 9204K View Download |
samidirect corporate video

DR MAJID, FOUNDER , SAMIDIRECT
Dr. Muhammed Majeed
Dear Friend, Congratulations on your decision!
A little over three decades ago I went from a small town in South India to the United States Of America seeking fulfillment of my dreams. Today with a business conglomerate spread across the globe, I can confidently say that the future belongs to those who believe in the beauty of their dreams.
The aspiration to dream and the conviction to follow their dreams is what sets apart the extraordinary from the ordinary. Congratulations for choosing to be among the extraordinary. Now we are in it together. You have chosen the right place and the right means. The awesome combination of extensively researched products and a revolutionary business plan is a definite formula for success. We are with you at every step to help you fulfill your dreams and reach greater heights.
Dr. Muhammed Majeed
Welcome home again!
– See more at: http://www.samidirect.com/about/founder-desk/#sthash.rrOCRiJ1.dpuf
Sami Direct, as a part of the Sami Group, is the culmination of relentless Research and Development for more than two decades. We at Sami Direct are committed to offer you an unrivalled range of nutraceuticals, soon to be followed by cosmeceutical products, which have been acknowledged by the world over for its highest quality and safety standards.
Sami Direct is supported by its very own R&D facility- SAMI LABS LTD., located in Bangalore. This state-of-the-art, multi-disciplinary division pursues diverse fields of research with over 120 scientists focusing all efforts towards creating effective and safe products. With six highly advanced cutting-edge manufacturing units adhering to the strictest quality and safety standards, Sami Direct ensures that the highest quality of products are being produced.
Today the Sami Group holds a strong intellectual property portfolio with over 70 US and International Patents to its credit including awards and recognitions worldwide.
With the perfect blend of world class products and a revolutionary business plan, it is a lifetime opportunity not just to enhance your health, but also a fruitful and lasting career heightening your income.
DISTRIBUTOR ENQUIRY WELCOME
CONTACT MR JAY DESAI
REGARDS
+91 9699952526
Mumbai, INDIA
email; jaydesai1502@gmail.com
“5TH PHARMACOVIGILANCE CONGREGATION 2013–20th November 2013, Kohinoor Continental Hotel, Mumbai, India.
DRUG REGULATORY AFFAIRS INTERNATIONAL

“5TH PHARMACOVIGILANCE CONGREGATION 2013”
“Ensuring safer drugs to market by analyzing latest developments in pharmacovigilance, drug safety and risk management”
20th November 2013, Kohinoor Continental Hotel, Mumbai, India.
Greetings from Virtue Insight,
I am happy to invite you and your colleagues to be a sponsor/ delegate for our upcoming “5th Pharmacovigilance Congregation 2013” The conference will be held on 20th November 2013, Kohinoor Continental Hotel, Mumbai, India.
KEY SPEAKERS:-
- Deepa Arora, Global Head, Drug Safety & Risk Management, Lupin
- Arun Bhatt, President, Clininvent Research
- Moin Don, Executive Director, PVCON Pharmacovigilance Auditing & Consulting Services
- Bhaswat Chakraborty, Senior Vice President, Research & Development, Cadila Pharmaceuticals
- Parminder Kaur, Owner & Regulatory Affairs & PhV Consultant (QPPV), RegPak BioPharma Consulting (Netherlands, UK)
- Babita Kirodian, Head – Pharmacovigilance, Bristol-Myers Squibb
- Rajani Rokade, Head – Pharmacovigilance, Sanofi Aventis
- Veena Rajan, Head – Patient Safety, AstraZeneca
- Sofi Joseph, Head –…
View original post 465 more words
Stem cells
……………………………..
Stem cells are undifferentiated biological cells, that can differentiate into specialized cells and can divide (through mitosis) to produce more stem cells. They are found in multicellular organisms. In mammals, there are two broad types of stem cells: embryonic stem cells, which are isolated from the inner cell mass of blastocysts, and adult stem cells, which are found in various tissues. In adult organisms, stem cells and progenitor cells act as a repair system for the body, replenishing adult tissues. In a developing embryo, stem cells can differentiate into all the specialized cells—ectoderm, endoderm and mesoderm (see induced pluripotent stem cells)—but also maintain the normal turnover of regenerative organs, such as blood, skin, or intestinal tissues.
There are three accessible sources of autologous adult stem cells in humans:
- Bone marrow, which requires extraction by harvesting, that is, drilling into bone (typically the femur or iliac crest),
- Adipose tissue (lipid cells), which requires extraction by liposuction, and
- Blood, which requires extraction through pheresis, wherein blood is drawn from the donor (similar to a blood donation), passed through a machine that extracts the stem cells and returns other portions of the blood to the donor.
Stem cells can also be taken from umbilical cord blood just after birth. Of all stem cell types, autologous harvesting involves the least risk. By definition, autologous cells are obtained from one’s own body, just as one may bank his or her own blood for elective surgical procedures.
Highly plastic adult stem cells are routinely used in medical therapies, for example in bone marrow transplantation. Stem cells can now be artificially grown and transformed (differentiated) into specialized cell types with characteristics consistent with cells of various tissues such as muscles or nerves through cell culture. Embryonic cell lines and autologous embryonic stem cells generated through therapeutic cloning have also been proposed as promising candidates for future therapies. Research into stem cells grew out of findings by Ernest A. McCulloch and James E. Till at the University of Toronto in the 1960s
……………

