



| Patent ID
|
Patent Title
|
Submitted Date
|
Granted Date
|
|---|---|---|---|
| US2016108123 | ANTIBODY MOLECULES TO PD-L1 AND USES THEREOF |
2015-10-13
|
2016-04-21
|
| US2014343086 | COMPOUNDS AND COMPOSITIONS FOR INHIBITING THE ACTIVITY OF ABL1, ABL2 AND BCR-ABL1 |
2014-07-31
|
2014-11-20
|
| US8829195 | Compounds and compositions for inhibiting the activity of ABL1, ABL2 and BCR-ABL1 |
2013-05-13
|
2014-09-09
|
FLAGS AND HITS
 DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
Join me on Linkedin
Join me on Researchgate
Join me on Facebook
 FACEBOOK
...................................................................Join me on twitter
FACEBOOK
...................................................................Join me on twitter
 ..................................................................Join me on google plus
..................................................................Join me on google plus
 Googleplus
Googleplus
FACEBOOK
...................................................................Join me on twitter
..................................................................Join me on google plus
GoogleplusMYSELF
DR ANTHONY MELVIN CRASTO Ph.D ( ICT, Mumbai)
, INDIA
36Yrs Exp. in the feld of Organic Chemistry,Working for AFRICURE PHARMA as ADVISOR earlier with GLENMARK PHARMA at Navi Mumbai, INDIA. Serving chemists around the world. Helping them with websites on Chemistry.Million hits on google,
NO ADVERTISEMENTS , ACADEMIC , NON COMMERCIAL SITE, world acclamation from industry, academia, drug authorities for websites, blogs and educational contribution, ........amcrasto@gmail.com..........+91 9323115463, Skype amcrasto64


New ICH Guidelines: ICH Q13 on Conti Manufacturing and ICH Q14 on AQbD
DRUG REGULATORY AFFAIRS INTERNATIONAL
![]()
New ICH Guidelines:
*ICH Q13* on Continuous Manufacturing &![]() 🎛
🎛![]() 🎚
🎚
*ICH Q14* on ATP – QbD (Analytical target profile and quality by design)![]() ⚗
⚗![]() ⏱
⏱
New ICH Guidelines: ICH Q13 on Conti Manufacturing and ICH Q14 on AQbD
In a press release from 22 June the International Council for Harmonisation (ICH) has announced that they will prepare new topics for the future. The Assembly agreed to begin working on two new topics for ICH harmonisation:
Analytical Procedure Development and Revision of Q2(R1) Analytical Validation (Q2(R2)/Q14)
and
Continuous Manufacturing (Q13)
The long anticipated revision of ICH Q2(R1) “Guideline on Validation of Analytical Procedures: Text and Methodology” has been approved and the work plan is scheduled to commence in Q3 2018. It is intended that the new guidelines will be consistent with ICH Q8(R2), Q9, Q10, Q11 and Q12 .
The AQbD approach is very important to collect information in order…
View original post 154 more words
Rebamipide, ребамипид , ريباميبيد ,瑞巴派特 ,

Rebamipide
- Molecular FormulaC19H15ClN2O4
- Average mass370.786 Da
- Monoisotopic mass370.072021 Da
OPC-12759
OPC-12759E
OPC-759
(±)-a-(p-Chlorobenzamido)-1,2-dihydro-2-oxo-4-quinolinepropionic acid
2-(4-Chlorobenzoylamino)-3-[2(1H)-quinolinon-4-yl]propionic acid
4-Quinolinepropanoic acid, α-[(4-chlorobenzoyl)amino]-1,2-dihydro-2-oxo- [ACD/Index Name]
4-quinolinepropanoic acid, α-[(4-chlorobenzoyl)amino]-2-hydroxy-
6454
CAS 90098-04-7 [RN]
a-[(4-Chlorobenzoyl)amino]-1,2-dihydro-2-oxo-4-quinolinepropanoic acid
LR583V32ZR
UNII:LR583V32ZR
ребамипид [Russian] [INN]
ريباميبيد [Arabic] [INN]
瑞巴派特 [Chinese] [INN]
(±)-2-(4-CHLOROBENZOYLAMINO)-3-(2(1H)-QUINOLINON-4-YL)-PROPIONIC ACID
obtain the white powder from dimethylformamide-water with its hemihydrate m.p. being 288-290°C (decomposition).
(-)-Configuration: from dimethylformamide to give colorless needles, mp 305~306 °C (decomposition). [α] D20-116.7 ° (C = 1.0, dimethylformamide).
(+)-Configuration: from dimethylformamide to give colorless needles, mp 305~306 °C (decomposition). [α] D20 + 116.9 ° (C = 1.0, dimethylformamide).
(-)-Configuration: from dimethylformamide to give colorless needles, mp 305~306 °C (decomposition). [α] D20-116.7 ° (C = 1.0, dimethylformamide).
(+)-Configuration: from dimethylformamide to give colorless needles, mp 305~306 °C (decomposition). [α] D20 + 116.9 ° (C = 1.0, dimethylformamide).
Rebamipide is a quinolone derivative that was launched in 1990 by Otsuka in Japan for the oral treatment of Helicobacter pylori-induced gastric inflammation after eradication therapy and peptic ulcer
Title: Rebamipide
CAS Registry Number: 90098-04-7
CAS Name: a-[(4-Chlorobenzoyl)amino]-1,2-dihydro-2-oxo-4-quinolinepropanoic acid
Additional Names: (±)-a-(p-chlorobenzamido)-1,2-dihydro-2-oxo-4-quinolinepropionic acid; 2-(4-chlorobenzoylamino)-3-[2(1H)-quinolinon-4-yl]propionic acid; proamipide
Manufacturers’ Codes: OPC-12759
Trademarks: Mucosta (Otsuka)
Molecular Formula: C19H15ClN2O4
Molecular Weight: 370.79
Percent Composition: C 61.55%, H 4.08%, Cl 9.56%, N 7.56%, O 17.26%
Literature References: Gastric cytoprotectant. Prepn: M. Uchida et al., DE 3324034; eidem, US 4578381; (1984, 1986 both to Otsuka). Synthesis and pharmacology: M. Uchida et al., Chem. Pharm. Bull. 33, 3775 (1985); of enantiomers: eidem, ibid. 35, 853 (1987). Antiulcer activity in rats: K. Yamasaki et al., Eur. J. Pharmacol. 142, 23 (1987); K. Yamasaki et al., Jpn. J. Pharmacol. 49,441 (1989). HPLC determn in plasma and urine: Y. Shioya, T. Shimizu, J. Chromatogr. 434, 283 (1988).
Properties: White powder from DMF-water, mp 288-290° (dec) as hemihydrate.
Melting point: mp 288-290° (dec) as hemihydrate
Derivative Type: (-)-Form
Properties: Colorless needles from DMF, mp 305-306° (dec). [a]D20 -116.7° (c = 1.0 in DMF).
Melting point: mp 305-306° (dec)
Optical Rotation: [a]D20 -116.7° (c = 1.0 in DMF)
Derivative Type: (+)-Form
Properties: Colorless needles from DMF, mp 305-306° (dec). [a]D20 +116.9° (c = 1.0 in DMF).
Melting point: mp 305-306° (dec)
Optical Rotation: [a]D20 +116.9° (c = 1.0 in DMF)
Therap-Cat: Antiulcerative.
Keywords: Antiulcerative; Cytoprotectant (Gastric).
Rebamipide has been investigated for the treatment of Stomach Ulcer, Keratoconjunctivitis Sicca, and Gastric Adenoma and Early Gastric Cancer.
Rebamipide is a quinolinone derivative that stimulates endogenous PGE2 generation in gastric mucosa, enhancing gastric mucosal defense in a COX-2-dependent manner.
Rebamipide has been shown to inhibit the production of reactive oxygen species and to decrease cytokine release induced by H. pylori infection.
A daily oral dose of 100 mg/kg was found to be protective against the development of pyloric channel ulcers in Mongolian gerbils infected with H. pylori.
In addition to the stomach, rebamipide can also enhance secretion of mucin covering the conjunctiva and cornea, which is important for tear film adhesion.
Rebamipide, a gastroprotective drug, was developed in Japan and was proven to be superior to cetraxate, the former most prescribed drug of the same category, in 1989 in the treatment for gastric ulcers. The initially discovered basic mechanisms of action of rebamipide included its action as a prostaglandin inducer and oxygen free-radical scavenger. In the last 5 years, several basic and clinical studies have been performed for functional dyspepsia, chronic gastritis, NSAID-induced gastrointestinal injuries, gastric ulcer following eradication therapy for Helicobacter pylori, gastric ulcer after endoscopic surgery and ulcerative colitis. In addition, several molecules have been identified as therapeutic targets of rebamipide to explain its pleiotropic pharmacological actions.
Rebamipide has been shown to inhibit the production of reactive oxygen species and to decrease cytokine release induced by H. pylori infection.
A daily oral dose of 100 mg/kg was found to be protective against the development of pyloric channel ulcers in Mongolian gerbils infected with H. pylori.
In addition to the stomach, rebamipide can also enhance secretion of mucin covering the conjunctiva and cornea, which is important for tear film adhesion.
Rebamipide, a gastroprotective drug, was developed in Japan and was proven to be superior to cetraxate, the former most prescribed drug of the same category, in 1989 in the treatment for gastric ulcers. The initially discovered basic mechanisms of action of rebamipide included its action as a prostaglandin inducer and oxygen free-radical scavenger. In the last 5 years, several basic and clinical studies have been performed for functional dyspepsia, chronic gastritis, NSAID-induced gastrointestinal injuries, gastric ulcer following eradication therapy for Helicobacter pylori, gastric ulcer after endoscopic surgery and ulcerative colitis. In addition, several molecules have been identified as therapeutic targets of rebamipide to explain its pleiotropic pharmacological actions.
Rebamipide, an amino acid derivative of 2-(1H)-quinolinone, is used for mucosal protection, healing of gastroduodenal ulcers, and treatment of gastritis. It works by enhancing mucosal defense, scavenging free radicals, and temporarily activating genes encoding cyclooxygenase-2.
Rebamipide is used in a number of Asian countries including Japan (marketed as Mucosta), South Korea, China[1] and India (where it is marketed under the trade name Rebagen). It is also approved in Russia under the brand name Rebagit.[2] It is not approved by the Food and Drug Administration for use in the United States.
Studies have shown that rebamipide can fight the damaging effects of NSAIDs on the GIT mucosa, and more recently, the small intestine.[citation needed] It has also been studied for the treatment of Behçet’s disease.[3] It was shown to successfully treat pouchitis in a single-N study after first-line therapies for the condition were unsuccessful.[4] Some studies have shown effectiveness in presbyacusis(age-related hearing loss).[citation needed]
It has also been shown to alleviate signs and symptoms of dry eyes in a randomised controlled trial although this is not yet widely available clinically.[5]
SYN
Rebamipide (CAS NO.: 111911-87-6), with its systematic name of 4-Quinolinepropanic acid, alpha-((4-chlorobenzoyl)amino)-1,2-dihydro-2-oxo-, (+-)-, could be produced through many synthetic methods.
Following is one of the reaction routes:

4-(Bromomethyl)quinolin-2(1H)-one (I) could react with hot phosphorus oxychloride to produce a mixture of 4-(bromomethyl)-2-chloroquinoline (II) and 2-chloro-4-(chloromethyl)quinoline (III), and then the mixture without separation is ondensed with 2(S)-isopropyl-3,6-dimethoxy-2,5-dihydropyrazine (IVs) in the presence of butyllithium in hexane, affording (-)-2-chloro-4-[6(S)-isopropyl-2,5-dimethoxy-3,6-dihydropyrazin-3(R)-yl methyl]quinoline (Vr). The hydrolysis of (Vr) with HCl produces 3-(2-chloroquinolin-4-yl)-(R)-alanine methyl ester (VIr), which is treated with HCl and propylene oxide to afford 3-(2-oxo-2,3-dihydroquinolin-4-yl)-(R)-alanine (VIIr). At last, this compound is acylated with 4-chlorobenzoyl chloride (VIII) by means of K2CO3in acetone, affording (R)-OPC-12759.

Figure 2 The synthetic route of Rebamipide.

DE 3324034; US 4578381 ABOVE
The condensation of 4-(bromomethyl)quinolin-2(1H)-one (I) with diethyl acetamidomalonate (II) by means of sodium ethoxide in refluxing ethanol gives ethyl 2-acetamido-2-(ethoxycarbonyl)-3-(2-oxo-1,2-dihydroquinolin-4yl)propionate (III), which is submitted to a decarboxylative hydrolysis with refluxing 20% HCl yielding 3-(2-oxo-1,2-dihydroquinolin-4yl)alanine (IV). Finaily this compound is acylated with 4-chlorobenzoyl chloride by means of K2CO3 in acetone water.
SYN

Chem Pharm Bull 1991,39(11),2906 ABOVE
The synthesis of (R)- and (S)-isomers of OPC-12759 has been described: These optical isomers can be obtained in three different ways: 1) The reaction of 4-(bromomethyl)quinolin-2(1H)-one (I) with hot phosphorus oxychloride gives a mixture of 4-(bromomethyl)-2-chloroquinoline (II) and 2-chloro-4-(chloromethyl)quinoline (III), which, without separation, is condensed with 2(S)-isopropyl-3,6-dimethoxy-2,5-dihydropyrazine (IVs) by means of butyllithium in hexane, yielding (-)-2-chloro-4-[6(S)-isopropyl-2,5-dimethoxy-3,6-dihydropyrazin-3(R)-yl methyl]quinoline (Vr). The hydrolysis of (Vr) with HCl affords 3-(2-chloroquinolin-4-yl)-(R)-alanine methyl ester (VIr), which is treated with HCl and propylene oxide to give 3-(2-oxo-2,3-dihydroquinolin-4-yl)-(R)-alanine (VIIr). Finally, this compound is acylated with 4-chlorobenzoyl chloride (VIII) by means of K2CO3 in acetone, affording (R)-OPC-12759.
SYN

 3) The methylation of 3-(2-oxo-1,2-dihydroquinolin-4-yl)-(R,S)-alanine (IX) with SOCl2 and methanol yields the corresponding methyl ester (X), which is submitted to optical resolution with D-(-)-mandelic acid, affording adducts (XII) and (XIII). The hydrolytic treatment of (XII) and (XIII) with HCl and propylene oxide finally yields isomers (VIIr) and (VIIs), already obtained. Racemic OPC-12759 can also be resolved into its optical isomers by treatment with brucine and fractionated crystallization.
3) The methylation of 3-(2-oxo-1,2-dihydroquinolin-4-yl)-(R,S)-alanine (IX) with SOCl2 and methanol yields the corresponding methyl ester (X), which is submitted to optical resolution with D-(-)-mandelic acid, affording adducts (XII) and (XIII). The hydrolytic treatment of (XII) and (XIII) with HCl and propylene oxide finally yields isomers (VIIr) and (VIIs), already obtained. Racemic OPC-12759 can also be resolved into its optical isomers by treatment with brucine and fractionated crystallization.
Rebamipide
-
- Synonyms:Proamipide
- ATC:A02BX
- Use:ulcer therapeutic
- Chemical name:α-[(4-chlorobenzoyl)amino]-1,2-dihydro-2-oxo-4-quinolinepropanoic acid
- Formula:C19H15ClN2O4
- MW:370.79 g/mol
- CAS-RN:90098-04-7
- LD50:572 mg/kg (M, i.v.);
700 mg/kg (R, i.v.);
>2 g/kg (dog, p.o.)
Substance Classes
Synthesis Path
Substances Referenced in Synthesis Path
| CAS-RN | Formula | Chemical Name | CAS Index Name |
|---|---|---|---|
| 39098-85-6 | C4H5ClO2 | acetoacetyl chloride | Butanoyl chloride, 3-oxo- |
| 62-53-3 | C6H7N | aniline | Benzenamine |
| 4876-10-2 | C10H8BrNO | 4-(bromomethyl)-2(1H)-quinolinone | 2(1H)-Quinolinone, 4-(bromomethyl)- |
| 128-08-5 | C4H4BrNO2 | N-bromosuccinimide | 2,5-Pyrrolidinedione, 1-bromo- |
| 122-01-0 | C7H4Cl2O | 4-chlorobenzoyl chloride | Benzoyl chloride, 4-chloro- |
| 1068-90-2 | C9H15NO5 | diethyl acetamidomalonate | Propanedioic acid, (acetylamino)-, diethyl ester |
| 4900-38-3 | C19H22N2O6 | ethyl 2-acetamido-2-(ethoxycarbonyl)-3-(2-oxo-1,2-dihydroquinolin-4-yl)propionate | Propanedioic acid, (acetylamino)[(1,2-dihydro-2-oxo-4-quinolinyl)methyl]-, diethyl ester |
| 5162-90-3 | C12H12N2O3 | 3-(2-oxo-1,2-dihydroquinolin-4-yl)alanine | 4-Quinolinepropanoic acid, α-amino-1,2-dihydro-2-oxo- |
| 102-01-2 | C10H11NO2 | 3-oxo-N-phenylbutanamide | Butanamide, 3-oxo-N-phenyl- |
Trade Names
| Country | Trade Name | Vendor | Annotation |
|---|---|---|---|
| J | Mucosta | Otsuka |
Formulations
- tabl. 100 mg
References
-
- Uchida, M. et al.: Chem. Pharm. Bull. (CPBTAL) 33, 3775 (1985).
- DOS 3 324 034 (Otsuka; appl. 7.4.1983; J-prior. 7.5.1982).
- GB 2 123 825 (Otsuka; appl. 7.5.1983; J-prior. 7.5.1982).
-
oral and parenteral formulations:
- JP 60 019 767 (Otsuka; appl. 7.11.1983).
PAPER
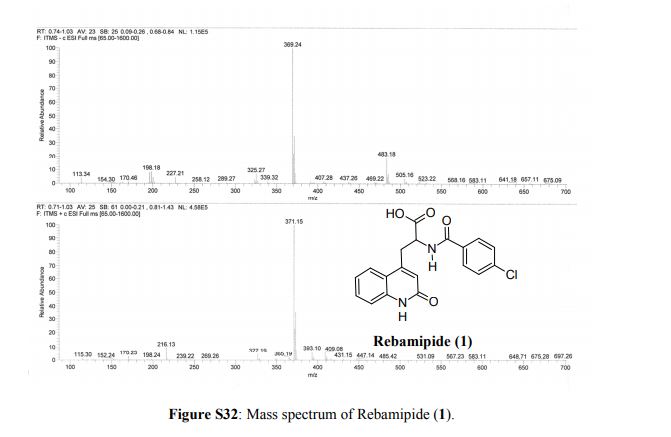
Magic Bullet! Rebamipide, a Superior Anti-ulcer and Ophthalmic Drug and Its Large-Scale Synthesis in a Single Organic Solvent via Process Intensification Using Krapcho Decarboxylation
https://pubs.acs.org/doi/10.1021/acs.oprd.7b00382#
Prashanth Kumar Babu, Mohan Reddy Bodireddy, Reshma Choudlu Puttaraju, Dnyaneshwar Vagare, Raghu Nimmakayala, Naresh Surineni, Madhusudana Rao Gajula*, and Pramod Kumar* 
Chemical Research Division, API R&D Centre, Micro Labs Ltd., Plot No.43-45, KIADB Industrial Area, fourth phase, Bommasandra-Jigani Link Road, Bommasandra, Bangalore 560 105, Karnataka, India
Org. Process Res. Dev., Article ASAP
DOI: 10.1021/acs.oprd.7b00382
Publication Date (Web): May 31, 2018
Copyright © 2018 American Chemical Society
*E-mail: pramodkumar@microlabs.in., *E-mail: gmadhusudanrao@yahoo.com.