Medical researchers believe that stem cell therapy has the potential to dramatically change the treatment of human disease. A number of adult stem cell therapies already exist, particularly bone marrow transplants that are used to treat leukemia. In the future, medical researchers anticipate being able to use technologies derived from stem cell research to treat a wider variety of diseases including cancer, Parkinson’s disease, spinal cord injuries, Amyotrophic lateral sclerosis, multiple sclerosis, and muscle damage, amongst a number of other impairments and conditions. However, there still exists a great deal of social and scientific uncertainty surrounding stem cell research, which could possibly be overcome through public debate and future research, and further education of the public.
One concern of treatment is the risk that transplanted stem cells could form tumors and become cancerous if cell division continues uncontrollably.
Stem cells are widely studied, for their potential therapeutic use and for their inherent interest.
Supporters of embryonic stem cell research argue that such research should be pursued because the resultant treatments could have significant medical potential. It has been proposed that surplus embryos created for in vitro fertilization could be donated with consent and used for the research.
The recent development of iPS cells has been called a bypass of the legal controversy. Laws limiting the destruction of human embryos have been credited for being the reason for development of iPS cells, but it is still not completely clear whether hiPS cells are equivalent to hES cells. Recent work demonstrates hotspots of aberrant epigenomic reprogramming in hiPS cells (Lister, R., et al., 2011).

Pluripotent, embryonic stem cells originate as inner cell mass (ICM) cells within a blastocyst. These stem cells can become any tissue in the body, excluding a placenta. Only cells from an earlier stage of the embryo, known as the morula, are totipotent, able to become all tissues in the body and the extraembryonic placenta
The European Commission has approved the first copycat version of an antibody-based drug, clearing the way for increased competition for the makers of multi-billion dollar biotechnology drugs to treat complex diseases