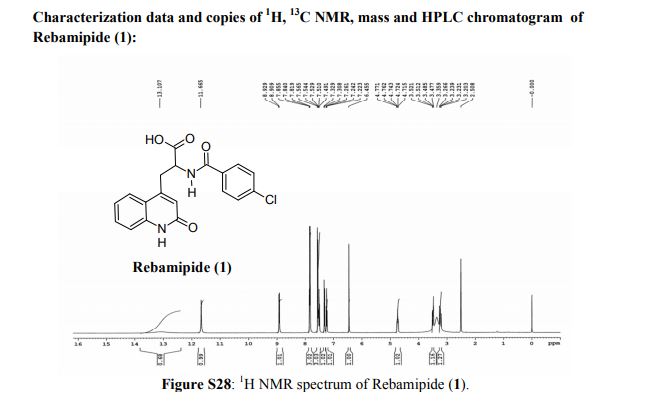
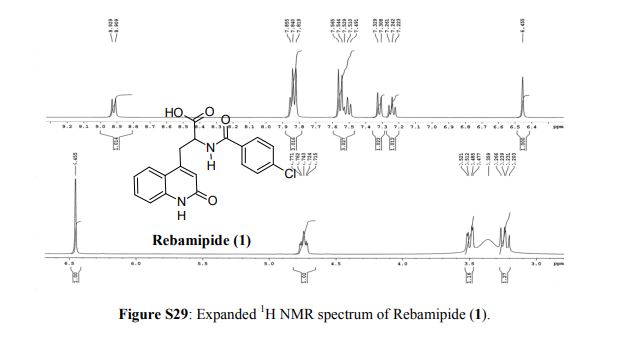
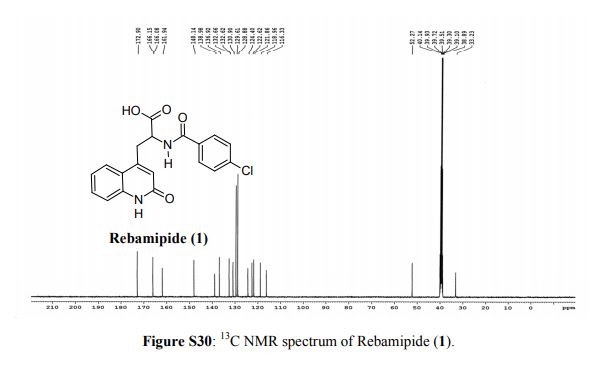
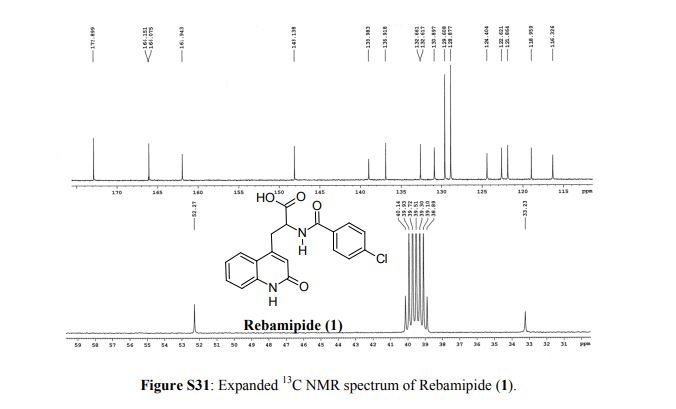
Rebamipide (1) is a superior drug compared to existing drugs for use in healing of peptic ulcers, gastrointestinal bleeding, and dyspepsia. It is also useful as an ophthalmic drug for the treatment of dry eye syndrome. Process intensification for its synthesis was achieved by (i) averting uncontrollable frothing using Krapcho decarboxylation instead of conventional acid hydrolysis, where uncontrollable frothing became chaotic, (ii) minimizing organic waste generation by using a single organic solvent, and (iii) avoiding anti-foaming agents (n-octanol, acetophenone) and acetic acid. With these trifling modifications, the overall yield of active pharmaceutical ingredient (API) was ≥83% with excellent purity (≥99.89%), and the process meets the metrics of “green” chemistry with an E-factor = 11.5. The developed hassle-free commercial process is viable for multi-kilogram synthesis of Rebamipide (1) as the key step, Krapcho decarboxylation is safe to run at 130–140 °C in DMSO, and it was proved to be effective by differential scanning calorimetry thermal screening studies. The characterization data of intermediates, process-related impurities, and API are reported. The carryover and process-related impurities were controlled efficiently. The present work can enhance the scope and worldwide adoptability of Rebamipide (1), which is currently limited to Asian countries.
https://pubs.acs.org/doi/suppl/10.1021/acs.oprd.7b00382/suppl_file/op7b00382_si_001.pdf
Articles
- Arakawa T, Watanabe T, Fukuda T, Yamasaki K, Kobayashi K (1995). “Rebamipide, novel prostaglandin-inducer accelerates healing and reduces relapse of acetic acid-induced rat gastric ulcer. Comparison with cimetidine”. Dig Dis Sci. 40 (11): 2469–72. doi:10.1007/BF02063257. PMID 7587834.
- Arakawa T, Kobayashi K, Yoshikawa T, Tarnawski A (1998). “Rebamipide: overview of its mechanisms of action and efficacy in mucosal protection and ulcer healing”. Dig Dis Sci. 43 (9 Suppl): 5S–13S. PMID 9753220.
- Tarnawski AS, Chai J, Pai R, Chiou SK (2004). “Rebamipide activates genes encoding angiogenic growth factors and Cox2 and stimulates angiogenesis: a key to its ulcer healing action?”. Dig Dis Sci. 49 (2): 202–9. doi:10.1023/B:DDAS.0000017439.60943.5c. PMID 15104358.
- Takumida M, Anniko M (2009). “Radical scavengers for elderly patients with age-related hearing loss”. Acta Otolaryngol. 129 (1): 36–44. doi:10.1080/00016480802008215. PMID 18607930.
References
- Jump up^ drugs.com
- Jump up^ “Russian State Register of Medicines. Registration Sertificate: Rebagit (rebamipide) Film-Coated Tablets” (in Russian). Retrieved 10 June 2017.
- Jump up^ Matsuda T, Ohno S, Hirohata S, Miyanaga Y, Ujihara H, Inaba G, Nakamura S, Tanaka S, Kogure M, Mizushima Y (2003). “Efficacy of rebamipide as adjunctive therapy in the treatment of recurrent oral aphthous ulcers in patients with Behcet’s disease: a randomised, double-blind, placebo-controlled study”. Drugs R D. 4 (1): 19–28. doi:10.2165/00126839-200304010-00002. PMID 12568631.
- Jump up^ http://www.wjgnet.com/1007-9327/12/656.pdf Archived October 20, 2013, at the Wayback Machine.
- Jump up^ Kinoshita, S.; K. Oshiden; S. Awamura; H. Suzuki; N. Nakamichi (2013). “A randomized, multicenter phase 3 study comparing 2% rebamipide (OPC-12759) with 0.1% sodium hyaluronate in the treatment of dry eye”. Ophthalmology. 120 (6): 1158–65. doi:10.1016/j.ophtha.2012.12.022. PMID 23490326.
 |
|
| Clinical data | |
|---|---|
| Trade names | Mucosta (JP), Rebagen (KR,CN, IN), Rebagit (RU) |
| AHFS/Drugs.com | International Drug Names |
| Routes of administration |
Oral (tablets) |
| ATC code | |
| Identifiers | |
| CAS Number | |
| PubChem CID | |
| IUPHAR/BPS | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEMBL | |
| Chemical and physical data | |
| Formula | C19H15ClN2O4 |
| Molar mass | 370.786 g/mol |
| 3D model (JSmol) | |
/////////Rebamipide, UNII:LR583V32ZR, ребамипид , ريباميبيد ,瑞巴派特 , OPC-12759 , OPC-12759E , OPC-759 , OPC 12759 , OPC 12759E , OPC 759 , OTSUKA, JAPAN 1990
OC(=O)C(CC1=CC(O)=NC2=CC=CC=C12)NC(=O)C1=CC=C(Cl)C=C1
Alfuzosin, 塩酸アルフゾシン
Alfuzosin
- Molecular FormulaC19H27N5O4
- Average mass389.449 Da
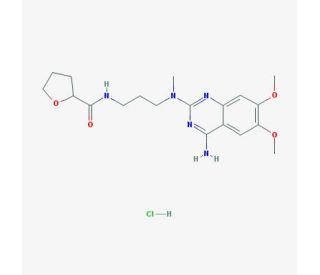
N-{3-[(4-Amino-6,7-dimethoxy-2-quinazolinyl)(methyl)amino]propyl}tetrahydro-2-furancarboxamide
N-{3-[(4-amino-6,7-dimethoxyquinazolin-2-yl)(methyl)amino]propyl}tetrahydrofuran-2-carboxamide
SL 77499-10
UNII:90347YTW5F
Urion
Xatral
2-furancarboxamide, N-[3-[(4-amino-6,7-dimethoxy-2-quinazolinyl)methylamino]propyl]tetrahydro-
5357
cas 81403-80-7 [RN]
| CAS: | 81403-68-1 HCL SALT |
90347YTW5F
塩酸アルフゾシン
Title: Alfuzosin
CAS Registry Number: 81403-80-7
CAS Name: N-[3-[(4-Amino-6,7-dimethoxy-2-quinazolinyl)methylamino]propyl]tetrahydro-2-furancarboxamide
Additional Names: N1-(4-amino-6,7-dimethoxyquinazol-2-yl)-N1-methyl-N2-(tetrahydrofuroyl-2)-propylenediamine
Manufacturers’ Codes: SL-77.499
Molecular Formula: C19H27N5O4
Molecular Weight: 389.45
Percent Composition: C 58.60%, H 6.99%, N 17.98%, O 16.43%
Literature References: a1-Adrenoceptor antagonist structurally similar to prazosin, q.v. Prepn: P. M. J. Manoury, DE 2904445; idem, US 4315007 (1979, 1982 both to Synthelabo); and antihypertensive activity in rats: P. M. Manoury et al., J. Med. Chem. 29,19 (1986). Pharmacology: A. G. Ramage, Eur. J. Pharmacol. 129, 307 (1986). HPLC determn in biological fluids: P. Guinebault et al., J. Chromatogr. 353, 361 (1986). Pharmacology in humans: A. H. Deering, Br. J. Clin. Pharmacol. 25, 417 (1988). Clinical evaluation in essential hypertension: S. Leto Di Priolo et al., Eur. J. Clin. Pharmacol. 35, 25 (1988); A. K. Ghosh, S. Ghosh, Ger. Cardiovasc. Med. 1, 81 (1988). Clinical trial in benign prostatic hyperplasia (BPH): C. G. Roehrborn et al., BJU Int. 92, 257 (2003). Review of clinical experience in BPH: D. M. Weiner, F. C. Lowe, Expert Opin. Pharmacother. 4, 2057-2063 (2003).
Alfuzosin hydrochloride (CAS 81403-68-1)
Derivative Type: Hydrochloride
CAS Registry Number: 81403-68-1
Manufacturers’ Codes: SL-77.499-10
Trademarks: Mittoval (Schering AG); Urion (Zambon); UroXatral (Sanofi-Synthelabo); Xatral (Sanofi-Synthelabo)
Molecular Formula: C19H27N5O4.HCl
Molecular Weight: 425.91
Percent Composition: C 53.58%, H 6.63%, N 16.44%, O 15.03%, Cl 8.32%
Properties: Crystals from ethanol + ether, mp 225° (Manoury, 1986), also reported earlier as mp 235° (dec) (Manoury, 1982). pKa 8.13.
Melting point: mp 225° (Manoury, 1986); mp 235° (dec) (Manoury, 1982)
pKa: pKa 8.13
Therap-Cat: Antihypertensive. In treatment of benign prostatic hypertrophy.
Keywords: Antihypertensive; Quinazoline Derivatives; Antiprostatic Hypertrophy; a-Adrenergic Blocker.
Alfuzosin (INN, provided as the hydrochloride salt) is a pharmaceutical drug of the α1 blocker class. As an antagonist of the α1adrenergic receptor, it works by relaxing the muscles in the prostate and bladder neck, making it easier to urinate. It is thus used to treat benign prostatic hyperplasia (BPH).[1]
Alfuzosin is marketed in the United States by Sanofi Aventis under the brand name Uroxatral and elsewhere under the tradenames Xat, Xatral, Prostetrol and Alfural. Alfuzosin was approved by the U.S. FDA for treatment of BPH in June 2003.
Side effects
The most common side effects are dizziness (due to postural hypotension), upper respiratory tract infection, headache, fatigue, and abdominal disturbances. Side effects include stomach pain, heartburn, and congested nose.[2] Adverse effects of alfuzosin are similar to that of tamsulosin with the exception of retrograde ejaculation.[3]
Contraindications
Alfuzosin should be used with caution in patients with severe renal insufficiency, and should not be prescribed to patients with a known history of QT prolongation who are taking medications known to prolong the QT interval.
Chemistry
Alfuzosin contains a stereocenter and is therefore chiral. There are two enantiomeric forms, (R)-alfuzosin and (S)-alfuzosin. The drug is used as a racemate, (RS)-alfuzosin, a 1: 1 mixture of the (R)- and (S)-forms.[4]
| Enantiomers of alfuzosin | |
|---|---|
-Alfuzosin_Structural_Formula_V2.svg) CAS number: 123739-69-5 |
-Alfuzosin_Structural_Formula_V2.svg) CAS number.: 123739-70-8 |
Alfuzosin
-
- ATC:G04CA01
- Use:antihypertensive, α1-adrenoceptor antagonist, α-blocker, treatment of benign prostatic hypertrophy (BPH)
- Chemical name:(±)-N-[3-[(4-amino-6,7-dimethoxy-2-quinazolinyl)methylamino]propyl]tetrahydro-2-furancarboxamide
- Formula:C19H27N5O4
- MW:389.46 g/mol
- CAS-RN:81403-80-7
Derivatives
monohydrochloride
- Formula:C19H27N5O4 • HCl
- MW:425.92 g/mol
- CAS-RN:81403-68-1
Substance Classes
Synthesis Path
Substances Referenced in Synthesis Path
| CAS-RN | Formula | Chemical Name | CAS Index Name |
|---|---|---|---|
| 23680-84-4 | C10H10ClN3O2 | 4-amino-2-chloro-6,7-dimethoxyquinazoline | 4-Quinazolinamine, 2-chloro-6,7-dimethoxy- |
| 5004-88-6 | C9H12N2O3 | 2-amino-4,5-dimethoxybenzamide | Benzamide, 2-amino-4,5-dimethoxy- |
| 541-41-3 | C3H5ClO2 | chloroformic acid ethyl ester | Carbonochloridic acid, ethyl ester |
| 72104-44-0 | C9H14N2O2 | 2-cyano-N-methyl-N-tetrahydrofuroylethylamine | 2-Furancarboxamide, N-(2-cyanoethyl)tetrahydro-N-methyl- |
| 27631-29-4 | C10H8Cl2N2O2 | 2,4-dichloro-6,7-dimethoxyquinazoline | Quinazoline, 2,4-dichloro-6,7-dimethoxy- |
| 28888-44-0 | C10H10N2O4 | 2,4-dihydroxy-6,7-dimethoxyquinazoline | 2,4(1H,3H)-Quinazolinedione, 6,7-dimethoxy- |
| 20357-25-9 | C9H9NO5 | 4,5-dimethoxy-2-nitrobenzaldehyde | Benzaldehyde, 4,5-dimethoxy-2-nitro- |
| 4959-60-8 | C9H10N2O5 | 4,5-dimethoxy-2-nitrobenzamide | Benzamide, 4,5-dimethoxy-2-nitro- |
| 28888-44-0 | C10H10N2O4 | 6,7-dimethoxyquinazoline-2,4-dione | 2,4(1H,3H)-Quinazolinedione, 6,7-dimethoxy- |
| 541-41-3 | C3H5ClO2 | ethyl chloroformate | Carbonochloridic acid, ethyl ester |
| 693-05-0 | C4H8N2 | 3-(methylamino)propanenitrile | Propanenitrile, 3-(methylamino)- |
| 81403-67-0 | C9H18N2O2 | N1-methyl-N2-tetrahydrofuroyltrimethylenediamine | 2-Furancarboxamide, tetrahydro-N-[3-(methylamino)propyl]- |
| 16874-33-2 | C5H8O3 | (±)-tetrahydrofuran-2-carboxylic acid | 2-Furancarboxylic acid, tetrahydro- |
| 167391-50-6 | C8H12O5 | tetrahydro-2-furancarboxylic acid anhydride with ethyl hydrogen carbonate | 2-Furancarboxylic acid, tetrahydro-, anhydride with ethyl hydrogen carbonate |
| 57-13-6 | CH4N2O | urea | Urea |
| 120-14-9 | C9H10O3 | veratraldehyde | Benzaldehyde, 3,4-dimethoxy- |
Trade Names
| Country | Trade Name | Vendor | Annotation |
|---|---|---|---|
| D | Alfunar | Apogepha | |
| Alfusin | TAD Pharma | ||
| Urion | Sanofi-Aventis | ||
| Uroxatral | Sanofi-Aventis | ||
| F | Urion | Zambon | |
| Xatral | Sanofi-Aventis | ||
| GB | Xatral | Sanofi-Aventis | |
| I | Mittoval | Sanofi-Aventis | |
| Xatral | Sanofi-Aventis |
Formulations
- film tabl. 2.5 mg; retard tabl. 10 mg (hydrochloride)
References
-
- Manoury, P.M. et al.: J. Med. Chem. (JMCMAR) 29, 19 (1986).
- US 4 315 007 (Synthelabo; 9.2.1982; F-prior. 6.2.1978, 29.12.1978).
- DE 2 904 445 (Synthelabo; appl. 16.8.1979; F-prior. 6.2.1978, 29.12.1978).
-
synthesis of 6,7-dimethoxyquinazoline-2,4-dione:
- Althuis, T.H.; Hess, H.J.: J. Med. Chem. (JMCMAR) 20, 146 (1977).
SYN
Mathias Scheer, “Alfuzosin tablets and synthesis.” U.S. Patent US20060062845, issued March 23, 2006.
Syn, DOI: 10.1021/jm00151a003 NB: (WO2009001369)

FTIR spectrum of alfuzosin hydrochloride
CLIP


Add the following:

C19H27N5O4·HCl ![]()
![]()
![]()
![]()
![]() 425.91
425.91
2-Furancarboxamide, N-[3-[(4-amino-6,7-dimethoxy-2-quinazolinyl)methylamino]propyl]tetrahydro-, monohydrochloride (±).
(±)-N-[3-[(4-Amino-6,7-dimethoxy-2-quinazolinyl)methylamino]propyl]tetrahydro-2-furamide monohydrochloride [81403-68-1].
[81403-68-1].
(±)-N-[3-[(4-Amino-6,7-dimethoxy-2-quinazolinyl)methylamino]propyl]tetrahydro-2-furamide monohydrochloride
» Alfuzosin Hydrochloride contains not less than 99.0 percent and not more than 101.0 percent of C19H27N5O4·HCl, calculated on the anhydrous basis.
Packaging and storage— Preserve in tight, well-closed containers, protected from light and humidity. Store at room temperature.
USP Reference standards  11
11 —
—
USP Alfuzosin Hydrochloride RS.
USP Alfuzosin System Suitability Mixture RS.
USP Alfuzosin Hydrochloride RS.
USP Alfuzosin System Suitability Mixture RS.
Identification—
B: It meets the requirements of the test for Chloride 191.
pH ![]() 791
791![]() : between 4.0 and 5.5
: between 4.0 and 5.5
Test solution: 20 mg per mL, in carbon dioxide-free water.
Optical rotation ![]() 781
781![]() :
: ![]() 0.10
0.10![]() to +0.10
to +0.10![]()
Test solution: 20 mg per mL, in carbon dioxide-free water.
Water, Method I 921: not more than 0.5%.
Residue on ignition 281: not more than 0.1%.
Related compounds—
Solution A— Dilute 5.0 mL of perchloric acid in 900 mL of water, adjust with 2 M sodium hydroxide solution to a pH of 3.5, and dilute with water to 1000 mL.
Mobile phase— Prepare a filtered and degassed mixture of Solution A, acetonitrile, and tetrahydrofuran (80:20:1). Make adjustments if necessary (see System Suitability under Chromatography 621).
System suitability solution— Dissolve an accurately weighed quantity of USP Alfuzosin System Suitability Mixture RS in Mobile phase, and dilute quantitatively with Mobile phase to obtain a solution containing about 0.4 mg per mL.
Test solution— Dissolve 40.0 mg of Alfuzosin Hydrochloride in Mobile phase, and dilute with Mobile phase to 100.0 mL.
Reference solution— Quantitatively dilute an accurately measured volume of the Test solution by a factor of 1000 with Mobile phase.
Chromatographic system (see Chromatography ![]() 621
621![]() )— The liquid chromatograph is equipped with a detector set at 254 nm and a 4.6-mm × 15-cm column that contains 5-µm packing L1. The flow rate is about 1.5 mL per minute. Chromatograph the System suitability solution, and record the peak responses as directed for Procedure: the peak-to-valley ratio is at least 5. [NOTE—The peak-to-valley ratio is determined as the ratio of the height above the baseline of the impurity A peak to the height above the baseline of the lowest point of the curve separating this impurity peak from the peak due to alfuzosin.]
)— The liquid chromatograph is equipped with a detector set at 254 nm and a 4.6-mm × 15-cm column that contains 5-µm packing L1. The flow rate is about 1.5 mL per minute. Chromatograph the System suitability solution, and record the peak responses as directed for Procedure: the peak-to-valley ratio is at least 5. [NOTE—The peak-to-valley ratio is determined as the ratio of the height above the baseline of the impurity A peak to the height above the baseline of the lowest point of the curve separating this impurity peak from the peak due to alfuzosin.]
Procedure— Separately inject equal volumes (about 10 µL) of the Reference solution and the Test solution, record the chromatograms, and measure the peak responses. Calculate the percentage of each impurity in the portion of Alfuzosin Hydrochloride taken by the formula:
100[rU / (1000 rS)]
in which 100 is the percentage conversion factor; rU is the peak response for any impurity obtained from the Test solution; 1000 is the dilution factor; and rS is the peak response for alfuzosin obtained from the Reference solution: the limits are as shown in the accompanying table. Disregard any peak with an area less than 0.05%.
| Compound | Relative Retention Time |
Limit (%) |
| Alfuzosin | 1.0 | — |
| Impurity A1 | 1.2 | * |
| Impurity D2 | 0.5 | 0.20 |
| Any individual unspecified impurity | — | 0.10 |
| Total impurities | — | 0.30 |
|
1 N-[3-[(4-Amino-6,7-dimethoxyquinazolin-2-yl)(methyl)amino]propyl]furan-2-carboxamide.
2 N-(4-Amino-6,7-dimethoxyquinazolin-2-yl)-N-methylpropane-1,3-diamine.
* Impurity A, a component of USP Alfuzosin System Suitability Mixture RS, is not a specified impurity.
|
||
Assay— Dissolve about 300 mg of Alfuzosin Hydrochloride, accurately weighed, in a mixture of 40 mL of anhydrous acetic acid and 40 mL of acetic anhydride. Titrate with 0.1 M perchloric acid, determining the endpoint potentiometrically. Each mL of 0.1 M perchloric acid is equivalent to 42.59 mg of C19H27N5O4·HCl. USP32
USP32
Auxiliary Information— Please check for your question in the FAQs before contacting USP.
| Topic/Question | Contact | Expert Committee |
| Monograph | Daniel K. Bempong, Ph.D. Senior Scientist 1-301-816-8143 |
(MDPS05) Monograph Development-Pulmonary and Steroids |
| Reference Standards | Lili Wang, Technical Services Scientist 1-301-816-8129 RSTech@usp.org |
USP32–NF27 Page 1449
Pharmacopeial Forum: Volume No. 34(1) Page 69
Chromatographic Column—
Chromatographic columns text is not derived from, and not part of, USP 32 or NF 27.
References
- Jump up^ Lepor, Herbert (2016). “Alpha-blockers for the Treatment of Benign Prostatic Hyperplasia”. Urologic Clinics of North America. 43 (3): 311–23. doi:10.1016/j.ucl.2016.04.009. PMC 2213889
 . PMID 27476124.
. PMID 27476124. - Jump up^ “Alfuzosin”. MedlinePlus. United States National Library of Medicine. April 15, 2016.
- Jump up^ Hills, Robert K; Liu, Chenli; Zeng, Guohua; Kang, Ran; Wu, Wenqi; Li, Jiasheng; Chen, Kang; Wan, Show P. (2015). “Efficacy and Safety of Alfuzosin as Medical Expulsive Therapy for Ureteral Stones: A Systematic Review and Meta-Analysis”. PLOS ONE. 10 (8): e0134589. doi:10.1371/journal.pone.0134589. ISSN 1932-6203. PMC 4526635 . PMID 26244843.
 This article incorporates text available under the CC BY 4.0 license.
This article incorporates text available under the CC BY 4.0 license. - Jump up^ Rote Liste Service GmbH (Hrsg.): Rote Liste 2017 – Arzneimittelverzeichnis für Deutschland (einschließlich EU-Zulassungen und bestimmter Medizinprodukte). Rote Liste Service GmbH, Frankfurt/Main, 2017, Aufl. 57, S. 159, ISBN 978-3-946057-10-9.
External links
- Uroxatral (alfuzosin HCl) Extended-Release Tablets Prescribing Information
- Alfuzosin (General information from the NIH)
 |
|
| Clinical data | |
|---|---|
| Pronunciation | /ælˈfjuːzoʊsɪn/ al-FEW-zoh-sin |
| Trade names | Uroxatral, others |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a64002 |
| Pregnancy category |
|
| Routes of administration |
By mouth (tablets) |
| ATC code | |
| Legal status | |
| Legal status | |
| Pharmacokinetic data | |
| Bioavailability | 49% |
| Protein binding | 82–90% |
| Metabolism | Liver (CYP3A4-mediated) |
| Elimination half-life | 10 hours |
| Excretion | Feces (69%) and Urine (24%) |
| Identifiers | |
| CAS Number | |
| PubChem CID | |
| IUPHAR/BPS | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEBI | |
| ChEMBL | |
| ECHA InfoCard | 100.108.671 |
| Chemical and physical data | |
| Formula | C19H27N5O4 |
| Molar mass | 389.46 g·mol−1 |
| 3D model (JSmol) | |
/////////////////塩酸アルフゾシン, Uroxatral, alfuzosin
COC1=C(OC)C=C2C(N)=NC(=NC2=C1)N(C)CCCNC(=O)C1CCCO1
Afloqualone, アフロクアロン
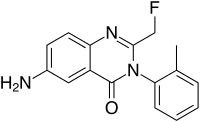
Afloqualone
| Molecular Formula: | C16H14FN3O |
|---|---|
| Molecular Weight: | 283.306 g/mol |
6-amino-2-(fluoromethyl)-3-(2-methylphenyl)quinazolin-4-one
HQ 495, C033541, QA-3735, UNII:CO4U2C8ORZ
4(3H)-Quinazolinone, 6-amino-2-(fluoromethyl)-3-(2-methylphenyl)- [ACD/Index Name]
4831
56287-74-2 [RN], アフロクアロン
Afloqualone; 56287-74-2; Arofuto; Aroft; Afloqualon; Afloqualone [INN:JAN]
Afloqualone (Arofuto) is a quinazolinone family GABAergic drug and is an analogue of methaqualone developed in the 1970s by a team at Tanabe Seiyaku.[1] It has sedative and muscle-relaxant effects resulting from its agonist activity at the β subtype of the GABAareceptor ,[2] and has had some clinical use, although it causes photosensitization as a side-effect that can cause skin problems such as dermatitis.[3]

PATENT
CN 106496145
PATENT
CN 106496144
https://patents.google.com/patent/CN106496144A/en
Example 1:
[0027] A-fluoro-quinolin-one process, comprising the steps of:
[0028] A. To the hydrogenation apparatus 10g 6- nitro-2- (fluoromethyl) -3- (2-methylphenyl) -4- (3H) -1,3- phthalazinone , 150ml acid content of 0.1 ~ 0.4N n-butanol solution of acetic acid, lg palladium ruthenium bimetallic catalyst, hydrogen pressure 0.02 ~ 0.4MPa, reaction temperature of 25-50 ° C, after 1 hour, filtered to give the filtrate ;
[0029] B. washed catalyst with ethanol, at normal temperature, under reduced pressure to obtain a solution ⑴;
[0030] C. was added to the filtrate and the solution ⑴ water, 0.1N sodium hydroxide solution was added, the pH adjusted to 10.2 to 11.0, and stirred at 50-60 ° C 0.5 h, cooled to room temperature and filtered to give the crude fluoro-quinolin-one;
[0031] D.-fluoro-quinolin per gram of the recrystallization solvent was added 5 ~ 15ml crude ketone, wherein the recrystallization solvent is a volume ratio of 1: 1: 0.2 in a solution of isopropanol (m), a solution of acid butyl ester (II ) and water mixture; crystallized at room temperature, filtered to give a fluorine methaqualone.
[0032] Example 2:
[0033] A-fluoro-quinolin-one process, comprising the steps of:
[0034] A. hydrogenation apparatus added to 20g 6- nitro _2_ (fluoromethyl) -3- (2_-methylphenyl) -4- (3-1,3-phthalazinone buckle, acid content of the acid-containing 240ml 0.1 ~ 0.4N ethanol solution of hydrochloric acid, lg palladium ruthenium bimetallic catalyst, hydrogen pressure 0.02 ~ 0.4MPa, reaction temperature of 25-50 ° C. after 0.5 hours the reaction was filtered to obtain filtrate;
[0035] B. washed catalyst with ethanol, at normal temperature, under reduced pressure to obtain a solution ⑴;
[0036] C. was added to the filtrate and the solution ⑴ water, 0.1N sodium hydroxide solution was added, the pH adjusted to 10.2 to 11.0, and stirred at 50-60 ° C 1 hour, cooled to room temperature and filtered to give the crude fluoro-quinolin-one;
[0037] D.-fluoro-quinolin added per gram of crude ketone was recrystallized from 5 ~ 15ml of the solvent, wherein the recrystallization solvent is a volume ratio of 1: o.2: methanol solution of i (m), an ethyl acetate solution (II ) and water mixture; crystallized at room temperature, filtered to give a fluorine methaqualone.
[0038] Example 3:
[0039] – quinolin-fluoro-one kind of process, comprising the steps of:
[0040] A. Add 5g 6- nitro apparatus _2_ hydride (fluoromethyl) -3- (2-methylphenyl) -4- (3-1,3-Perot phthalazinone, 80ml methanol containing an acid in an amount of 0.1 ~ 0.4N solution of sulfuric acid, lg palladium ruthenium bimetallic catalyst, hydrogen pressure 0.02 ~ 0.4MPa, reaction temperature of 25-50 ° C. after 1.5 hours the reaction was filtered to obtain filtrate;
[0041] B. the catalyst was washed with ethanol, normal temperature under reduced pressure to obtain a solution (the I);
[0042] C. was added to the filtrate and the solution (I) water, 0.1N sodium hydroxide solution was added, the pH adjusted to 10.2 to 11.0, and stirred at 50-60 ° C 1 hour, cooled to room temperature and filtered to give fluoro-quinolin-one Crude;
[0043] D. methaqualone fluorine per gram of crude product were added 5 ~ 15ml recrystallization solvent, wherein the recrystallization solvent is a volume ratio of 1: 0.2: 0.2 ethanol solution (m), carboxylic acid butyl ester (II) and water mixture; crystallization at room temperature, and filtered to give fluoro-quinolin-one.
PAPER
6-Amino-2-(fluoromethyl)-3-(2-methylphenyl)quinazolin-4(3H)-one
Acta Crystallographica, Section E: Structure Reports Online (2007), 63, (7), o3109
http://scripts.iucr.org/cgi-bin/paper?S1600536807026670
PAPER
Synthesis of the metabolites of afloqualone and related compounds
Chemical & pharmaceutical bulletin (1983), 31, (4), 1158-65.
Seven main metabolites (3-9) of afloqualone (1, 6-amino-2-fluoromethyl-3-(o-tolyl)-4 (3H)-quinazolinone and related 4 (3H)-quinazolinone derivatives were synthesized. The metabolites 4 and 5 containing a sulfur atom were prepared by the reaction of 6-acetamido-2-chloromethyl-3-(o-tolyl)-4 (3H)-quinazolinone (11) with NaSCH3 followed by oxidation with H2O2. Reaction of 11 and N-acetyl-L-cysteine gave the mercapturic acid-conjugated metabolite 6. Condensation of 2-fluoroacetamido-5-nitrobenzoic acid (19) and 2-amino-benzyl alcohol (20) with dicyclohexylcarbodiimide (DCC) in the presence of 1-hydroxy-benzotriazole afforded 2-fluoromethyl-3-(o-hydroxymethylphenyl)-6-nitro-4 (3H)-quinazolinone (21), which was converted to the metabolites 7 and 8. Treatment of the 2-bromomethyl-4 (3H)-quinazolinone (24) with AgBF4-H2O in dimethylsulfoxide (DMSO) gave the 2-hydroxymethyl metabolite 9. None of the main metabolites (2-9) showed significant central nervous system depressant activity
https://www.jstage.jst.go.jp/article/cpb1958/31/4/31_4_1158/_article
References
- Jump up^ US Patent 3966731 – 2-Fluoromethyl-3-o-tolyl-6-amino-4(3H)-quinazolinone
- Jump up^ Ochiai T, Ishida R. Pharmacological studies on 6-amino- 2-fluoromethyl- 3-(O-tolyl)- 4(3H)- quinazolinone (afloqualone), a new centrally acting muscle relaxant. (II) Effects on the spinal reflex potential and the rigidity. Japanese Journal of Pharmacology. 1982 Jun;32(3):427-38.
- Jump up^ Ishikawa T, Kamide R, Niimura M. Photoleukomelanodermatitis (Kobori) induced by afloqualone. Journal of Dermatology. 1994 Jun;21(6):430-3.
 |
|
| Clinical data | |
|---|---|
| AHFS/Drugs.com | International Drug Names |
| ATC code |
|
| Legal status | |
| Legal status |
|
| Identifiers | |
| CAS Number | |
| PubChem CID | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEMBL | |
| Chemical and physical data | |
| Formula | C16H14FN3O |
| Molar mass | 283.3 |
| 3D model (JSmol) | |
//////////////Afloqualone, HQ 495, アフロクアロン , C033541, QA-3735, UNII:CO4U2C8ORZ, 4831
CC1=CC=CC=C1N2C(=NC3=C(C2=O)C=C(C=C3)N)CF
Afloqualone
-
- ATC:M03A
- Use:muscle relaxant
- Chemical name:6-amino-2-(fluoromethyl)-3-(2-methylphenyl)-4(3H)-quinazolinone
- Formula:C16H14FN3O
- MW:283.31 g/mol
- CAS-RN:56287-74-2
- LD50:397 mg/kg (M, p.o.);
249 mg/kg (R, p.o.)
Derivatives
hydrochloride
- Formula:C16H14FN3O • xHCl
- MW:unspecified
- CAS-RN:56287-75-3
Substance Classes
Synthesis Path
Substances Referenced in Synthesis Path
| CAS-RN | Formula | Chemical Name | CAS Index Name |
|---|---|---|---|
| 108-24-7 | C4H6O3 | acetic anhydride | Acetic acid, anhydride |
| 69123-71-3 | C7H5ClN2O3 | 2-amino-5-nitrobenzoyl chloride | Benzoyl chloride, 2-amino-5-nitro- |
| 23076-31-5 | C14H13N3O3 | N-(2-amino-5-nitrobenzoyl)-o-toluidine | Benzamide, 2-amino-N-(2-methylphenyl)-5-nitro- |
| 56287-72-0 | C16H14FN3O4 | 2-[(fluoroacetyl)amino]-N-(2-methylphenyl)-5-nitrobenzamide | Benzamide, 2-[(fluoroacetyl)amino]-N-(2-methylphenyl)-5-nitro- |
| 359-06-8 | C2H2ClFO | fluoroacetyl chloride | Acetyl chloride, fluoro- |
| 56287-73-1 | C16H12FN3O3 | 2-(fluoromethyl)-3-(2-methylphenyl)-6-nitro-4(3H)-quinazolinone | 4(3H)-Quinazolinone, 2-(fluoromethyl)-3-(2-methylphenyl)-6-nitro- |
| 616-79-5 | C7H6N2O4 | 5-nitroanthranilic acid | Benzoic acid, 2-amino-5-nitro- |
| 95-53-4 | C7H9N | o-toluidine | Benzenamine, 2-methyl- |
Trade Names
| Country | Trade Name | Vendor | Annotation |
|---|---|---|---|
| J | Aflomus | Hishiyama | |
| Airomate | SawaiNippon Chemiphar | ||
| Arofuto | Tanabe |
Formulations
- tabl. 20 mg
References
-
- Tani, J. et al.: J. Med. Chem. (JMCMAR) 22, 95 (1979).
- DOS 2 449 113 (Tanabe; appl. 15.10.1974; J-prior. 15.10.1973).
- US 3 966 731 (Tanabe; 29.6.1976; J-prior. 15.10.1973)
Title: Afloqualone
CAS Registry Number: 56287-74-2
CAS Name: 6-Amino-2-(fluoromethyl)-3-(2-methylphenyl)-4(3H)-quinazolinone
Additional Names: 6-amino-2-fluoromethyl-3-(o-tolyl)-4(3H)-quinazolinone
Manufacturers’ Codes: HQ-495
Trademarks: Arofuto (Tanabe)
Molecular Formula: C16H14FN3O
Molecular Weight: 283.30
Percent Composition: C 67.83%, H 4.98%, F 6.71%, N 14.83%, O 5.65%
Literature References: A centrally acting muscle relaxant. Prepn: I. Inoue et al., DE 2449113; eidem, US 3966731 (1975, 1976 to Tanabe); J. Tani et al., J. Med. Chem. 22, 95 (1979). Pharmacology: T. Ochiai, R. Ishida, Jpn. J. Pharmacol. 31, 491 (1981); 32,427 (1982). Metabolism: N. Otsuka et al., J. Pharmacobio-Dyn. 5, S-59 (1982); S. Furuuchi et al., Drug Metab. Dispos. 11, 371 (1983).
Properties: Pale yellow prisms from 2-propanol, mp 195-196°. LD50 in mice (mg/kg): 315.1 i.p. (Tani).
Melting point: mp 195-196°
Toxicity data: LD50 in mice (mg/kg): 315.1 i.p. (Tani)
Therap-Cat: Muscle relaxant (skeletal).
Keywords: Muscle Relaxant (Skeletal).
FDA approves first drug Epidiolex (cannabidiol) comprised of an active ingredient derived from marijuana to treat rare, severe forms of epilepsy
The U.S. Food and Drug Administration today approved Epidiolex (cannabidiol) [CBD] oral solution for the treatment of seizures associated with two rare and severe forms of epilepsy, Lennox-Gastaut syndrome and Dravet syndrome, in patients two years of age and older. This is the first FDA-approved drug that contains a purified drug substance derived from marijuana. It is also the first FDA approval of a drug for the treatment of patients with Dravet syndrome.
June 25, 2018
Release
The U.S. Food and Drug Administration today approved Epidiolex (cannabidiol) [CBD] oral solution for the treatment of seizures associated with two rare and severe forms of epilepsy, Lennox-Gastaut syndrome and Dravet syndrome, in patients two years of age and older. This is the first FDA-approved drug that contains a purified drug substance derived from marijuana. It is also the first FDA approval of a drug for the treatment of patients with Dravet syndrome.
CBD is a chemical component of the Cannabis sativa plant, more commonly known as marijuana. However, CBD does not cause intoxication or euphoria (the “high”) that comes from tetrahydrocannabinol (THC).
It is THC (and not CBD) that is the primary psychoactive component of marijuana.
“This approval serves as a reminder that advancing sound development programs that properly evaluate active ingredients contained in marijuana can lead to important medical therapies. And, the FDA is committed to this kind of careful scientific research and drug development,” said FDA Commissioner Scott Gottlieb, M.D. “Controlled clinical trials testing the safety and efficacy of a drug, along with careful review through the FDA’s drug approval process, is the most appropriate way to bring marijuana-derived treatments to patients. Because of the adequate and well-controlled clinical studies that supported this approval, prescribers can have confidence in the drug’s uniform strength and consistent delivery that support appropriate dosing needed for treating patients with these complex and serious epilepsy syndromes. We’ll continue to support rigorous scientific research on the potential medical uses of marijuana-derived products and work with product developers who are interested in bringing patients safe and effective, high quality products. But, at the same time, we are prepared to take action when we see the illegal marketing of CBD-containing products with serious, unproven medical claims. Marketing unapproved products, with uncertain dosages and formulations can keep patients from accessing appropriate, recognized therapies to treat serious and even fatal diseases.”
Dravet syndrome is a rare genetic condition that appears during the first year of life with frequent fever-related seizures (febrile seizures). Later, other types of seizures typically arise, including myoclonic seizures (involuntary muscle spasms). Additionally, status epilepticus, a potentially life-threatening state of continuous seizure activity requiring emergency medical care, may occur. Children with Dravet syndrome typically experience poor development of language and motor skills, hyperactivity and difficulty relating to others.
Lennox-Gastaut syndrome begins in childhood. It is characterized by multiple types of seizures. People with Lennox-Gastaut syndrome begin having frequent seizures in early childhood, usually between ages 3 and 5. More than three-quarters of affected individuals have tonic seizures, which cause the muscles to contract uncontrollably. Almost all children with Lennox-Gastaut syndrome develop learning problems and intellectual disability. Many also have delayed development of motor skills such as sitting and crawling. Most people with Lennox-Gastaut syndrome require help with usual activities of daily living.
“The difficult-to-control seizures that patients with Dravet syndrome and Lennox-Gastaut syndrome experience have a profound impact on these patients’ quality of life,” said Billy Dunn, M.D., director of the Division of Neurology Products in the FDA’s Center for Drug Evaluation and Research. “In addition to another important treatment option for Lennox-Gastaut patients, this first-ever approval of a drug specifically for Dravet patients will provide a significant and needed improvement in the therapeutic approach to caring for people with this condition.”
Epidiolex’s effectiveness was studied in three randomized, double-blind, placebo-controlled clinical trials involving 516 patients with either Lennox-Gastaut syndrome or Dravet syndrome. Epidiolex, taken along with other medications, was shown to be effective in reducing the frequency of seizures when compared with placebo.
The most common side effects that occurred in Epidiolex-treated patients in the clinical trials were: sleepiness, sedation and lethargy; elevated liver enzymes; decreased appetite; diarrhea; rash; fatigue, malaise and weakness; insomnia, sleep disorder and poor quality sleep; and infections.
Epidiolex must be dispensed with a patient Medication Guide that describes important information about the drug’s uses and risks. As is true for all drugs that treat epilepsy, the most serious risks include thoughts about suicide, attempts to commit suicide, feelings of agitation, new or worsening depression, aggression and panic attacks. Epidiolex also caused liver injury, generally mild, but raising the possibility of rare, but more severe injury. More severe liver injury can cause nausea, vomiting, abdominal pain, fatigue, anorexia, jaundice and/or dark urine.
Under the Controlled Substances Act (CSA), CBD is currently a Schedule I substance because it is a chemical component of the cannabis plant. In support of this application, the company conducted nonclinical and clinical studies to assess the abuse potential of CBD.
The FDA prepares and transmits, through the U.S. Department of Health and Human Services, a medical and scientific analysis of substances subject to scheduling, like CBD, and provides recommendations to the Drug Enforcement Administration (DEA) regarding controls under the CSA. DEA is required to make a scheduling determination.
The FDA granted Priority Review designation for this application. Fast-Track designation was granted for Dravet syndrome. Orphan Drug designation was granted for both the Dravet syndrome and Lennox-Gastaut syndrome indications.
The FDA granted approval of Epidiolex to GW Research Ltd.