Tuesday’s final green light for Inflectra – which was developed by South Korea’s Celltrion and will be marketed by U.S. company Hospira – had been expected following a European Medicines Agency recommendation in June.
Hospira said the drug for treating rheumatoid arthritis and some other conditions would be launched throughout Europe “at the earliest opportunity taking into account any relevant patent protection”.
Inflectra is a so-called biosimilar version of Johnson & Johnson and Merck & Co’s Remicade.
http://www.reuters.com/article/2013/09/10/celltrion-hospira-europe-idUSL5N0H620R20130910
remicade= infliximab
Infliximab (INN; trade name Remicade) is a monoclonal antibody against tumour necrosis factor alpha (TNF-α) used to treat autoimmune diseases. Remicade is marketed by Janssen Biotech, Inc. (formerly Centocor Biotech, Inc.) in the USA, Mitsubishi Tanabe Pharma in Japan, Xian Janssen in China, and Schering-Plough (now part of Merck & Co) elsewhere.[1] In 2013, two biosimilars were submitted for approval in Europe, by Hospiraand Celltrion Healthcare.[2]
Infliximab was approved by the U.S. Food and Drug Administration (FDA) for the treatment of psoriasis, Crohn’s disease, ankylosing spondylitis, psoriatic arthritis, rheumatoid arthritis, and ulcerative colitis. Infliximab won its initial approval by the FDA for the treatment of Crohn’s disease in August 1998.[3]
Infliximab works by binding to TNF-α. TNF-α is a chemical messenger (cytokine) and a key part of the autoimmune reaction. In rheumatoid arthritis, infliximab seems to work by preventing TNF-α from binding to its receptor in the cell.
Infliximab is an artificial antibody. It was originally developed in mice as a mouse antibody. Because humans have immune reactions to mouse proteins, the mouse common domains were replaced with similar human antibody domains. Because the antibodies were produced from one cell grown into a clone of identical cells, it is called a monoclonal antibody. Furthermore, as a combination of mouse and human antibody amino acid sequences, it is called a chimeric monoclonal antibody.
Infliximab was developed by Junming Le and Jan Vilcek at New York University School of Medicine and developed by Centocor, (now Janssen Biotech, Inc.)[4]
In the United States, Infliximab can cost $19,000 to $22,000 a year per patient wholesale, according to Centocor.[5]
Other monoclonal antibodies targeting TNF-α are golimumab (Simponi), adalimumab(Humira), and certolizumab pegol (Cimzia). Etanercept also binds and inhibits the action of TNF-α, but is not a monoclonal antibody (it is instead a fusion of TNF-receptor and anantibody constant region).[6]
Infliximab is administered by intravenous infusion, typically at six- to eight-week intervals, at a clinic or hospital. It cannot be administered orally because the digestive system would destroy the drug.[7]

- “Remicade Becomes First Anti-TNF Biologic Therapy to Treat One Million Patients Worldwide” (Press release).Johnson & Johnson. November 6, 2007. Retrieved 2009-11-14.
- ^ George, John (June 28, 2013). “Billion-dollar biotech drug may soon have biosimilar competition”. Philadelphia Business Journal. Retrieved June 27, 2013.
- ^ “Infliximab Product Approval Information – Licensing Action”.Drugs@FDA. U.S. Food and Drug Administration (FDA). Retrieved 2009-11-14.
- ^ Knight DM, Trinh H, Le J et al. (November 1993). “Construction and initial characterization of a mouse-human chimeric anti-TNF antibody”. Mol. Immunol. 30 (16): 1443–53.doi:10.1016/0161-5890(93)90106-L. PMID 8232330.
- ^ “Priced out of pain relief; Insurers balk at high costs of promising new treatments”, Victoria Colliver, San Francisco Chronicle, May 8, 2007
- ^ Peppel, K; et al. (1991). “A tumor necrosis factor (TNF) receptor-IgG heavy chain chimeric protein as a bivalent antagonist of TNF activity”. J. Exp. Med. 174 (6): 1483–9.doi:10.1084/jem.174.6.1483. PMC 2119031.PMID 1660525.
- ^ Steinhilber, D; Schubert-Zsilavecz, M; Roth, HJ (2005). “Molekülstruktur und biologische Eigenschaften”. Medizinische Chemie (in German) (1 ed.). Stuttgart: Deutscher Apothekerverlag. p. 5. ISBN 3-7692-3483-9.
Sun, Reddys, Bharat Biotech, 3 Indian Companies among Best Company in an Emerging market–Scrip Awards 2013