/////////// Epidiolex, cannabidiol, fda 2018, Dravet syndrome, epilepsy, Priority Review , Fast-Track designation, Orphan Drug designation
RG7440, Ipatasertib, アイパタセルチブ;
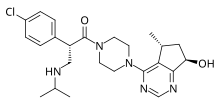
Ipatasertib
GDC-0068 , RG7440
CAS 1001264-89-6, C24H32ClN5O2, 457.9962
アイパタセルチブ;
イパタセルチブ;
Antineoplastic, AKT serine/threonine kinase inhibitor
2(S)-(4-Chlorophenyl)-1-[4-[7(R)-hydroxy-5(R)-methyl-6,7-dihydro-5H-cyclopenta[d]pyrimidin-4-yl]piperazin-1-yl]-3-(isopropylamino)propan-1-one
(2S)-2-(4-Chlorophenyl)-1-(4-((5R,7R)-7-hydroxy-5-methyl-6,7-dihydro-5H-cyclopenta(d)pyrimidin-4-yl)piperazin-1-yl(-3-((propan-2-yl)amino)propan-1-one
1-Propanone, 2-(4-chlorophenyl)-1-(4-((5R,7R)-6,7-dihydro-7-hydroxy-5-methyl-5H-cyclopentapyrimidin-4-yl)-1-piperazinyl)-3-((1-methylethyl)amino)-, (2S)-
Ipatasertib dihydrochloride
1396257-94-5
Ipatasertib (RG7440) is an experimental cancer drug in development by Roche. It is a small molecule inhibitor of Akt. It was discovered by Array Biopharma and is currently in phase II trials for treatment of breast cancer.[1]
In vitro, ipatasertib showed activity against all three isoforms of Akt.[2]
Ipatasertib is an orally-available protein kinase B (PKB/Akt) inhibitor in phase III clinical development at Genentech for the treatment of metastatic castration-resistant prostate cancer in combination with abiraterone and prednisone.
In 2014, orphan drug designation was assigned in the U.S. for the treatment of gastric cancer including cancer of the gastro-esophageal junction.
Ipatasertib. An orally bioavailable inhibitor of the serine/threonine protein kinase Akt (protein kinase B) with potential antineoplastic activity. Ipatasertib binds to and inhibits the activity of Akt in a non-ATP-competitive manner, which may result in the inhibition of the PI3K/Akt signaling pathway and tumor cell proliferation and the induction of tumor cell apoptosis. Activation of the PI3K/Akt signaling pathway is frequently associated with tumorigenesis and dysregulated PI3K/Akt signaling may contribute to tumor resistance to a variety of antineoplastic agents. Check for active clinical trials using this agent.
PROBLEM
It has been found that ipatasertib exhibits a very high solubility (>1 g/g water; >2 g/g water/ethanol 1:1) and a very high hygroscopicity (˜6% at 50% RH, >35% at 95% RH). Whereas poor solubility is often a limiting factor in the development of galenical formulations of other API’s (active pharmaceutical ingredient), a high solubility can equally be problematic for the process performance. Due to this very high intrinsic hygroscopicity of the API, ipatasertib drug substance tends to auto-dissolve to a honey-like viscous liquid at increased humidity. Such high solubility and hygroscopicity may pose serious problems for processing as well as for stability and shelf-life of the final product. Therefore, conventional pharmaceutical compositions comprising ipatasertib and processes for the manufacture of pharmaceutical compositions comprising wetting (e.g. wet granulation) are difficult due to the high solubility and high hygroscopicity of the API.
SYN

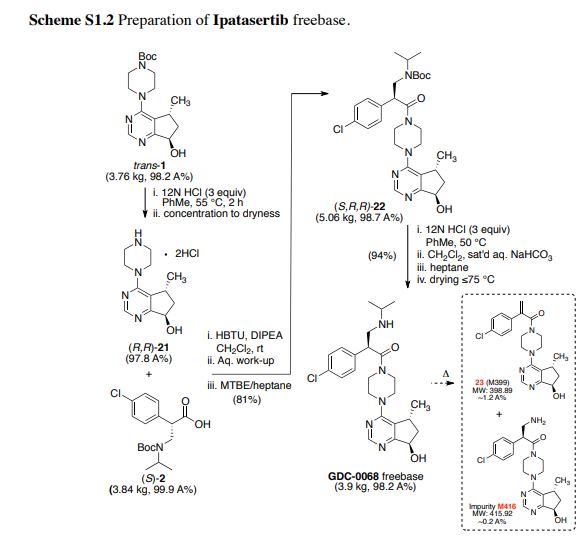
Bromination of (+)-(R)-pulegone (I) with Br2 in the presence of NaHCO3 in Et2O, followed by ring contraction via Favorskii rearrangement with NaOEt in EtOH, and treatment with semicarbazide hydrochloride and NaOAc in refluxing EtOH/H2O gives rise to cyclopentanecarboxylate (II) (1). Subsequent ozonolysis of olefin (II) by means of O3 in EtOAc at -78 °C, and reductive treatment with Zn in AcOH provides beta-ketoester (III). Reaction of ketoester (III) with ammonium acetate (IVa) in MeOH/CH2Cl2 yields enamine (V), which upon cyclization with ammonium formate (IVb) and formamide (VI) at 150 °C provides cyclopentapyrimidinol (VII). Chlorination of pyrimidinol (VII) using POCl3 in refluxing CH2Cl2 results in 4-chloro-5(R)-methyl-6,7-dihydro-5H-cyclopenta[d]pyrimidine (VIII), which is condensed with N-Boc-piperazine (IX) in the presence of DIEA in refluxing BuOH to produce piperazinyl cyclopentapyrimidine (X). Oxidation of compound (X) using mCPBA and NaHCO3 in CHCl3 furnishes N-oxide (XI). Subsequent rearrangement of N-oxide (XI) using Ac2O in CH2Cl2 at 100 °C yields acetate (XII). This compound (XII) is hydrolyzed with LiOH in H2O/THF to give alcohol (XIII), which upon Swern oxidation with (COCl)2, DMSO and Et3N in CH2Cl2 at -78 °C affords ketone (XIV) (1-6). Asymmetric transfer hydrogenation of ketone (XIV) in the presence of RuCl[(R,R)-TsDPEN(p-cymene)], HCOOH and Et3N in CH2Cl2, followed by protection with PNBCl in the presence of Et3N in CH2Cl2, and hydrolysis with LiOH in H2O/THF gives rise to alcohol (XV) (1-6). Also, intermediate (XV) can be produced by enzymatic reduction of ketone (XI) using KRED-101 in the presence of GDH, NADP, KOH and PEG-400, KRED-X1.1-P1F01 in the presence of glucose and NAD in DMSO/i-PrOH or KRED-X1.1-P1B06, KRED-X1.1-P1F01 or KRED-X1.1-P1H10 in the presence of NADP in DMSO/i-PrOH or i-PrOH (11,12). In an alternative method, asymmetric transfer hydrogenation of ketone (XIV) in the presence of RuCl[(R,R)-MsDPEN(p-cymene)], HCOOH and Et3N in CH2Cl2, followed by O-protection of the resultant cis/trans mixture of alcohols with PNBCl and Et3N or protection with pivaloyl chloride in the presence of DIEA in CH2Cl2, followed by separation of the resulting cis/trans mixture of esters by means of HPLC. Hydrolysis of trans ester with LiOH in THF yields alcohol (XV) (11). N-Deprotection of piperazine derivative (XV) by means of HCl in CH2Cl2, i-PrOH or toluene at 62 °C provides amine dihydrochloride (XVI) (1-7,11,12), which is then coupled with aminoacid derivative (XVIIa) (1-7,11) or its sodium salt (XVIIb) (12,13) in the presence of DIEA and HBTU in CH2Cl2 or NMM and T3P in i-PrOH or toluene to produce amide (XVIII) (1-7,11-13). Finally, Boc-deprotection of precursor (XVIII) by means of HCl in MeOH/Et2O, PrOH, i-PrOH or toluene at 57 °C furnishes the target GDC-0068

Synthesis of intermediate (XVII): Condensation of methyl (4-chlorophenyl)acetate (XIX) with formaldehyde (XX) in the presence of NaOMe in DMSO gives beta-hydroxyester (XXI). Subsequent dehydration of alcohol (XXI) using MsCl and Et3N in CH2Cl2 provides arylacrylate (XXII), which upon conjugate addition with isopropylamine (XXIII) in the presence of Boc2O in THF yields N-Boc beta-aminoester (XXIV). Basic hydrolysis of ester (XXIV) using KOSiMe3 in THF generates the potassium carboxylate (XXV), which upon condensation with 4(R)-benzyl-2-oxazolidinone (XXVI) via activation with pivaloyl chloride and BuLi in THF at -78 °C affords the N-acyl oxazolidinone (XXVII) (2-6). Finally, removal of the chiral auxiliary group of (XXVII) using LiOH and H2O2 in THF/H2O furnishes the key intermediate (XVII) (1-6,11). Alternative synthesis of intermediate (XXVII): Protection of isopropylamine (XXIII) with Boc2O in toluene affords tert-butyl isopropylcarbamate (XXVIII), which upon N-alkylation with bromomethyl methyl ether (XXIX) in the presence of NaHMDS in 2-MeTHF gives tert-butyl isopropyl(methoxymethyl)carbamate (XXX) (11). Condensation of 4(R)-benzyl-2-oxazolidinone (XXVI) with 2-(4-chlorophenyl)acetyl chloride (XXXIIa) using BuLi in THF at -50 °C (1) or with 2-(4-chlorophenyl)acetic acid (XXXIIb) via activation with pivaloyl chloride and Et3N in refluxing toluene (11) affords N-acyl oxazolidinone(XXXI). After conversion of intermediate (XXXI) to its titanium enolate with TiCl4 and DIEA in CH2Cl2 at -50 °C, diastereoselective Mannich reaction with formaldehyde hemiaminal (XXX) affords adduct (XXVII)
PAPER
Synthesis of Akt inhibitor ipatasertib. Part 2. Total synthesis and first kilogram scale-up
Org Process Res Dev 2014, 18(12): 1652
https://pubs.acs.org/doi/full/10.1021/op500270z
https://pubs.acs.org/doi/suppl/10.1021/op500270z/suppl_file/op500270z_si_001.pdf
Synthesis of Akt Inhibitor Ipatasertib. Part 2. Total Synthesis and First Kilogram Scale-up
† Small Molecule Process Chemistry, Genentech, Inc., a member of the Roche Group, 1 DNA Way, South San Francisco, California 94080-4990, United States
‡ Array BioPharma Inc., 3200 Walnut Street, Boulder, Colorado 80301, United States
Org. Process Res. Dev., 2014, 18 (12), pp 1652–1666
DOI: 10.1021/op500270z
*E-mail: travisr@gene.com.

Herein, the first-generation process to manufacture Akt inhibitor Ipatasertib through a late-stage convergent coupling of two challenging chiral components on multikilogram scale is described. The first of the two key components is a trans-substituted cyclopentylpyrimidine compound that contains both a methyl stereocenter, which is ultimately derived from the enzymatic resolution of a simple triester starting material, and an adjacent hydroxyl group, which is installed through an asymmetric reduction of the corresponding cyclopentylpyrimidine ketone substrate. A carbonylative esterification and subsequent Dieckmann cyclization sequence was developed to forge the cyclopentane ring in the target. The second key chiral component, a β2-amino acid, is produced using an asymmetric aminomethylation (Mannich) reaction. The two chiral intermediates are then coupled in a three-stage endgame process to complete the assembly of Ipatasertib, which is isolated as a stable mono-HCl salt.
(S)-2-(4-Chlorophenyl)-1-(4-((5R,7R)-7-hydroxy-5-methyl-6,7-dihydro-5H-cyclopenta[d]pyrimidin-4-yl)piperazin-1-yl)-3-(isopropylamino)propan-1-one, Ipatasertib Mono-HCl
Ipatasertib mono-HCl (3.23 kg, 80% yield) as an off-white solid. Analytical results: 99.7 A% [0.26% S,R,S-diastereomer observed)]; impurity 23 (M399) was not detected (<0.02 A%) [Method 2.2]; ruthenium content by IPC-AES = 5 ppm; analysis for PF6 anion by CAD-HPLC resulted in not detected [Method 2.3]; residual solvent = 0.4% EtOAc; ion chromatography (IC) = 8.5% chloride (1.14 salt equivalent); DSC = 141 °C; FTIR (neat) 3269 (br OH), 2961–2865 (N–H stretch), 1637 (C═O stretch); 1H NMR (600 MHz, DMSO-d6) 9.39 (s, 1H), 8.64 (s, 1H), 8.49 (s, 1H), 7.49 (q, J = 2.9 Hz, 2H), 7.41 (q, J = 2.9 Hz, 2H), 5.58 (s, 1H), 4.91 (t, J = 6.9 Hz, 1H), 4.78 (dd, J = 8.9, 4.5 Hz, 1H), 3.81 (m, J = 3.3 Hz, 1H), 3.68 (m, J = 3.3 Hz, 1H), 3.67 (m, J = 3.1 Hz, 1H), 3.65 (m, J = 3.2 Hz, 1H), 3.63 (m, J = 3.6 Hz, 1H), 3.59 (m, J = 4.3 Hz, 1H), 3.51 (m, J = 3.5 Hz, 1H), 3.46 (m, J = 3.5 Hz, 1H), 3.36 (m, J = 3.2 Hz, 1H), 3.30 (m, J = 5.7 Hz, 1H), 3.21 (m, J = 3.4 Hz, 1H), 2.98 (m, J = 5.8 Hz, 1H), 1.97 (m, J = 4.8 Hz, 2H), 1.26 (d, J = 6.6 Hz, 3H), 1.25 (d, J = 7.0 Hz, 3H); 13C NMR (150 MHz, DMSO-d6) 170.2, 168.2, 159.4, 155.2, 135.3, 132.5, 129.7 (2C), 129.1 (2C), 120.8, 71.7, 50.4, 47.0, 44.8, 44.5, 44.1, 41.4, 40.8, 34.5, 19.8, 18.4, 18.1; HRMS calcd for C24H32ClN5O2 457.2245; found [M+H]+ 458.2306.
Ipatasertib freebase (3.9 kg, 98.2 A% containing ~1.2% impurity 23 (M399) and impurity M416 at 0.2 A% [Method 2.2]) as tan solid. By CAD-HPLC (see Figure S1-2), the PF6 anion was present in ~0.86 A% [Method 2.3]; Ion chromatography (IC) = 4.0% chloride (0.56 salt equivalent); 1 H NMR (600 MHz, DMSO-d6) 8.44 (s, 1H), 7.45 (d, J = 8.5 Hz, 2H), 7.40 (d, J = 8.5 Hz, 2H), 5.48 (br s, 1H), 4.86 (t, J = 6.9 Hz, 1H), 4.58 (dd, J = 7.3, 4.6 Hz, 1H), 3.74 (m, 1H), 3.40 (m, 1H), 3.63 (m, 2H), 3.61 (m, 1H), 3.42 (m, 1H), 3.57 (m, 1H), 3.18 (m, 1H), 3.50 (m, J = 2.9 Hz, 1H), 3.09 (m, J = 3.1 Hz, 1H), 3.42 (m, 1H), 2.87 (m, J = 4.7 Hz, 1H), 2.00 (m, 1H), 1.92 (m, J = 3.1 Hz, 1H), 1.15 (d, J = 6.4 Hz, 6H), 1.03 (d, J = 6.9 Hz, 3H); 13C NMR (150 MHz, DMSO-d6) 172.0, 169.0, 159.6, 156.3, 136.3, 132.1, 129.7 (2C), 128.9 (2C), 120.9, 72.0, 49.4, 48.7, 45.4, 44.9, 44.8, 44.6, 41.4, 40.9, 34.3, 20.1, 19.9, 19.7; HRMS calcd for C24H32ClN5O2 [M+H]+ 458.2317; found 458.2312. See supporting information (S2) for the NMR spectra (DMSO-d6) of Ipatasertib freebase: ( 1 H) S2, Figure S2-5.12 and ( 13C) Figure S2-5.13.
https://pubs.acs.org/doi/suppl/10.1021/op500270z/suppl_file/op500270z_si_002.pdf
Table S2-1 1 H NMR Assignments of Ipatasertib mono-HCl. S2-52 Figure S2-5.10. 13C NMR (DMSO-d6) spectrum of Ipatasertib mono-HCl. S2-53 Table S2-2 13C NMR Assignments of Ipatasertib mono-HCl. S2-54 Table S2-3 Characteristic Ipatasertib mono-HCl Infrared Signals. S2-55 Figure S2-5.11. FTIR Spectrum of Ipatasertib mono-HCl. S2-56 Figure S2-5.12. XRPD Pattern of Ipatasertib mono-HCl. S2-57
PAPER
https://pubs.acs.org/doi/abs/10.1021/op500271w
https://pubs.acs.org/doi/suppl/10.1021/op500271w/suppl_file/op500271w_si_001.pdf
Synthesis of Akt Inhibitor Ipatasertib. Part 1. Route Scouting and Early Process Development of a Challenging Cyclopentylpyrimidine Intermediate
† Array BioPharma Inc., 3200 Walnut Street, Boulder, Colorado 80301, United States
‡ Genentech Inc., a member of the Roche Group, 1 DNA Way, South San Francisco, California 94080-4990, United States
Org. Process Res. Dev., 2014, 18 (12), pp 1641–1651
DOI: 10.1021/op500271w
*E-mail: jlane@arraybiopharma.com., *E-mail: travisr@gene.com.

Herein, the route scouting and early process development of a key cyclopentylpyrimidine ketone intermediate toward the synthesis of Akt inhibitor Ipatasertib are described. Initial supplies of the intermediate were prepared through a method that commenced with the natural product (R)-(+)-pulegone and relied on the early construction of a methyl-substituted cyclopentyl ring system. The first process chemistry route, detailed herein, enabled the synthesis of the ketone on a hundred-gram scale, but it was not feasible for the requisite production of multikilogram quantities of this compound and necessitated the exploration of alternative strategies. Several new synthetic approaches were investigated towards the preparation of the cyclopentylpyrimidine ketone, in either racemic or chiral form, which resulted in the discovery of a more practical route that hinged on the initial preparation of a highly substituted dihydroxypyrimidine compound. The cyclopentane ring in the target was then constructed through a key carbonylative esterification and subsequent tandem Dieckmann cyclization–decarboxylation sequence that was demonstrated in a racemic synthesis. This proof-of-concept was later developed into an asymmetric synthesis of the cyclopentylpyrimidine ketone, which will be described in a subsequent paper, along with the synthesis of Ipatasertib.
PAPER
Discovery and preclinical pharmacology of a selective ATP-Competitive akt inhibitor (GDC-0068) for the treatment of human tumors
J Med Chem 2012, 55(18): 8110
PAPER
Asymmetric synthesis of akt kinase inhibitor ipatasertib
Org Lett 2017, 19(18): 4806
PATENT
WO 2008006040
PATENT
WO 2012135753
PATENT
WO 2012135759
PATENT
WO 2012135781
PATENT
WO 2013173784
PATENT
WO 2015073739
PATENT
WO 2012135779
PATENT
WO 2013173768
References
- Jump up^ https://www.clinicaltrials.gov/ct2/show/NCT02301988
- Jump up^ Lin K, Friedman L, Gloor S, Gross S, Liederer BM, Mitchell I, et al. Preclinical characterization of GDC-0068, a novel selective ATP competitive inhibitor of Akt. 22nd-EORTC-NCI-AACR-2010 2010; abstr. 79
 |
|
| Clinical data | |
|---|---|
| Routes of administration |
PO |
| ATC code |
|
| Identifiers | |
| ChemSpider | |
| KEGG | |
| Chemical and physical data | |
| Formula | C24H32ClN5O2 |
| Molar mass | 458.00 g·mol−1 |
| 3D model (JSmol) | |
////////////// ipatasertib, orphan drug designation, GDC-0068 , RG7440, PHASE 3
CC(C)NC[C@@H](C(=O)N1CCN(CC1)c2ncnc3[C@H](O)C[C@@H](C)c23)c4ccc(Cl)cc4
It has been found that ipatasertib exhibits a very high solubility (>1 g/g water; >2 g/g water/ethanol 1:1) and a very high hygroscopicity (˜6% at 50% RH, >35% at 95% RH). Whereas poor solubility is often a limiting factor in the development of galenical formulations of other API’s (active pharmaceutical ingredient), a high solubility can equally be problematic for the process performance. Due to this very high intrinsic hygroscopicity of the API, ipatasertib drug substance tends to auto-dissolve to a honey-like viscous liquid at increased humidity. Such high solubility and hygroscopicity may pose serious problems for processing as well as for stability and shelf-life of the final product. Therefore, conventional pharmaceutical compositions comprising ipatasertib and processes for the manufacture of pharmaceutical compositions comprising wetting (e.g. wet granulation) are difficult due to the high solubility and high hygroscopicity of the API.
Linrodostat BMS 986205, ONO 7701
cas 2221034-29-1
- Linrodostat
- (2R)-N-(4-chlorophenyl)-2-(cis-4-(6-fluoroquinolin-4-yl)cyclohexyl)propanamide
- Linrodostat mesylate
- Linrodostat [USAN]
- UNII-OS7OBU191R
- OS7OBU191R
- Linrodostat mesylate [USAN]
- BMS-986205-04
- 2221034-29-1
- Cyclohexaneacetamide, N-(4-chlorophenyl)-4-(6-fluoro-4-quinolinyl)-alpha- methyl-, (alphaR,1alpha,4alpha)-, methanesulfonate (1:1)
Linrodostat; (2R)-N-(4-chlorophenyl)-2-(cis-4-(6-fluoroquinolin-4-yl)cyclohexyl)propanamide; Linrodostat mesylate; Linrodostat [USAN]; UNII-OS7OBU191R; OS7OBU191R


BMS 986205
(2R)-N-(4-Chlorophenyl)-2-[cis-4-(6-fluoro-4-quinolinyl)cyclohexyl]propanamide
Cyclohexaneacetamide, N-(4-chlorophenyl)-4-(6-fluoro-4-quinolinyl)-α-methyl-, cis-
Cyclohexaneacetamide, N-(4-chlorophenyl)-4-(6-fluoro-4-quinolinyl)-α-methyl-, cis-(αR)-
(i?)-N-(4-chlorophenyl)-2- c 5-4-(6-fluoroquinolin-4-yl)cyclohexyl)propanamide
CAS: 1923833-60-6
Phase III Head and neck cancer; Malignant melanoma
BMS-986205, ONO-7701, F- 001287
- Molecular Formula C24H24ClFN2O
- Average mass 410.912 Da
BMS986205, BMS 986205, ONO-7701
Cyclohexaneacetamide, N-(4-chlorophenyl)-4-(6-fluoro-4-quinolinyl)-α-methyl-, cis-(αR)-
A potent and selective IDO1 (indoleamine 2,3-dioxygenase 1) inhibitor.
| Alternate Name | (R)-N-(4-chlorophenyl)-2-((1s,4S)-4-(6-fluoroquinolin-4-yl)cyclohexyl)propenamide |
|---|---|
| Appearance | Crystalline solid |
| CAS # | 1923833-60-6 |
| Molecular Formula | C₂₄H₂₄ClFN₂O |
| Molecular Weight | 410.92
|
- Originator Bristol-Myers Squibb
- Developer Bristol-Myers Squibb; Ono Pharmaceutical
- Class Antineoplastics; Cyclohexanes; Quinolines; Small molecules
- Mechanism of Action Indoleamine-pyrrole 2,3-dioxygenase inhibitors
Highest Development Phases
- Phase II IHead and neck cancer; Malignant melanoma
- Phase I/II Cancer
- Phase I Solid tumours
Most Recent Events
- 01 Jun 2018Efficacy and adverse events data from a phase I/IIa trial in Bladder cancer (Combination therapy, Late-stage disease) presented at the 54th Annual Meeting of the American Society of Clinical Oncology (ASCO- 2018)
- 08 May 2018Bristol-Myers Squibb plans the CheckMate 9UT phase II trial for Bladder Cancer in USA, Canada, Italy, Mexico, Netherlands, Spain and United Kingdom , (NCT03519256)
- 30 Apr 2018Bristol-Myers Squibb withdraws a phase III trial for Non-small cell lung cancer (First-line therapy, Combination therapy, Late-stage disease) in USA, Austria, Australia, Brazil, Canada, Czech Republic, France, Germany, Greece, Italy, Japan, South Korea, Mexico, Spain, Switzerland, Taiwan and Turkey prior to enrolment (NCT03417037)
BMS , following its acquisition of Flexus Biosciences , and licensee Ono Pharmaceutical are developing linrodostat, a once-daily, indoleamine 2,3-dioxygenase 1 inhibitor for the potential oral treatment of cancer including renal cell carcinoma, muscle-invasive bladder cancer and melanoma. In October 2018, the trial was initiated in the US, Europe, Israel and Brazil.
WO2015031295 product pat
WO2016073770 first disclosed
WO2018209049
- WO 2016073770


Bristol-Myers Squibb, following its acquisition of Flexus Biosciences, is developing BMS-986205 (previously F- 001287), the lead from an immunotherapy program of indoleamine 2,3-dioxygenase 1 (IDO1) inhibitors for the potential treatment of cancer. In February 2016, a phase I/IIa trial was initiated .
BMS-986205 (ONO-7701) is being evaluated at Bristol-Myers Squibb in phase I/II clinical trials for the oral treatment of adult patients with advanced cancers in combination with nivolumab. Early clinical development is also ongoing at Ono in Japan for the treatment of hematologic cancer and for the treatment of solid tumors.
In April 2017, data from the trial were presented at the 108th AACR Annual Meeting in Washington DC. As of February 2017, the MTD had not been reached, but BMS-986205 plus nivolumab treatment was well tolerated, with only two patients discontinuing treatment due to DLTs. The most commonly reported treatment-related adverse events (TRAEs) were decreased appetite, fatigue, nausea, diarrhea, and vomiting. Grade 3 TRAEs were reported in three patients during the combination therapy; however, no grade 3 events were reported during BMS-986205 monotherapy lead-in. No grade 4 or 5 TRAEs were reported with BMS-986205 alone or in combination with nivolumab
Indoleamine 2,3-dioxygenase (IDO; also known as IDOl) is an IFN-γ target gene that plays a role in immunomodulation. IDO is an oxidoreductase and one of two enzymes that catalyze the first and rate-limiting step in the conversion of tryptophan to N-formyl-kynurenine. It exists as a 41kD monomer that is found in several cell populations, including immune cells, endothelial cells, and fibroblasts. IDO is relatively well-conserved between species, with mouse and human sharing 63% sequence identity at the amino acid level. Data derived from its crystal structure and site-directed mutagenesis show that both substrate binding and the relationship between the substrate and iron-bound dioxygenase are necessary for activity. A homolog to IDO (ID02) has been identified that shares 44% amino acid sequence homology with IDO, but its function is largely distinct from that of IDO. (See, e.g., Serafini P, et al, Semin. Cancer Biol, 16(l):53-65 (Feb. 2006) and Ball, H.J. et al, Gene, 396(1):203-213 (Jul. 2007)).
IDO plays a major role in immune regulation, and its immunosuppressive function manifests in several manners. Importantly, IDO regulates immunity at the T cell level, and a nexus exists between IDO and cytokine production. In addition, tumors frequently manipulate immune function by upregulation of IDO. Thus, modulation of IDO can have a therapeutic impact on a number of diseases, disorders and conditions.
A pathophysiological link exists between IDO and cancer. Disruption of immune homeostasis is intimately involved with tumor growth and progression, and the production of IDO in the tumor microenvironment appears to aid in tumor growth and metastasis. Moreover, increased levels of IDO activity are associated with a variety of different tumors (Brandacher, G. et al, Clin. Cancer Res., 12(4): 1144-1151 (Feb. 15, 2006)).
Treatment of cancer commonly entails surgical resection followed by chemotherapy and radiotherapy. The standard treatment regimens show highly variable degrees of long-term success because of the ability of tumor cells to essentially escape by regenerating primary tumor growth and, often more importantly, seeding distant metastasis. Recent advances in the treatment of cancer and cancer-related diseases, disorders and conditions comprise the use of combination therapy incorporating immunotherapy with more traditional chemotherapy and radiotherapy. Under most scenarios, immunotherapy is associated with less toxicity than traditional chemotherapy because it utilizes the patient’s own immune system to identify and eliminate tumor cells.
In addition to cancer, IDO has been implicated in, among other conditions, immunosuppression, chronic infections, and autoimmune diseases or disorders (e.g. , rheumatoid arthritis). Thus, suppression of tryptophan degradation by inhibition of IDO activity has tremendous therapeutic value. Moreover, inhibitors of IDO can be used to enhance T cell activation when the T cells are suppressed by pregnancy, malignancy, or a virus (e.g., HIV). Although their roles are not as well defined, IDO inhibitors may also find use in the treatment of patients with neurological or neuropsychiatric diseases or disorders (e.g., depression).
Small molecule inhibitors of IDO have been developed to treat or prevent IDO-related diseases. For example, the IDO inhibitors 1-methyl-DL-tryptophan; p-(3-benzofuranyl)-DL-alanine; p-[3-benzo(b)thienyl]-DL-alanine; and 6-nitro-L-tryptophan have been used to modulate T cell-mediated immunity by altering local extracellular concentrations of tryptophan and tryptophan metabolites (WO 99/29310). Compounds having IDO inhibitory activity are further reported in WO 2004/094409.
In view of the role played by indoleamine 2,3-dioxygenase in a diverse array of diseases, disorders and conditions, and the limitations (e.g., efficacy) of current IDO inhibitors, new IDO modulators, and compositions and methods associated therewith, are needed.
In April 2017, preclinical data were presented at the 108th AACR Annual Meeting in Washington DC. BMS-986205 inhibited kynurenine production with IC50 values of 1.7, 1.1 and > 2000 and 4.6, 6.3 and > 2000 nM in human (HeLa, HEK293 expressing human IDO-1 and tryptophan-2, 3-dioxygenase cell-based assays) and rat (M109, HEK293 expressing mouse ID0-1 and -2 cell-based assays) respectively. In human SKOV-3 xenografts (serum and tumor) AUC (0 to 24h; pharmacokinetic and pharmacodynamic [PK and PD])) was 0.8, 4.2 and 23 and 3.5, 11 and 40 microM h, respectively; area under the effect curve (PK and PD) was 39, 32 and 41 and 60, 63 and 76% kyn, at BMS-986205 (5, 25 and 125 mg/kg, qd×5), respectively
In April 2017, preclinical data were presented at the 253rd ACS National Meeting and Exhibition in San Francisco, CA. BMS-986205 showed potent and selective inhibition of IDO-1 enzyme (IC50 = 1.7nM) and potent growth inhibition in cellular assays (IC50 = 3.4 nM) in SKOV3 cells. A good pharmacokinetic profile was seen at oral and iv doses in rats, dogs and monkeys. The compound showed good oral exposure and efficacy in in vivo assays
Preclinical studies were performed to evaluate the activity of BMS-986205, a potent and selective optimized indoleamine 2, 3-dioxygenase (IDO)- 1inhibitor, for the treatment of cancer. BMS-986205 inhibited kynurenine production with IC50 values of 1.7, 1.1 and > 2000 and 4.6, 6.3 and > 2000 nM in human (HeLa, HEK293 expressing human IDO-1 and tryptophan-2, 3-dioxygenase cell-based assays) and rat (M109, HEK293 expressing mouse ID0-1 and -2 cell-based assays) respectively. BMS-986205 was also found to be potent when compared with IDO-1from other species (human < dog equivalent monkey equivalent mouse > rat). In cell-free systems, incubation of inhibitor lead to loss of heme absorbance of IDO-1 which was observed in the presence of BMS-986205 (10 microM), while did not observed with epacadostat (10 microM). The check inhibitory activity and check reversibility (24 h after compound removal) of BMS-986205 was found to be < 1 and 18% in M109 (mouse) and < 1 and 12% SKOV3 (human) cells, respectively. In human whole blood IDO-1, human DC mixed lymphocyte reaction and human T cells cocultured with SKOV3 cells- cell based assays, BMS-986205 showed potent cellular effects (inhibition of kynurenine and T-cell proliferation 3H-thymidine) with IC50 values of 2 to 42 (median 9.4 months), 1 to 7 and 15 nM, respectively. In human SKOV-3 xenografts (serum and tumor) AUC (0 to 24h; pharmacokinetic and pharmacodynamic [PK and PD])) was 0.8, 4.2 and 23 and 3.5, 11 and 40 microM h, respectively; area under the effect curve (PK and PD) was 39, 32 and 41 and 60, 63 and 76% kyn, at BMS-986205 (5, 25 and 125 mg/kg, qd×5), respectively. In vivo human-SKOV3 and hWB-xenografts, IC50 values of BMS-986205 were 3.4 and 9.4 NM, respectively. The ADME of BMS-986205 at parameters iv/po dose was 0.5/2, 0.5/1.5 and 0.5/1.2 mg/kg, respectively; iv/clearance was 27, 25 and 19 ml, min/kg, respectively; iv Vss was 3.8, 5.7 and 4.1 l/kg, respectively; t1/2 (iv) was 3.9, 4.7 and 6.6 h, respectively; fraction (po) was 64, 39 and 10%, respectively. At the time of presentation, BMS-986205 was being evaluated in combination with nivolumab.
The chemical structure and preclinical profile was presented for BMS-986205 ((2R)-N-(4-Chlorophenyl)-2-[cis-4-(6-fluoroquinolin-4-yl)cyclohexyl]propanamide), a potent IDO-1 inhibitor in phase I for the treatment of cancer. This compound showed potent and selective inhibition of IDO-1 enzyme (IC50 = 1.7nM) and potent growth inhibition in cellular assays (IC50 = 3.4 nM) in SKOV3 cells. The pharmacokinetic profile in rats dosed at 0.5 mg/kg iv and 2 mg/kg po, with clearance, Vss, half-life and bioavailability of 27 ml/min/kg, 3.8 l/kg, 3.9 h and 4%, respectively; in dogs at 0.5 iv and 1.5 po mg/kg dosing results were 25 ml/min/kg, 5.7 l/kg, 4.7 h and 39%; and, in cynomolgus monkeys with the same doses as dogs results were 19 ml/min/kg, 4.1 l/kg, 6.6 h and 10%, respectively. The compound showed good oral exposure and efficacy in in vivo assays.
BMS-986158: a BET inhibitor for cancerAshvinikumar Gavai of Bristol Myers Squibb (BMS) gave an overview of his company’s research into Bromodomian and extra-terminal domain (BET) as oncology target for transcriptional suppression of key oncogenes, such as MYC and BCL2. BET inhibition has been defined as strong rational strategy for the treatment of hematologic malignancies and solid tumors. From crystal-structure guided SAR studies, BMS-986158, 2-{3-(1,4-Dimethyl-1H-1,2,3-triazol-5-yl)-5-[(S)-(oxan-4-yl)(phenyl)methyl]-5H-pyrido[3,2-b]indol-7-yl}propan-2-ol, was chosen as a potent BET inhibitor, showing IC50 values for BRD2, BRD3 and BRD4 activity of 1 nM; it also inhibited Myc oncogene (IC50 = 0.5 nM) and induced chlorogenic cancer cell death. In vitro the compound also displayed significant cytotoxicity against cancer cells. When administered at 0.25, 0.5 and 1 mg/kg po, qd to mice bearing human lung H187 SCLC cancer xenograft, BMS-986158 was robust and showed efficacy as a anticancer agent at low doses. In metabolic studies, it showed t1/2 of 36, 40 and 24 min in human, rat and mice, respectively, and it gave an efflux ratio of 3 in Caco-2 permeability assay. In phase 1/II studies, BMS-986158 was well tolerated at efficacious doses and regimens, and drug tolerable toxicity at efficacy doses and regimens. Selective Itk inhibitors for inflammatory disordersThe development of highly selective Itk inhibitors for the treatment of diseases related to T-cell function, such as inflammatory disorders, was described by Shigeyuki Takai (Ono Pharmaceutical). Inhibitory properties of a hit compound, ONO-8810443, were modified via X-ray structure and Molecular Dynamics stimulation to get ONO-212049 with significant kinase selectivity (140-fold) against Lck, a tyrosine kinase operating upstream of Itk in the TCR cascade. Further modifications identified final lead compound ONO-7790500 (N-[6-[3-amino-6-[2-(3-methoxyazetidin-1-yl)pyridin-4-yl]pyrazin-2-yl]pyridin-3-yl]-1-(3-methoxyphenyl)-2,3-dimethyl-5-oxopyrazole-4-carboxamide), which selectively inhibited Itk (IC50 = < 0.004 microM) over Lck (IC50 = 9.1 microM; SI 2000-fold) and suppressed Jurkat T-cell proliferation (IC50 = 0.014 microM). This compound suppressed alphaCD3/CDP28 CD4+T-cell stimulation (IC50 = 0.074 microM) with selectivity over PMA/Ionomycin (IC50 = > 10 microM). ONO-7790500 also exhibited in vivo IL-2 inhibitory properties (62% inhibition at 30 mg/kg po) in mice. In pharmacokinetic studies in balb/c mice, the compound administered orally (10 mg/kg) showed a Cmax of 1420 ng/ml, AUClast of 11,700 ng*h/ml, t1/2 of 5.3 h and oral bioavailability of 68%. Administration iv at 0.3 mg/kg gave an AUC last of 610 ng*h/ml, t1/2 of 3.8 h, Vss of 1260 ml/kg and Cl of 5.1 ml/min/kg. ADMET data showed ONO-7790500 did not have relevant activity in cytochromes and hERG channels (IC50 > 10 microM) in toxicological studies, and gave a PAMPA value of 5.0 x 10(-6) cm/s. Fused imidazole and pyrazole derivatives as TGF-beta inhibitorsDual growth and differentiation factor-8 (GDF-8; also known as myostatin) and TGF-beta inhibitors were described. Both targets belong to TGF-beta superfamily consisting of a large group of structurally related cell regulatory proteins involved in fundamental biological and pathological processes, such as cell proliferation or immunomodulation. Myostatin (GDF8) is a negative regulator negative regulator of skeletal muscle growth and has also been related to bone metabolism. Investigators at Rigel Pharmaceuticals found that compounds designed to be GDF-8 inhibitors were able to inhibit TGF-beta as well, this could be an advantage for the treatment of diseases associated with muscle and adipose tissue disorders, as well as potentially immunosuppressive disorders. Jiaxin Yu from the company described new fused imidazole derivatives, of which the best compound was 6-[2-(2,4,5-Trifluorophenyl)-6,7-dihydro-5H-pyrrolo[1,2-a]imidazol-3-yl]quinoxaline. This compound was very potent at TGF-beta Receptor Type-1 (ALK5) inhibition with an IC50 value of 1nM. In an in vivo mouse assay this compound showed good activity at 59.7 mg/kg, po, and good plasma exposure; inhibition of GDF-8 and TGFbeta growth factors was 90 and 81.6 %, respectively.Rigel’s Ihab Darwish described a series of fused pyrazole derivatives, with the best compound being 6-[2-(2,4-Difluorophenyl)-5,6-dihydro-4H-pyrrolo[1,2-b]pyrazol-3-yl][1,2,4]triazolo[1,5-a]pyridine. This compound showed an IC50 of 0.06 and 0.23 microM for GDF-8 and TGFbeta, respectively, in the pSMAD (MPC-11) signaling inhibition test. The compound had a good pharmacokinetic profile, with 40% of bioavailability in mice after a 5-mg/kg po dose. An iv dose of 1 mg/kg showed t1/2 of 0.7 h and Vss of 1.0 l/h/kgDiscovery of selective inhibitor of IDO BMS-986205 for cancerIndoleamine-2,3-dioxygenase (IDO)-1 enzyme initiates and regulates the first step of the kynurenine pathway (KP) of tryptophan metabolism, and evidence has shown that overexpression of IDO-1 in cancer tumors is a crucial mechanism facilitating tumor immune evasion and persistence. The chemical structure and preclinical profile of BMS-986205 was presented by Aaron Balog from BMS. BMS-986205 ((2R)-N-(4-Chlorophenyl)-2-[cis-4-(6-fluoroquinolin-4-yl)cyclohexyl]propanamide), is a potent IDO-1 inhibitor in phase I for the treatment of cancer. This compound showed potent and selective inhibition of IDO-1 enzyme (IC50 = 1.7nM) and potent growth inhibition in cellular assays (IC50 = 3.4 nM) in SKOV3 cells. The pharmacokinetic profile in rats dosed at 0.5 mg/kg iv and 2 mg/kg po, with clearance, Vss, half-life and bioavailability of 27 ml/min/kg, 3.8 l/kg, 3.9 h and 4%, respectively; in dogs at 0.5 iv and 1.5 po mg/kg dosing results were 25 ml/min/kg, 5.7 l/kg, 4.7 h and 39%; and, in cynomolgus monkeys with the same doses as dogs results were 19 ml/min/kg, 4.1 l/kg, 6.6 h and 10%, respectively. The compound showed good oral exposure and efficacy in in vivo assays.Three further reports have been published from this meeting .The website for this meeting can be found at https://www.acs.org/content/acs/en/meetings/spring-2017.html.
SYNTHESIS
1 Wittig NaH
2 REDUCTION H2, Pd, AcOEt, 4 h, rt, 50 psi
3 Hydrolysis HCl, H2O, Me2CO, 2 h, reflux
4 4-Me-2,6-(t-Bu)2-Py, CH2Cl2, overnight, rt
5 SUZUKI AcOK, 72287-26-4, Dioxane, 16 h, 80°C
6 Heck Reaction, Suzuki Coupling, Hydrogenolysis of Carboxylic Esters, Reduction of Bonds, HYDROGEN
7 Et3N, THF, rt – -78°C , Pivaloyl chloride, 15 min, -78°C; 1 h, 0°C ,THF, 0°C – -78°C, BuLi, Me(CH2)4Me, 15 min, -78°C, R:(Me3Si)2NH •Na, THF, 10 min, -50°C , HYDROLYSIS, (PrP(=O)O)3, C5H5N, AcOEt, 5 min, rt

Product Patent
WO2016073770
Example 19
(i?)-N-(4-chlorophenyl)-2- c 5-4-(6-fluoroquinolin-4-yl)cyclohexyl)propanamide
Example 19 : (i?)-N-(4-chlorophenyl)-2-(cz5-4-(6-fluoroquinolin-4- yl)cyclohexyl)propanamide
[0277] Prepared using General Procedures K, B, E, L, M, N, and O. General Procedure L employed 2-(4-(6-fluoroquinolin-4-yl)-cyclohexyl)acetic acid (mixture of
diastereomers), and ( ?)-2-phenyl-oxazolidinone. General Procedure M employed the cis product and iodomethane. The auxiliary was removed following General Procedure N and the desired product formed employing General Procedure O with 4-chloroaniline.
Purified using silica gel chromatography (0% to 100% ethyl acetate in hexanes) to afford Example 19. 1H NMR of czs-isomer (400 MHz; CDC13): δ 9.14 (s, 1H), 8.70 (d, J= 4.6 Hz, 1H), 8.06 (dd, J= 9.2 Hz, J= 5.6 Hz, 1H), 7.58-7.64 (m, 3H), 7.45 (ddd, J= 9.3 Hz, J= 7.8 Hz, J= 2.7 Hz, 1H), 7.19-7.24 (m, 2H), 7.15 (d, J= 4.6Hz, 1H), 3.16-3.26 (m, 1H), 2.59-2.69 (m, 1H), 2.08-2.16 (m, 1H), 1.66-1.86 (m, 7H), 1.31-1.42 (m, 1H), 1.21 (d, J= 6.8Hz, 3H) ppm. m/z 411.2 (M+H)+.
PAPER
Bioorganic & Medicinal Chemistry Letters (2018), 28(3), 319-329.
https://www.sciencedirect.com/science/article/pii/S0960894X17312180