Shortlist for the SCRIP Awards 2013.
http://www.scripintelligence.com/awards/categories/
Deciding on a shortlist from so many deserving entries was never going to be an easy process for our independent judging panel, but they rose to the challenge and this list represents the best of the best.
Best Company in an Emerging Market – Sponsored by Clinigen Group
- Bharat Biotech – India
- Dr Reddy’s Laboratories – India
- Sphaera Pharma – Singapore
- Sun Pharmaceutical Industries – India
- WuXi AppTec – China
Best Technological Development in Clinical Trials
- ArisGlobal’s Total Clinical
- Covance’s Xcellerate
- ICON’s ICONIK Monitoring for Patient Safety
- INC Research’s Trusted Process
- PPD’s real-time data offering
- Quintiles’ Infosario Safety
Best Partnership Alliance
- AstraZeneca with Bristol-Myers Squibb and Amylin in diabetes
- AstraZeneca and LegoChem to develop two compounds as a combination antibacterial
- Drugdev.org for The Investigator Databank with Janssen R&D, Eli Lilly, Merck & Co and Pfizer
- Roche with Isis Pharmaceuticals for antisense drugs in Huntington’s disease
- Vaxxas with Merck & Co for the Nanopatch vaccine platform
- WuXi AppTec with MedImmune for autoimmune and inflammatory diseases
Financing Deal of the Year
- Clinigen’s Initial Public Offering on AIM
- Elcelyx Therapeutics’ $20 million series C financing
- e-Therapeutics’ fundraising of £40 million on AIM
- Karolinska Development financing through option deal with Rosetta Capital Partners
- Mesoblast’s equity financing of Aus$170m
Best Advance in an Emerging Market
- Bharat Biotech’s development of low-cost rotavirus vaccine Rotavac for emerging markets
- Janssen’s TB treatment program for Sirtuto (bedaquiline) in emerging markets
- Novartis’s Jian Kang Kuai Che healthcare project in China
- Roche’s collaboration with Ascletis for hepatitis C treatments in China
Clinical Advance of the Year – Sponsored by Quintiles
- Galapagos’s Phase IIa study of the JAK1 inhibitor GLPG0634 in rheumatoid arthritis
- Genmab and Janssen Biotech’s Phase I/II study of daratumumab in multiple myeloma
- Janssen Research & Development/Merck’s PURSUIT clinical program of Simponi (golimumab) in ulcerative colitis
- Mundipharma’s (ReSearch Pharmaceutical Services) RELOXYN-Study of oxycodone/naloxone FDC for restless legs syndrome
- Novartis’s Gilenya’s effect on brain volume loss in TRANSFORMS, FREEDOMS and FREEDOMS II
- Regeneron Pharmaceuticals and Sanofi’s Phase IIa study dupilumab in in asthma
Licensing Deal of the Year
- Allergan and Molecular Partners for the development and commercialization of DARPin products for ophthalmic diseases
- AstraZeneca and Horizon Discovery for the development and commercialization of the HD-001 kinase target program for multiple cancer types
- Clinigen and Theravance for commercialization of Vibativ (telavancin) in Europe
- Genentech and AC Immune and for the development and commercialization of anti-Tau antibodies for Alzheimer’s disease
- Janssen Biotech and Genmab for the development and commercialization of daratumumab
- Pfizer and AstraZeneca for the over-the-counter marketing of Nexium (esomeprazole)
Executive of the Year
- Harvey Berger, chairman and chief executive officer of ARIAD Pharmaceuticals
- Joe Jimenez, chief executive officer of Novartis
- Josef von Rickenbach, chairman and chief executive officer of PAREXEL
- Patrik de Haes, chief executive officer of ThromboGenics
- Phil Lee, president and chief executive officer of PHT
- Roch Doliveux, chairman and chief executive officer of UCB
Biotech Company of the Year
- Ablynx
- ARIAD Pharmaceuticals
- Galapagos
- Genmab
- Prosensa
- ThromboGenics
Best Contract Research Organization
- ClinTec International
- Covance
- ICON
- INC Research
- PPD
- Quintiles
Management Team of the Year
- Beximco Pharmaceuticals’ management team
- Prosensa’s management team
- Regeneron Pharmaceuticals’ CEO Leonard S Schleifer and CSO George D Yancopoulos
Best New Drug – Sponsored by INC Research
- Algeta and Bayer’s Xofigo (radium Ra223 dichloride)
- ARIAD Pharmaceuticals’ Iclusig (ponatinib)
- Novartis’ Bexsero (meningococcal group B vaccine)
- ThromboGenics/Alcon’s Jetrea (ocriplasmin)
- Zealand Pharma’s Lyxumia (lixisenatide)
Pharma Company of the Year – Sponsored by ICON
- Amgen
- Astellas
- Dr Reddy’s Laboratories
- Sun Pharmaceutical Industries
- Vifor Pharma (Galenica)