PATENT
WO 2018022992
PATENT
WO 2018071500
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2018071500&redirectedID=true
WO-2019006292
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2019006292&tab=PCTDESCRIPTION&maxRec=1000
Improved methods for the preparation of substituted quinolinycyclohexylpropanamide compounds, such as linrodostat claiming substituted pyridine compounds as IDO1 inhibitors, useful for treating cancers.
Indoleamine 2,3 -di oxygenase (IDO; also known as IDOl) is an IFN-γ target gene that plays a role in immunomodulation. IDO plays a major role in immune regulation, and its immunosuppressive function manifests in several manners. A pathophysiological link exists between IDO and cancer. Disruption of immune homeostasis is intimately involved with tumor growth and progression, and the production of IDO in the tumor microenvironment appears to aid in tumor growth and metastasis. Moreover, increased levels of IDO activity are associated with a variety of different tumors (Brandacher, G. et al, Clin. Cancer Res. , 12(4): 1144-1151 (Feb. 15, 2006)). In addition to cancer, IDO has been implicated in, among other conditions, immunosuppression, chronic infections, and autoimmune diseases or disorders (e.g., rheumatoid arthritis).
Substituted quinolinylcyclohexylpropanamide pharmaceutical compounds that inhibit IDO and are useful for the treatment of cancer have been previously described. See, e.g., WO2016/073770. Improved methods of making such compounds, which reduce production costs and improve production safety, are, therefore, needed.
Scheme 4
[0076] The disclosure is also directed to methods of preparing intermediate compounds of formula IV. Methods to produce compounds of formula IV are depicted in Schemes 5 and 6.
Scheme 5
IX-A
Scheme 6
IX-B IV
Compounds of the disclosure that include one or more radioisotopes can be used in imaging. See, e.g., WO2018017529. For example, radiolabeled compounds of the disclosure can be used in Positron Emission Tomography (PET). Such methods are useful in the imaging of cancer in a subject. A preferred radiolabeled compound is
1
Pharmaceutically acceptable salts of [18F]-Compound 1 are also within the scope of the disclosure. An exemplary method for the preparation of [18F]-Compound 1 is depicted in Scheme below.
1 . reaction
[18F]-Compound 1
Example 9
(R)-N-(4-chlorophenyl)-2-((ls,4S)-4-(6-fluoroquinolin-4-yl)cyclohexyl)propanamide
[00258] To a 10 L glass-lined reactor under a blanket of nitrogen was charged 349 g Ν,Ν,Ν’,Ν’-tetramethylchloroformamidinium hexafluorophosphate (TCFH) and 2 L acetonitrile. 245 g N-methylimidazole was added followed by 0.3 L acetonitrile. 300 g (R)-2-((ls,4S)-4-(6-fluoroquinolin-4-yl)cyclohexyl)propanoic acid was added followed by 0.3 L acetonitrile. The mixture was held for 0.5 h then 139 g 4-chloroaniline charged followed by 0.4 L acetonitrile. The mixture was maintained at 20 °C until the reaction was deemed complete by HPLC analysis. The solution was then heated to 60°C, and 1.2 L water was charged. The solution was then cooled to 40 °C, seeds (3 g) were charged, and the resulting slurry was maintained for 1 h. The slurry was then cooled to 20 °C and 2.7 L water was charged. The slurry was filtered and the cake was washed three times with 3 L of 2: 1 water: acetonitrile. The cake was dissolved with 5.1 L ethyl acetate and the solution was distilled to a volume of 4.2 L at 41 °C under vacuum. The slurry was cooled to 20 °C, 4.14 g seeds were charged, and a solution of 95.7 g methanesulfonic acid in 2.9 L ethyl acetate was added. The slurry was then filtered and washed two times with 1.65 L ethyl acetate and dried under vacuum at 50°C to yield 445 g of (R)-N-(4-chlorophenyl)-2-((l s,4S)-4-(6-fluoroquinolin-4-yl)cyclohexyl)propanamide methanesulfonate as a white solid in 88% yield.
[00259] ¾ NMR (600 MHz, DMSO-de) δ 10.19 (s, IH), 9.24 (d, J=5.7 Hz, IH), 8.40 (dd, J=10.3, 2.6 Hz, IH), 8.33 (dd, J=9A, 5.3 Hz, IH), 8.09 (d, J=5.7 Hz, IH), 8.04 (t, J=8.6 Hz, IH), 7.71 – 7.64 (m, 2H), 7.37 – 7.30 (m, 2H), 3.64 (ddt, J=10.8, 7.3, 3.8 Hz, IH), 2.98 – 2.89 (m, IH), 2.43 (s, 3H), 2.05 – 1.60 (m, 9H), 1.14 (d, J=6.7 Hz, 3H); 13C NMR (126 MHz, DMSO-de) δ 175.0, 162.7, 161.1 , 145.4, 138.2, 136.8, 128.6, 128.1 , 126.7, 126.4, 123.3, 120.8, 119.8, 109.0, 39.8, 39.7, 38.6, 35.5, 28.3, 27.6, 27.2, 26.1 , 16.2 MS (ESI): calcd for C24H24CIFN2O
([M + H]+), 410.16; found, 410.15.
[00260] HPLC analysis: Column: Sigma-Aldrich Supelco Ascentis Express CI 8 2.7um, 150 x 4.6 mm ID; Solvent A: 0.05% TFA with MeCN:water (5/95 v/v); Solvent B: 0.05% TFA with MeCN: water (95/5 v/v); Gradient: %B: 0 Min. 15%; 1 Min. 15%; 13 Min. 55%; 19 Min. 65%; 24 Min. 100%; 24.1 15%; 28 Min. 15%; Stop Time: 24 Min; Flow Rate: 1.0 ml/min;
Column temperature: 30 °C; wavelength: 218 nm. The retention time (R)-N-(4-chlorophenyl)-2-((ls,4S)-4-(6-fluoroquinolin-4-yl)cyclohexyl)propanamide peak was 12.6 min.
Example 7
(R)-N-(4-chlorophenyl)-2-((ls, -4-(6-fluoroquinolin-4-yl)cyclohexyl)propanamide
[00252] To a 50 L glass-lined reactor under a blanket of nitrogen was charged 13.75 kg acetonitrile, then 2.68 Kg Ν,Ν,Ν’,Ν’-tetramethylchloroformamidinium hexafluorophosphate (TCFH) and rinsed with 2.0 Kg acetonitrile. 2.03 Kg N-methylimidazole was added followed by 1.95 Kg acetonitrile. 2.48 Kg (R)-2-((ls,4S)-4-(6-fluoroquinolin-4-yl)cyclohexyl)propanoic acid was added followed by 1.05 Kg acetonitrile. The mixture was held for 0.5 h then 1.21 Kg 4-chloroaniline charged followed by 1.0 Kg acetonitrile. The mixture was maintained at 20 °C until the reaction was deemed complete by HPLC analysis. The solution was then heated to 60°C, and 9.25 Kg water was charged. The solution was then cooled to 40 °C, the mixture was aged
for 1 h, seeds (32 g) were charged and rinsed with 1.15 Kg 2: 1 water: acetonitrile, and the resulting slurry was maintained for 1 h. The slurry was then cooled to 20 °C and 25.75 Kg water was charged. The slurry was filtered and the cake was washed three times with 6.9 Kg of 2: 1 water: acetonitrile. The cake was dried under vacuum at 50°C to yield 3.33 Kg of (R)-N-(4-chlorophenyl)-2-((ls,4S)-4-(6-fluoroquinolin-4-yl)cyclohexyl)propanamide hydrate as a white solid in 94.1% yield.
[00253] ¾ NMR (600 MHz, DMSO-de) δ 10.09 (s, 1H), 8.86 (d, J=4.5 Hz, 1H), 8.08 (dd, J=9.0, 5.6 Hz, 1H), 7.95 (dd, J=10.9, 2.6 Hz, 1H), 7.70 – 7.60 (m, 3H), 7.54 (d, J=4.5 Hz, 1H), 7.33 (d, J=9.0 Hz, 2H), 3.43 – 3.31 (m, 3H), 2.90 – 2.80 (m, 1H), 1.99 – 1.55 (m, 9H), 1.13 (d, J=6.8 Hz, 3H); 13C NMR (151 MHz, DMSO-de) δ 175.0, 159.9, 152.4, 149.7, 145.2, 138.1, 132.7, 128.5, 127.2, 126.7, 120.8, 119.0, 118.6, 107.2, 40.2, 37.4, 35.6, 28.5, 27.6, 27.4, 26.3, 16.1 ; HRMS (ESI); calcd for C24H24CIFN2O ([M + H]+), 411.1619; found 411.1649.
WO-2019006283
https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2019006283&redirectedID=true
Novel crystalline forms of linrodostat , its salts and hydrates, designated as Forms 1, 2 and 4 (first disclosed in WO2016073770 ), processes for their preparation and compositions comprising them are claimed. Also claims are their use for treating prostate cancer, liver cancer, brain cancer, bladder cancer, ovary cancer and breast cancer.
(R)-N-(4-chlorophenyl)-2-((l S,4S)-4-(6-fluoroquinolin-4-yl)cyclohexyl)propanami the below structure:
[0003] Compound 1 is a potent inhibitor of indoleamine 2,3-dioxygenase (IDO; also known as IDOl), which is an IFN-γ target gene that plays a role in immunomodulation.
Compound 1 is being investigated as a treatment for cancer and other diseases. Compound 1 has been previously described in WO2016/073770.
[0004] A compound, as a free base, hydrate, solvate, or salt, can exist in amorphous form and/or one or more crystalline forms, each having different physical properties, for example, different X-ray diffraction patterns (XRPD or PXRD) and different thermal behavior. The free base, hydrate, solvate, and salt forms of a compound can also differ with respect to their individual stabilities, processing, formulation, dissolution profile, bioavailability, and the like. [0005] New forms of (R)-N-(4-chlorophenyl)-2-((l S,4S)-4-(6-fluoroquinolin-4-yl)cyclohexyl)propanamide, having desirable and beneficial chemical and physical properties are needed. There is also a need for reliable and reproducible methods for the manufacture, purification, and formulation of Compound 1 (and its hydrates, solvates, salt,, and hydrated salt forms) to facilitate commercialization. The present disclosure is directed to these, as well as other important aspects.
REFERENCES
23-Feb-2015
Bristol-Myers Squibb To Expand Its Immuno-Oncology Pipeline with Agreement to Acquire Flexus Biosciences, Inc
Bristol-Myers Squibb Co; Flexus Biosciences Inc
17-Dec-2014
Flexus Biosciences, a Cancer Immunotherapy Company Focused on Agents for the Reversal of Tumor Immunosuppression (ARTIS), Announces $38M Financing
Flexus Biosciences Inc
2015106thApril 21Abs 4290
Potent and selective next generation inhibitors of indoleamine-2,3-dioxygenase (IDO1) for the treatment of cancer
American Association for Cancer Research Annual Meeting
Jay P. Powers, Matthew J. Walters, Rajkumar Noubade, Stephen W. Young, Lisa Marshall, Jan Melom, Adam Park, Nick Shah, Pia Bjork, Jordan S. Fridman, Hilary P. Beck, David Chian, Jenny V. McKinnell, Maksim Osipov, Maureen K. Reilly, Hunter P. Shunatona, James R. Walker, Mikhail Zibinsky, Juan C. Jaen
2017108thApril 04Abs 4964
Structure, in vitro biology and in vivo pharmacodynamic characterization of a novel clinical IDO1 inhibitor
American Association for Cancer Research Annual Meeting
John T Hunt, Aaron Balog, Christine Huang, Tai-An Lin, Tai-An Lin, Derrick Maley, Johnni Gullo-Brown, Jesse Swanson, Jennifer Brown
2017253rdApril 05Abs MEDI 368
Discovery of a selective inhibitor of indoleamine-2,3-dioxygenase for use in the therapy of cancer
American Chemical Society National Meeting and Exposition
Aaron Balog
April 2-62017
American Chemical Society – 253rd National Meeting and Exhibition (Part IV) – OVERNIGHT REPORT, San Francisco, CA, USA
Casellas J, Carceller V
////////////////PHASE 1, BMS 986205, 1923833-60-6, BMS-986205, ONO-7701,Bristol-Myers Squibb, Antineoplastics, F- 001287
C[C@H]([C@H]1CC[C@@H](C2=CC=NC3=CC=C(F)C=C23)CC1)C(NC4=CC=C(Cl)C=C4)=O
Wrapping up #MEDI‘s 1st time disclosures is Aaron Balog of @bmsnews talking about an IOD-1 inhibitor to treat cancer #ACSSanFran
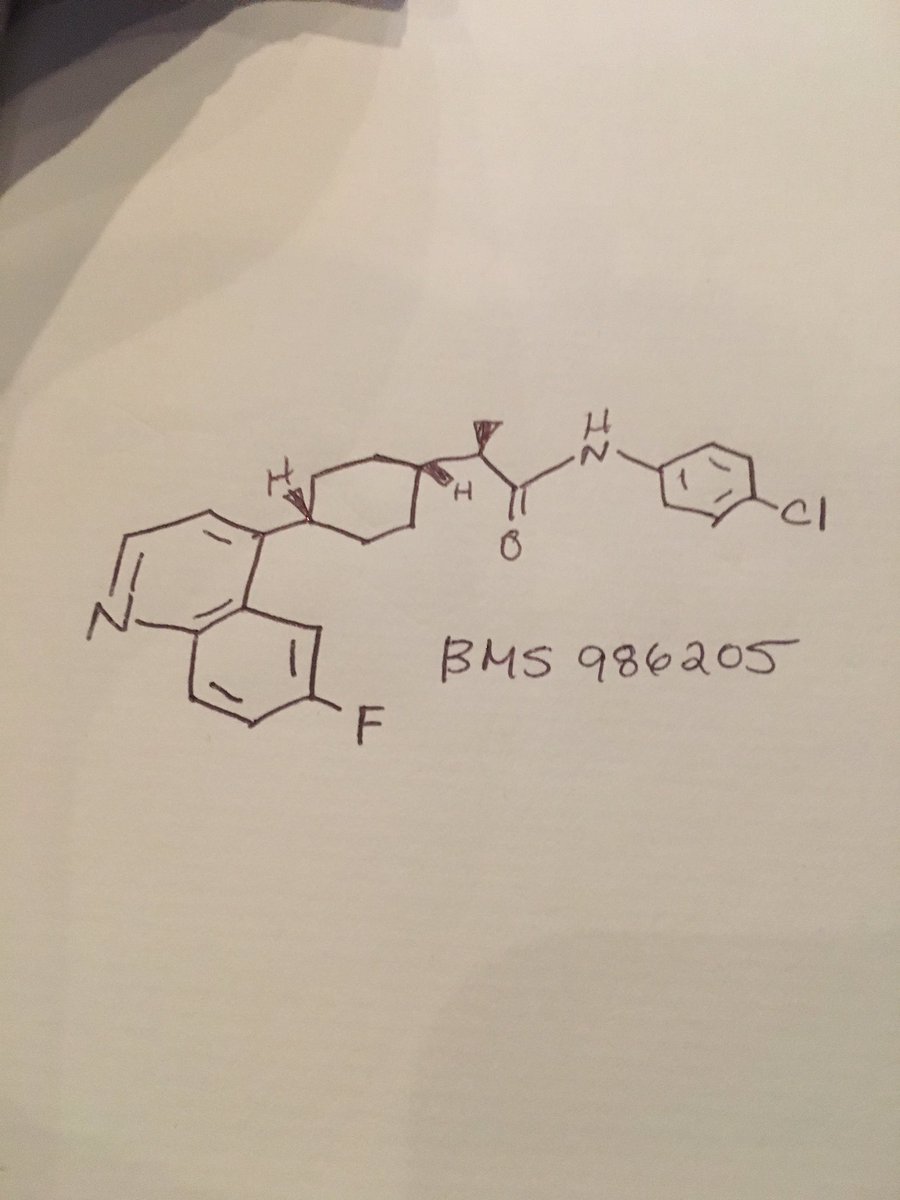
////////////////BMS986205, BMS 986205, BM-986205, ONO-7701, Phase III, Head and neck cancer, Malignant melanoma, 1923833-60-6, Linrodostat
CC(C1CCC(CC1)C2=C3C=C(C=CC3=NC=C2)F)C(=O)NC4=CC=C(C=C4)Cl
ABL 001, Asciminib
ABL001 / Asciminib
Cas 1492952-76-7
Chemical Formula: C20H18ClF2N5O3
Molecular Weight: 449.8428
Elemental Analysis: C, 53.40; H, 4.03; Cl, 7.88; F, 8.45; N, 15.57; O, 10.67
N-[4-[Chloro(difluoro)methoxy]phenyl]-6-[(3R)-3-hydroxypyrrolidin-1-yl]-5-(1H-pyrazol-5-yl)pyridine-3-carboxamide
3-Pyridinecarboxamide, N-[4-(chlorodifluoromethoxy)phenyl]-6-[(3R)-3-hydroxy-1-pyrrolidinyl]-5-(1H-pyrazol-3-yl)-
PHASE 3, Chronic Myeloid Leukemia, NOVARTIS
UPDATE FDA APPROVED 10/29/2021,
| Scemblix |
To treat Philadelphia chromosome-positive chronic myeloid leukemia with disease that meets certain criteria
Asciminib, sold under the brand name Scemblix, is a medication used to treat Philadelphia chromosome-positive chronic myeloid leukemia (Ph+ CML).[1][2][3] Asciminib is a protein kinase inhibitor.[1]
The most common adverse reactions include upper respiratory tract infections, musculoskeletal pain, fatigue, nausea, rash, and diarrhea.[2]
Asciminib was approved for medical use in the United States in October 2021.[1][4][5]
The U.S. Food and Drug Administration (FDA) granted the application for asciminib priority review, fast track, orphan drug, and breakthrough therapy designations.[2][6][7]
Asciminib is an orally bioavailable, allosteric Bcr-Abl tyrosine kinase inhibitor with potential antineoplastic activity. Designed to overcome resistance, ABL001 binds to the Abl portion of the Bcr-Abl fusion protein at a location that is distinct from the ATP-binding domain. This binding results in the inhibition of Bcr-Abl-mediated proliferation and enhanced apoptosis of Philadelphia chromosome-positive (Ph+) hematological malignancies. The Bcr-Abl fusion protein tyrosine kinase is an abnormal enzyme produced by leukemia cells that contain the Philadelphia chromosome.
ABL001 has been used in trials studying the health services research of Chronic Myelogenous Leukemia and Philadelphia Chromosome-positive Acute Lymphoblastic Leukemia.

- Originator Novartis
- Developer Novartis; Novartis Oncology
- Class Antineoplastics; Pyrazoles; Pyrrolidines; Small molecules
- Mechanism of Action Bcr-abl tyrosine kinase inhibitors
Highest Development Phases
- Phase III Chronic myeloid leukaemia
- No development reported Precursor cell lymphoblastic leukaemia-lymphoma
Most Recent Events
- 04 Nov 2017 No recent reports of development identified for phase-I development in Acute-lymphoblastic-leukaemia(Second-line therapy or greater) in Australia (PO)
- 04 Nov 2017 No recent reports of development identified for phase-I development in Acute-lymphoblastic-leukaemia(Second-line therapy or greater) in France (PO)
- 04 Nov 2017 No recent reports of development identified for phase-I development in Acute-lymphoblastic-leukaemia(Second-line therapy or greater) in Germany (PO)
- The tyrosine kinase activity of the ABLl protein is normally tightly regulated, with the N-terminal cap region of the SH3 domain playing an important role. One regulatory mechanism involves the N-terminal cap glycine-2 residue being myristoylated and then interacting with a myristate binding site within the SHI catalytic domain. A hallmark of chronic myeloid leukemia (CML) is the Philadelphia chromosome (Ph), formed by the t(9,22) reciprocal chromosome translocation in a haematopoietic stem cell. This chromosome carries the BCR-ABL1 oncogene which encodes the chimeric BCR-ABL1 protein, that lacks the N-terminal cap and has a constitutively active tyrosine kinase domain.Although drugs that inhibit the tyrosine kinase activity of BCR-ABL1 via an ATP-competitive mechanism, such as Gleevec® / Glivec® (imatinib), Tasigna® (nilotinib) and Sprycel® (dasatinib), are effective in the treatment of CML, some patients relapse due to the emergence of drug-resistant clones, in which mutations in the SHI domain compromise inhibitor binding. Although Tasigna® and Sprycel® maintain efficacy towards many Gleevec-resistant mutant forms of BCR-ABLl, the mutation in which the threonine-315 residue is replaced by an isoleucine (T315I) remains insensitive to all three drugs and can result in CML patients developing resistance to therapy. Therefore, inhibiting BCR-ABLl mutations, such as T315I, remains an unmet medical need. In addition to CML, BCR-ABLl fusion proteins are causative in a percentage of acute lymphocytic leukemias, and drugs targeting ABL kinase activity also have utility in this indication.Agents targeting the myristoyl binding site (so-called allosteric inhibitors) have potential for the treatment of BCR-ABLl disorders (J. Zhang, F. J. Adrian, W. Jahnke, S. W. Cowan- Jacob, A. G. Li, R. E. Iacob4, T. Sim, J. Powers, C. Dierks, F. Sun, G.-R. Guo, Q. Ding, B. Okram, Y. Choi, A. Wojciechowski, X. Deng, G. Liu, G. Fendrich, A. Strauss, N. Vajpai, S. Grzesiek, T. Tuntland, Y. Liu, B. Bursulaya, M. Azam, P. W. Manley, J. R. Engen, G. Q. Daley, M. Warmuth., N. S. Gray. Targeting BCR-ABL by combining allosteric with ATP -binding-site inhibitors. Nature 2010;463:501-6). To prevent the emergence of drug resistance from ATP inhibitor and/or allosteric inhibitor use, a combination treatment using both types of inhibitor can be developed for the treatment of BCR-ABLl related disorders. In particular, the need exists for small molecules, or combinations thereof, that inhibit the activity of BCR-ABLl and BCR-ABLl mutations via the ATP binding site, the myristoyl binding site or a combination of both sites.Further, inhibitors of ABL 1 kinase activity have the potential to be used as therapies for the treatment of metastatic invasive carcinomas and viral infections such as pox and Ebola viruses.The compounds from the present invention also have the potential to treat or prevent diseases or disorders associated with abnormally activated kinase activity of wild-type ABL1, including non-malignant diseases or disorders, such as CNS diseases in particular neurodegenerative diseases (for example Alzheimer’s, Parkinson’s diseases), motoneuroneuron diseases (amyotophic lateral sclerosis), muscular dystrophies, autoimmune and inflammatory diseases (diabetes and pulmonary fibrosis), viral infections, prion diseases.
Asciminib is an allosteric inhibitor of BCR-ABL kinase in phase III clinical development at Novartis for the treatment of patients with chronic myelogenous leukemia (CML) in chronic phase who have been previously treated with ATP-binding site tyrosine kinase inhibitors. Early clinical trials are also under way in patients with Philadelphia chromosome-positive acute lymphoblastic leukemia (Ph+ ALL) and as first-line threapy of CML.
PATENT
To illustrate tautomerism with the following specific examples, (R)-N-(4- (chlorodifluoromethoxy)phenyl)-6-(3-hydroxypyrrolidin-l-yl)-5-(lH-pyrazol-5-yl)nicotinamide
(right structure, below) is a tautomer of (R)-N-(4-(chlorodifluoromethoxy)phenyl)-6-(3-hydroxypyrrolidin-l-yl)-5-(lH-pyrazol-3-yl)nicotinamide (left structure, below) and vice versa:

[0045] Where the plural form (e.g. compounds, salts) is used, this includes the singular
Example 9
(R)-N-(4-(Chlorodifluoromethoxy)phenyl)-6-(3-hvdroxypyrrolidin-l-yl)-5-(lH-pyrazol-5- vDnicotinamide

[00365] A mixture of (R)-5-Bromo-N-(4-(chlorodifluoromethoxy)phenyl)-6-(3-hydroxypyrrolidin-l-yl)nicotinamide (Stage 9.2, 100 mg, 0.216 mmol) and 5-(4 ,4,5,5-tetramethyl- 1 ,3 ,2-dioxaborolan-2-yl)- 1 -((2-(trimethylsilyl)ethoxy)methyl)- IH-pyrazole (215 mg, 0.663 mmol), Pd(PPh3)2Cl2 (17 mg, 0.024 mmol), Na2C03 (115 mg, 1.081 mmol), DME (917 μί), water (262 μΕ) and EtOH (131 μί) in a MW vial was sealed, evacuated / purged 3 times with argon and subjected to MW irradiation at 125°C for 20 min. The RM was diluted with 2 mL
of DME, stirred with Si-Thiol (Silicycle 1.44 mmol/g, 90 mg, 0.130 mmol) for 3 h. The mixture was centrifuged and the supernatant was filtered through a 0.45 μηι PTFE filter and the solvent was evaporated off under reduced pressure. The crude product was purified by flash
chromatography (RediSep® Silica gel column, 12 g, cyclohexane / EtOAc from 40% to 100% EtOAc) to afford the protected intermediate as a colorless oil. Ethylene diamine (96 μί, 1.428 mmol) and TBAF 1 M in THF (1.428 mL, 1.428 mmol) were then added and the RM was stirred at 80-85°C for 5 days. The solvent was evaporated off under reduced pressure and the residue was dissolved in EtOAc (40 mL), washed 3 times with sat. aq. NaHCC and brine, dried over Na2S04 and The solvent was evaporated off under reduced pressure to give a residue which was purified by preparative SFC (Column DEAP, from 25% to 30% in 6 min) to yield the title compound as a white solid.
[00366] Alternatively, Example 9 was prepared by adding TFA (168 mL, 2182 mmol) to a solution of N-(4-(chlorodifluoromethoxy)phenyl)-6-((R)-3-hydroxypyrrolidin-l-yl)-5-(l-(tetrahydro-2H-pyran-2-yl)-lH-pyrazol-5-yl)nicotinamide (Stage 9.1, 31.3 g, 54.6 mmol) in DCM (600 mL). The mixture was stirred at RT for 2.5 h. The solvent was evaporated off under reduced pressure and the residue was dissolved in EtOAc (1.5 L),washed with a sat. solution of NaHC03 (3 x 500 mL) and brine (500 mL), dried over Na2S04 and the solvent was evaporated off under reduced pressure to give a residue which was suspended in DCM (300 mL), stirred at RT for 15 min, filtered, washed with DCM (200 mL), dried and purified by chromatography (Silica gel, 1 kg, DCM / MeOH 95:5). The residue was dissolved in MeOH (500 mL) and treated with Si-Thiol (Biotage, 5.0 g , 6.5 mmol) for 16 h at 25°C. The resin was filtered off, the solvent was evaporated off under reduced pressure and the residue was crystallized from MeCN to afford the title compound as a white crystalline solid.
[00367] Alternatively, Example 9 was prepared by the dropwise addition of aqueous HC1
(7.7 mL of 6M) to a solution of N-(4-(chlorodifluoromethoxy)phenyl)-6-((R)-3-hydroxypyrrolidin- 1 -yl)-5-( 1 -(tetrahydro-2H-pyran-2-yl)- 1 H-pyrazol-5-yl)nicotinamide (Stage 9.1, 3.8 g, 7.12 mmol) in MeOH (20 mL) and THF (10 mL) with cooling (below 35°C). The mixture was stirred at 22°C for 2 h and then added to cooled (10°C) 1.2 M NaOH (22 mL).
Throughout the addition the temperature was kept below 30°C and pH was kept in the range of 9-10. The RM was then stirred for 30 min at 30°C. The solvent was evaporated off under reduced pressure, until the desired compound precipitated. The precipitate was filtered and dried to give the title compound as a yellow solid.
[00368] Analytical data for Example 9: HPLC (Condition 5) tR = 5.54 min, HPLC Chiral
(CHIRALCEL® OD-H, 250 x 4.6 mm, eluent : n-heptane/EtOH/MeOH (85: 10:5), 1 mL/min, UV 210 nm) tR = 10.17 min, UPLC-MS (condition 3) tR = 0.93 min, m/z = 450.3 [M+H]+, m/z = 494.1 [M+formic acid-H]“; XH-NMR (400 MHz, DMSO-d6) δ ppm 1.65 – 1.76 (m, 1 H) 1.76 – 1.87 (m, 1 H) 2.93 (d, J=l 1.73 Hz, 1 H) 3.19 – 3.29 (m, 2 H) 3.35 – 3.51 (m, 1 H) 4.10 – 4.25 (m, 1 H) 4.89 (br. s, 1 H) 6.41 (br. s, 1 H) 7.33 (d, J=8.50 Hz, 2 H) 7.57/7.83 (br. s, 1 H) 7.90 (d, J=8.50 Hz, 2 H) 8.07 (br. s, 1 H) 8.77 (br. s, 1 H) 10.23 (s, 1 H) 12.97/13.15 (br. s, 1 H).
[00369] Stage 9.1 : N-(4-(Chlorodifluoromethoxy)phenyl)-6-((R)-3-hydroxypyrrolidin- 1 -yl)-5-( 1 -(tetrahydro-2H-pyran-2- l)- 1 H-pyrazol-5-yl)nicotinamide

[00370] l-(Tetrahydro-2H-pyran-2-yl)-5-(4,4,5,5-tetramethyl-l,3,2-dioxaborolan-2-yl)-lH-pyrazole (29.6 g, 102 mmol), K3P04 (51.6 g, 236 mmol) and Pd(PPh3)4 (4.55 g, 3.93 mmol) were added to a suspension of (R)-5-bromo-N-(4-(chlorodifluoromethoxy)phenyl)-6-(3-hydroxypyrrolidin-l-yl)nicotinamide (Stage 9.2, 36.4 g, 79 mmol) in toluene (360 mL) under an argon atmosphere and the mixture was stirred at 110°C for 4 h. The RM was poured into brine (500 mL) and extracted with EtOAc (2 x 1 L). The combined extracts were washed with brine (500 mL), dried over Na2S04, and the solvent was evaporated off under reduced pressure to give a residue which was purified by chromatography (Silica gel column, 1.5 kg, DCM / MeOH 95:5) to afford a dark yellow foam, that was dissolved in MeOH / DCM (1 L of 3: l) and treated with Si-Thiol (Biotage, 35 g , 45.5 mmol) for 17 h at 30°C. The resin was filtered off, and solvent was evaporated off under reduced pressure, until the desired compound crystallized. The product was filtered washed with MeOH and dried to afford the title compound.
[00371] Alternatively, Stage 9.1 was prepared by adding 4-(chlorodifluoromethoxy)aniline
(16.6 g, 84.9 mmol), NMM (21.7 g, 212.1 mmol), hydroxybenzotriazole hydrate (HOBt H20, 11.9 g, 77.77 mmol) and l-ethyl-3-(3-dimethylaminopropyl)carbodiimide hydrochloride (EDCIHCl, 20.9 g, 109.0 mmol) to a solution of 6-((R)-3-hydroxypyrrolidin-l-yl)-5-(l-(tetrahydro-2H-pyran-2-yl)-lH-pyrazol-5-yl)nicotinic acid (Stage 9.4, 29.83 g, 70.7 mmol) in THF (271 mL). The mixture was stirred for 1.5 h at 25°C and then at 65°C for 16 h. After cooling the RM to 35 °C, further EDCIHCl (13.3 g, 69.4 mmol) was added and the RM was stirred for 1.5 h at 35°C then again at 65°C for 16 h. After cooling the RM to 35°C, water (150 mL) was added, the THF was removed under reduced pressure, EtOAc (180 mL) was added and the mixture was stirred for at 35 °C fori h. The two layers were separated and the aq. phase was then extracted with EtOAc (60 mL). The combined organic layers were washed with water (90 mL), brine (90 mL). The solvent was evaporated off under reduced pressure to give a brown solid which was purified by column chromatography (Silica gel, DCM / MeOH 40: 1 to 20: 1) to afford the title compound as a yellow solid.
[00372] Analytical data for Stage 9.1: HPLC (Condition 5) tR = 6.12 min, UPLC-MS
(Condition 3) tR = 1.06 min, m/z = 533.2 [M+H]+; XH-NMR (400 MHz, DMSO-d6) δ ppm 1.36 -2.02 (m, 7 H) 2.23 – 2.38 (m, 1 H) 3.08 – 3.29 (m, 2 H) 3.32 – 3.52 (m, 2 H) 3.73 – 3.93 (m, 1 H) 4.13 – 4.25 (m, 1 H) 4.80 – 4.90 (m, 1 H) 4.95 – 5.17 (m, 1 H) 6.33 – 6.50 (m, 1 H) 7.33 (d, J=8.99 Hz, 2 H) 7.61 (d, J=1.56 Hz, 1 H) 7.86 (d, J=8.99 Hz, 2 H) 7.97 – 8.11 (m, 1 H) 8.82 (s, 1 H) 10.13 – 10.25 (m, 1 H).
[00373] Stage 9.2: (R)-5-Bromo-N-(4-(chlorodifluoromethoxy)phenyl)-6-(3-hydroxypyrrolidin- 1 -yl)nicotinamide

[00374] (R)-Pyrrolidin-3-ol (9.55 g, 109.6 mmol) and DIPEA (35.1 ml, 201.3 mmol) were added to a suspension of 5-bromo-6-chloro-N-(4-(chlorodifluoromethoxy)phenyl)nicotinamide (Stage 9.3, 37.7 g, 91.5 mmol) in iPrOH (65 mL) and stirred at 140°C for 1 h. EtOAc (700 mL) was added and the solution was washed IN HC1 (2 x 200 mL), sat. NaHCC (200 mL) and brine (2 x 200 mL), dried over Na2S04, and the solution was concentrated under reduced pressure until crystallization commenced. n-Heptane (1 L) were added and the mixture was stirred at RT for 30 min, filtered and washed with ΪΡΓ20 (500 mL) to afford the title compound as a white crystalline solid. HPLC (Condition 5) tR = 6.68 min, UPLC-MS (Condition 3) tR = 1.10 min, m/z =
462.2/464.2 [M+H]+; XH-NMR (400 MHz, DMSO-d6) δ ppm 1.78 – 2.01 (m, 2 H) 3.55 (d, J=l 1.34 Hz, 1 H) 3.66 – 3.75 (m, 1 H) 3.79 – 3.93 (m, 2 H) 4.34 (br. s, 1 H) 4.98 (d, =3.13 Hz, 1 H) 7.32 (d, J=8.99 Hz, 2 H) 7.84 (d, J=8.99 Hz, 2 H) 8.33 (d, J=1.96 Hz, 1 H) 8.66 (d, J=1.96 Hz, 1 H) 10.21 (s, 1 H).
[00375] Stage 9.3: 5-Bromo-6-chloro-N- 4-(chlorodifluoromethoxy)phenyl)nicotinamide

[00376] DMF (2.55 mL, 33.0 mmol) and SOCl2 (24.08 ml, 330 mmol) were added to a suspension of 5-bromo-6-chloro-nicotinic acid (26 g, 110 mmol) in toluene (220 mL) and the RM was stirred at 80°C for 1 h. The solvent was evaporated off under reduced pressure and the residue was dissolved in THF (220 mL) and cooled to -16°C. DIPEA (38.4 mL, 220 mmol) was added, followed by dropwise addition of a solution of 4-(chlorodifluoromethoxy)aniline (22.35 g, 115 mmol) in THF (220 mL) over 15 min. The suspension was stirred for 1 h at RT. The solvent was evaporated off under reduced pressure and the residue was dissolved in TBME (700 mL), washed with IN HC1 (2 x 200 mL), sat. NaHC03 (200 mL) and brine (2 x 200 mL), dried over Na2S04, and the solvent was evaporated off under reduced pressure to give the product which was crystallized from EtOAc – n-heptane to afford the title compound as a white crystalline solid. HPLC (Condition 5) tR = 7.77 min, UPLC-MS (Condition 3) tR = 1.24 min, m/z =
409.1/411.1/413.1 [M+H]+; XH-NMR (400 MHz, DMSO-d6) δ ppm 7.38 (d, =8.99 Hz, 2 H) 7.85 (d, =8.99 Hz, 2 H) 8.72 (br. s, 1 H) 8.92 (br. s, 1 H) 10.68 (s, 1 H).
[00377] Stage 9.4: 6-((R)-3-Hydroxypyrrolidin-l-yl)-5-(l-(tetrahydro-2H-pyran-2-yl)-lH-pyrazol-5-yl)nicotinic acid

[00378] Aq. NaOH (180 niL of 2.6 M) was added to a solution of methyl 6-((R)-3-hydroxypyrrolidin- 1 -yl)-5-(l -(tetrahydro-2H-pyran-2-yl)- 1 H-pyrazol-5-yl)nicotinate (Stage 9.5, 11 lg, 299 mmol) in MeOH (270 mL) and the RM was stirred at RT for 14 h. The MeOH was evaporated off under reduced pressure and the aq. residue was treated with brine (90 mL), extracted with MeTHF twice (540 mL + 360 mL) and the combined organic layers were washed with water (90 mL). MeTHF was added to the combined aq. layers, the biphasic mixture was cooled to 0 °C and acidified (pH = 4-4.5) with aq. HC1 solution (18%) and extracted with
MeTHF. The combined organic extracts were washed with brine and the solvent was evaporated off under reduced pressure to give a residue which was recrystallized from a EtOAc / TBME (1 : 1) to afford the title compound as a white solid. HPLC (Condition 7) tR = 4.74 min, LC-MS
(Condition 8) tR = 3.37 min, m/z = 359.0 [M+H]+; XH-NMR (400 MHz, DMSO-d6) δ ppm 1.44 (br. s, 2 H), 1.51 (d, J=11.54 Hz, 2 H), 1.64 – 1.86 (m, 4 H), 1.90 (br. s, 1 H), 2.31 (d, J=9.29 Hz, 1 H), 2.77 (br. s, 1 H), 3.10 (br. s, 1 H), 3.21 (d, J=8.78 Hz, 2 H), 3.27 – 3.51 (m, 4 H), 3.87 (d, J=11.54 Hz, 1 H), 4.16 (br. s, 1 H), 4.75 – 4.93 (m, 1 H), 5.04 (br. s, 1 H), 6.35 (d, J=17.32 Hz, 1 H), 7.51 – 7.64 (m, 1 H), 7.64 – 7.82 (m, 1 H), 8.67 (d, J=2.26 Hz, 1 H), 12.58 (br. s, 1 H).
[00379] Stage 9.5: Methyl 6-((R)-3-hydroxypyrrolidin-l-yl)-5-(l-(tetrahydro-2H-pyran-2-yl)- 1 H-pyrazol-5-yl)nicotinate

[00380] A mixture of (R)-methyl 5-bromo-6-(3-hydroxypyrrolidin-l-yl)nicotinate (Stage
9.6, 90 g, 299 mmol), l-(tetrahydro-2H-pyran-2-yl)-lH-pyrazole-5-boronic acid pinacol ester (103.9 g, 373.6 mmol), K3P04 (126.9 g, 597.7 mmol), Pd(PPh3)2Cl2 (6.29 g, 8.97 mmol) in toluene (900 mL) was stirred at 92°C and for 16 h. After cooling the mixture to RT, the solution was washed with water (450 mL), 5% NaHCC solution (430 mL) and the solvent was evaporated off under reduced pressure to give a residue which was used without further purifications in the next step. HPLC (Condition 7) tR = 6.929 min, LC-MS (Condition 8) tR = 4.30 min, m/z = 373.0 [M+H ; XH-NMR (400 MHz, DMSO-d6) δ ppm 1.19 – 1.28 (m, 1 H), 1.35 – 1.63 (m, 4 H), 1.63 -1.86 (m, 3 H), 1.89 (br. s, 1 H), 2.12 – 2.39 (m, 1 H), 3.11 (br. s, 1 H), 3.18 – 3.48 (m, 4 H), 3.78 (s, 4 H), 3.88 (d, J=11.54 Hz, 1 H), 4.08 – 4.24 (m, 1 H), 4.86 (dd, J=18.20, 2.89 Hz, 1 H), 5.02 (d, J=8.28 Hz, 1 H), 6.39 (br. s, 1 H), 7.58 (d, J=1.25 Hz, 1 H), 7.78 (br. s, 1 H), 8.69 (t, J=2.01 Hz, 1 H).
[00381] Stage 9.6: (R)-methyl 5-bromo-6-(3-hydroxypyrrolidin-l-yl)nicotinate

[00382] DIPEA (105.3 g, 142.2 mL, 814.4 mmol) was added to a solution of methyl-5-bromo-6-chroronicotinate (85 g, 339.5 mmol) and (R)-pyrrolidin-3-ol (54.2 g, 441.2 mmol) in isopropyl acetate and the RM was stirred at 70°C for 14 h . The solvent was evaporated off under reduced pressure to give a the residue which was dissolved in toluene (850 mL), washed with water (127 mL) and brine (127 mL)and concentrated under reduced pressure until precipitation commenced. n-Heptane (340 mL) was slowly added to the stirred mixture at 22 °C, which was then cooled to 0 °C and the product was filtered, washed with a toluene / n-heptane mixture
(1 : 1.5) and dried to give the title compound as a yellow solid. HPLC (Condition 7) tR = 8.54 min, LC-MS (Condition 8) tR = 4.62 min, m/z = 300.9/302.9 [M+H]+; XH-NMR (400 MHz, DMSO-d6) δ ρριη 1.77 – 1.99 (m, 2 H), 3.57 (d, J=11.54 Hz, 1 H), 3.72 (ddd, J=l 1.11, 7.97, 3.26 Hz, 1 H), 3.78 (s, 3 H), 3.81 -3.90 (m, 2 H), 4.26 – 4.39 (m, 1 H), 4.99 (br. s, 1 H), 8.11 (d, J=2.01 Hz, 1 H), 8.56 (d, J=1.76 Hz, 1 H).
PAPER
- By Wylie, Andrew A.; Schoepfer, Joseph; Jahnke, Wolfgang; Cowan-Jacob, Sandra W.; Loo, Alice; Furet, Pascal; Marzinzik, Andreas L.; Pelle, Xavier; Donovan, Jerry; Zhu, Wenjing; et al
- From Nature (London, United Kingdom) (2017), 543(7647), 733-737.
By Wylie, Andrew A. et alFrom Nature (London, United Kingdom), 543(7647), 733-737; 2017
PAPER
- By Molica, Matteo; Massaro, Fulvio; Breccia, Massimo
- From Expert Opinion on Pharmacotherapy (2017), 18(1), 57-65.
PATENT
US 20170216289
PAPER
- By El Rashedy, Ahmed A.; Olotu, Fisayo A.; Soliman, Mahmoud E. S.
- From Chemistry & Biodiversity (2018), 15(3), n/a.

join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE

join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@amcrasto
/////////////////////////////////////////////////////////////////////////////////////////////////////
 |
|
| Clinical data | |
|---|---|
| Trade names | Scemblix |
| Other names | ABL001 |
| Routes of administration |
By mouth |
| Drug class | Tyrosine kinase inhibitor |
| ATC code |
|
| Legal status | |
| Legal status | |
| Identifiers | |
| CAS Number |
|
| PubChem CID | |
| IUPHAR/BPS | |
| DrugBank | |
| ChemSpider | |
| UNII |
|
| KEGG | |
| ChEMBL |
|
| PDB ligand | |
| Chemical and physical data | |
| Formula | C20H18ClF2N5O3 |
| Molar mass | 449.84 g·mol−1 |
| 3D model (JSmol) | |
References
- ^ Jump up to:a b c d “Scemblix- asciminib tablet, film coated”. DailyMed. Retrieved 4 November 2021.
- ^ Jump up to:a b c “FDA approves asciminib for Philadelphia chromosome-positive chronic myeloid leukemia”. U.S. Food and Drug Administration (FDA) (Press release). 29 October 2021. Retrieved 4 November 2021.
 This article incorporates text from this source, which is in the public domain.
This article incorporates text from this source, which is in the public domain. - ^ Breccia M, Colafigli G, Scalzulli E, Martelli M (August 2021). “Asciminib: an investigational agent for the treatment of chronic myeloid leukemia”. Expert Opinion on Investigational Drugs. 30 (8): 803–811. doi:10.1080/13543784.2021.1941863. PMID 34130563.
- ^ “Scemblix: FDA-Approved Drugs”. U.S. Food and Drug Administration (FDA). Retrieved 29 October 2021.
- ^ “FDA approves Novartis Scemblix (asciminib), with novel mechanism of action for the treatment of chronic myeloid leukemia”. Novartis (Press release). Retrieved 29 October 2021.
- ^ “Asciminib Orphan Drug Designations and Approvals”. U.S. Food and Drug Administration (FDA). 27 February 2017. Retrieved 29 October 2021.
- ^ “Novartis receives FDA Breakthrough Therapy designations for investigational STAMP inhibitor asciminib (ABL001) in chronic myeloid leukemia”. Novartis (Press release). 8 February 2020. Retrieved 29 October 2021.
External links
- “Asciminib”. Drug Information Portal. U.S. National Library of Medicine.
- Clinical trial number NCT02081378 for “A Phase I Study of Oral ABL001 in Patients With CML or Ph+ ALL” at ClinicalTrials.gov
- Clinical trial number NCT03106779 for “Study of Efficacy of CML-CP Patients Treated With ABL001 Versus Bosutinib, Previously Treated With 2 or More TKIs” at ClinicalTrials.gov
////////////////ABL001, Asciminib, ABL 001, ABL-001, PHASE 3, Chronic Myeloid Leukemia, NOVARTIS
O=C(NC1=CC=C(OC(F)(Cl)F)C=C1)C2=CN=C(N3C[C@H](O)CC3)C(C4=CC=NN4)=C2

NEW DRUG APPROVALS
one time
$10.00
Alpelisib, BYL 719
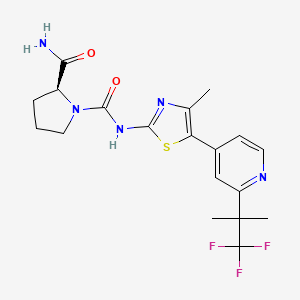
Alpelisib
(2S)-1-N-[4-methyl-5-[2-(1,1,1-trifluoro-2-methylpropan-2-yl)pyridin-4-yl]-1,3-thiazol-2-yl]pyrrolidine-1,2-dicarboxamide
PDT PAT WO 2010/029082
| Chemical Names: | Alpelisib; CAS 1217486-61-7; BYL-719; BYL719; UNII-08W5N2C97Q; BYL 719 |
|---|---|
| Molecular Formula: | C19H22F3N5O2S |
| Molecular Weight: | 441.473 g/mol |
- alpelisib
- 1217486-61-7
- BYL-719
- BYL719
- UNII-08W5N2C97Q
- BYL 719
- Alpelisib (BYL719)
- (S)-N1-(4-Methyl-5-(2-(1,1,1-trifluoro-2-methylpropan-2-yl)pyridin-4-yl)thiazol-2-yl)pyrrolidine-1,2-dicarboxamide
- NVP-BYL719
Alpelisib is an orally bioavailable phosphatidylinositol 3-kinase (PI3K) inhibitor with potential antineoplastic activity. Alpelisib specifically inhibits PI3K in the PI3K/AKT kinase (or protein kinase B) signaling pathway, thereby inhibiting the activation of the PI3K signaling pathway. This may result in inhibition of tumor cell growth and survival in susceptible tumor cell populations. Activation of the PI3K signaling pathway is frequently associated with tumorigenesis. Dysregulated PI3K signaling may contribute to tumor resistance to a variety of antineoplastic agents.
Alpelisib has been used in trials studying the treatment and basic science of Neoplasms, Solid Tumors, BREAST CANCER, 3rd Line GIST, and Rectal Cancer, among others.


SYN 2
POLYMORPHS
(S)-pyrrolidine-l,2-dicarboxylic acid 2-amide l-(4-methyl-5-[2-(2,2,2-trifluoro-l,l- dimethyl-ethyl)-pyridin-4-yl]-thiazol-2-yl)-amidei hereafter referred to as compound I,

is an alpha-selective phosphatidylinositol 3 -kinase (PI3K) inhibitor. Compound I was originally described in WO 2010/029082, wherein the synthesis of its free base form was described. There is a need for additional solid forms of compound I, for use in drug substance and drug product development. It has been found that new solid forms of compound I can be prepared as one or more polymorph forms, including solvate forms. These polymorph forms exhibit new physical properties that may be exploited in order to obtain new pharmacological properties, and that may be utilized in drug substance and drug product development. Summary of the Invention
In one aspect, provided herein is a crystalline form of the compound of formula I, or a solvate of the crystalline form of the compound of formula I, or a salt of the crystalline form of the compound of formula I, or a solvate of a salt of the crystalline form of the compound of formula I. In one embodiment, the crystalline form of the compound of formula I has the polymorph form SA, SB, Sc, or SD.
In another aspect, provided herein is a pharmaceutical composition comprising a crystalline compound of formula I. In one embodiment of the pharmaceutical composition, the crystalline compound of formula I has the polymorph form SA, SB,Sc, or So.
In another aspect, provided herein is a method for the treatment of disorders mediated by PI3K, comprising administering to a patient in need of such treatment an effective amount of a crystalline compound of formula I, particularly SA, SB, SC,or SD .
In yet another aspect, provided herein is the use of a crystalline compound of formula I, particularly SA, SB, SC, or SD, for the preparation of a medicament for the treatment of disorders mediated by PI3K.
In still another aspect, provided herein is a method for the treatment of disorders selected from benign or malignant tumor; a cancer selected from sarcoma; lung; bronchus; prostate; breast (including sporadic breast cancers and sufferers of Cowden disease);
pancreas; gastrointestinal cancer; colon; rectum; colon carcinoma; colorectal adenoma;
thyroid; liver; intrahepatic bile duct; hepatocellular; adrenal gland; stomach; gastric; glioma; glioblastoma; endometrial; melanoma; kidney; renal pelvis; urinary bladder; uterine corpus; uterine cervix; vagina; ovary; multiple myeloma; esophagus; a leukaemia; acute myelogenous leukemia; chronic myelogenous leukemia; lymphocytic leukemia; myeloid leukemia; brain; a carcinoma of the brain; oral cavity and pharynx; larynx; small intestine; non-Hodgkin lymphoma; melanoma; villous colon adenoma; a neoplasia; a neoplasia of epithelial character; lymphomas; a mammary carcinoma; basal cell carcinoma; squamous cell carcinoma; actinic keratosis; tumor diseases, including solid tumors; a tumor of the neck or head; polycythemia vera; essential thrombocythemia; myelofibrosis with myeloid metaplasia; and Walden stroem disease; as well as polycythemia vera, essential thrombocythemia, myelofibrosis with myeloid metaplasia, asthma, COPD, ARDS, Loffler’s syndrome, eosinophilic pneumonia, parasitic (in particular metazoan) infestation (including tropical eosinophilia), bronchopulmonary aspergillosis, polyarteritis nodosa (including Churg-Strauss syndrome), eosinophilic granuloma, eosinophil-related disorders affecting the airways occasioned by drug-reaction, psoriasis, contact dermatitis, atopic dermatitis, alopecia areata, erythema multiforme, dermatitis herpetiformis, scleroderma, vitiligo, hypersensitivity angiitis, urticaria, bullous pemphigoid, lupus erythematosus, pemphisus, epidermolysis bullosa acquisita, autoimmune haematogical disorders (e.g., haemolytic anaemia, aplastic anaemia, pure red cell anaemia and idiopathic thrombocytopenia), systemic lupus erythematosus, polychondritis, scleroderma, Wegener granulomatosis, dermatomyositis, chronic active hepatitis, myasthenia gravis, Steven-Johnson syndrome, idiopathic sprue, autoimmune inflammatory bowel disease (e.g., ulcerative colitis and Crohn’s disease), endocrine opthalmopathy, Grave’s disease, sarcoidosis, alveolitis, chronic hypersensitivity pneumonitis, multiple sclerosis, primary biliary cirrhosis, uveitis (anterior and posterior), interstitial lung fibrosis, psoriatic arthritis, glomerulonephritis, cardiovascular diseases, atherosclerosis, hypertension, deep venous thrombosis, stroke, myocardial infarction, unstable angina, thromboembolism, pulmonary embolism, thrombolytic diseases, acute arterial ischemia, peripheral thrombotic occlusions, and coronary artery disease, reperfusion injuries, retinopathy, such as diabetic retinopathy or hyperbaric oxygen-induced retinopathy, and conditions characterized by elevated intraocular pressure or secretion of ocular aqueous humor, such as glaucoma, comprising administering to a patient in need of such treatment an effective amount of the crystalline compound of formula I, particularly polymorph forms SA, SB, SC, or SD-
In another aspect, provided herein is the use of the crystalline compound of formula I, particularly polymorph forms SA, SB, SC, or SD for the preparation of a medicament for the treatment of the disorders listed above. Brief Description of the Drawings
Figure I depicts the X-ray powder diffraction pattern of polymorph form A. Figure II depicts the FT-IR spectrum of polymorph form A. Figure III depicts the differential scanning calorimetry thermogram of polymorph form A. Figure IV depicts the X-ray powder diffraction pattern of polymorph form SA- Figure V depicts the X-ray powder diffraction pattern of polymorph form SB. Figure VI depicts the X-ray powder diffraction pattern of polymorph form Sc. Figure VII depicts the X-ray powder diffraction pattern of polymorph form SD.
Scheme 2. Synthesis of (S)-Pyrrolidine-1.2-dicarboxylic acid 2-amide l-((4-methyl-5-r2- (2,2,2-trifluoro- 1 , 1 -dimethyl-ethyl -pyridin-4-yl1-thiazol-2-yl} -amide)

Example 2: (S)-Pyrrolidine-1.2-dicarboxylic acid 2-amide 1 -((4-methyl-5- 2 -(2,2,2- trifluoro-1 J-dirhethyl-ethylVpyridin-4-yl -thia2ol-2-yll-amide
The title compound is prepared in analogy to the procedure described in Example 1 but with the following modifications. In Step 2.1 (corresponding to Step 1.1 of Example 1), the reaction mixture is stirred for 14 h at reflux. In Step 2.2 (corresponding to Step 1.2 of Example 1), the reaction mixture is stirred for 1 h at 85 °C and extracted with ethyl acetate after being quenched. In step 2.3 (corresponding to Step 1.3 of Example 1), the reaction mixture is stirred for 2.5 h at 120 °C. In Step 2.4 (corresponding to Step 1.4 of Example 1), the reaction mixture is stirred for 1 h at 83 °C and extracted with ethyl acetate after being quenched. In Step 2.5 (corresponding to Step 1.5 of Example 1), the reaction mixture is stirred for 1 h at 65 °C and trituration in methanol is not performed. In Step 2.6
(corresponding to Step 1.6 of Example 1), the crude product is not purified. In Step 2.7 (corresponding to Step 1.7 of Example 1), 3,3,3-trifluoro-2,2-dimethyl-propionyl chloride is used.
Title compound: ESI-MS: 442.0 [M+H]+; tR= 3.02 min (System 1); TLC: Rf = 0.35 (DCM/MeOH, 9: 1).
Example 3: Preparation of Polymorph Form A
(S)-Pyrrolidine-l,2-dicarboxylic acid 2-amide l-({4-methyl-5-[2-(2,2,2-trifluoro-l,l- dimethyl-ethyl)-pyridin-4-yl]-thiazol-2-yl}-amide) (10.0 g) was suspended in ethanol/water (85:15 v/v; 75 mL) and the mixture was heated to 75 °C. The solution was clear-filtered into a second flask and the first flask was then washed with ethanol/water (4:6 v/v; 20 mL), followed by water (10 mL). The clear solution was stirred at 75 °C for an additional 30 minutes. The clear solution was then cooled to 2 °C over 2 hours and the obtained thick suspension was stirred at 2 °C for an additional hour. The mixture was then filtered, and the flask and filter cake were washed with ethanol/water (1 :1 v/v; 20 mL), followed by ethyl acetate (10 mL). The wet filter cake was returned to the flask and suspended in ethyl acetate (75 mL). the mixture was heated to 78 °C and was stirred under reflux for 1 hour. During this time, 15 mL ethyl acetate was distilled off. The mixture was then cooled to 2 °C over 2 hours and the suspension was stirred at 2 °C for an additional hour. The mixture was filtered, and the flask and filter cake were washed with cold ethyl acetate (12 mL). The filter cake was then dried under 1-50 mbar vacuum at 50 °C to yield the polymorph form A (7.3 g).
| Patent ID | Patent Title | Submitted Date | Granted Date |
|---|---|---|---|
| US9815898 | ANTIBODY MOLECULES TO PD-1 AND USES THEREOF |
2017-05-15
|
|
| US2017210733 | BENZOXAZEPIN OXAZOLIDINONE COMPOUNDS AND METHODS OF USE |
2017-04-07
|
|
| US2017210804 | ANTIBODY MOLECULES TO LAG-3 AND USES THEREOF |
2017-03-24
|
|
| US2017190777 | ANTIBODY MOLECULES TO TIM-3 AND USES THEREOF |
2017-03-17
|
|
| US2017166550 | BENZOTHIOPHENE-BASED SELECTIVE ESTROGEN RECEPTOR DOWNREGULATORS |
2016-12-09
|
| Patent ID | Patent Title | Submitted Date | Granted Date |
|---|---|---|---|
| US2016117439 | SUPERIOR BIOINFORMATICS PROCESS FOR IDENTIFYING AT RISK SUBJECT POPULATIONS |
2015-10-26
|
2016-04-28
|
| US2017096492 | DOSAGE AND ADMINISTRATION OF ANTI-IGF-1R, ANTI-ErbB3 BISPECIFIC ANTIBODIES, USES THEREOF AND METHODS OF TREATMENT THEREWITH |
2016-08-19
|
|
| US2017165246 | PHARMACEUTICAL COMBINATIONS COMPRISING A PI3K INHIBITOR FOR THE TREATMENT OF CANCER |
2015-02-10
|
|
| US9474754 | Pharmaceutical Combinations Comprising a B-RAF Inhibitor, and EGFR Inhibitor and Optionally a PI3K-Alpha Inhibitor |
2013-08-05
|
2015-09-24
|
| US2015111927 | PHARMACEUTICAL DIAGNOSTIC |
2013-03-27
|
2015-04-23
|
from PubChem
from PubChem
/////////////////Alpelisib, CAS, 1217486-61-7, BYL-719, BYL719, UNII-08W5N2C97Q, BYL 719
CC1=C(SC(=N1)NC(=O)N2CCCC2C(=O)N)C3=CC(=NC=C3)C(C)(C)C(F)(F)F
Capmatinib, капматиниб , كابماتينيب , 卡马替尼 ,

Capmatinib / INC280/ INCB 28060
INC280 / INCB-28060 FREE BASE
UNIITY34L4F9OZ
CAS number 1029712-80-8
WeightAverage: 412.428
Chemical FormulaC23H17FN6O
2-fluoro-N-methyl-4-{7-[(quinolin-6-yl)methyl]imidazo[1,2-b][1,2,4]triazin-2-yl}benzamide
Capmatinib dihydrochloride; CAS 1197376-85-4
1029712-80-8 [RN]
2-Fluoro-N-méthyl-4-[7-(6-quinoléinylméthyl)imidazo[1,2-b][1,2,4]triazin-2-yl]benzamide [French] [ACD/IUPAC Name]
капматиниб [Russian] [INN]
كابماتينيب [Arabic] [INN]
卡马替尼 [Chinese] [INN]
Scheme 1



Scheme 2

Method C
![]()



Capmatinib has been used in trials studying the treatment of Melanoma, Gliosarcoma, Solid Tumors, Colorectal Cancer, and Hepatic Impairment, among others.
Capmatinib is an orally bioavailable inhibitor of the proto-oncogene c-Met (also known as hepatocyte growth factor receptor (HGFR)) with potential antineoplastic activity. Capmatinib selectively binds to c-Met, thereby inhibiting c-Met phosphorylation and disrupting c-Met signal transduction pathways. This may induce cell death in tumor cells overexpressing c-Met protein or expressing constitutively activated c-Met protein. c-Met, a receptor tyrosine kinase overexpressed or mutated in many tumor cell types, plays key roles in tumor cell proliferation, survival, invasion, metastasis, and tumor angiogenesis.
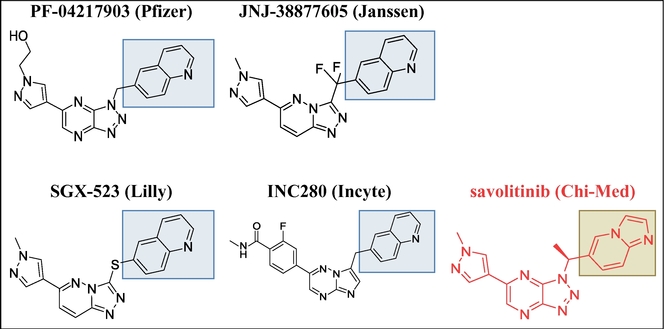
Capmatinib has been used in trials studying the treatment of Melanoma, Gliosarcoma, Solid Tumors, Colorectal Cancer, and Hepatic Impairment, among others
Protein kinases (PKs) are a group of enzymes that regulate diverse, important biological processes including cell growth, survival and differentiation, organ formation and morphogenesis, neovascularization, tissue repair and regeneration, among others. Protein kinases exert their physiological functions through catalyzing the phosphorylation of proteins (or substrates) and thereby modulating the cellular activities of the substrates in various biological contexts, hi addition to the functions in normal tissues/organs, many protein kinases also play more specialized roles in a host of human diseases including cancer. A subset of protein kinases (also referred to as oncogenic protein kinases), when dysregulated, can cause tumor formation and growth, and further contribute to tumor maintenance and progression (Blume- Jensen P et al, Nature 2001, 411(6835):355-365). Thus far, oncogenic protein kinases represent one of the largest and most attractive groups of protein targets for cancer intervention and drug development. c-Met, a proto-oncogene, is a member of a distinct subfamily of heterodimeric receptor tyrosine kinases which include Met, Ron, and Sea (Birchmeier, C. et al., Nat. Rev. MoI. Cell Biol. 2003, 4(12):915-925; Christensen, J. G. et al., Cancer Lett. 2005, 225(1): 1-26). The only high affinity ligand for c-Met is the hepatocyte growth factor (HGF), also known as scatter factor (SF). Binding of HGF to c-Met induces activation of the receptor via autophosphorylation resulting in an increase of receptor dependent signaling. Both c-Met and HGF are widely expressed in a variety of organs, but their expression is normally confined to the cells of epithelial and mesenchymal origin, respectively. The biological functions of c-Met (or c-Met signaling pathway) in normal tissues and human malignancies such as cancer have been well documented (Christensen, J.G. et al., Cancer Lett. 2005, 225(l):l-26; Corso, S. et al., Trends in MoI. Med. 2005, l l(6):284-292).
HGF and c-Met are each required for normal mammalian development, and abnormalities reported in both HGF- and c-Met-null mice are consistent with proximity of embryonic expression and epithelial-mesenchymal transition defects during organ morphogenesis (Christensen, J.G. et al., Cancer Lett. 2005, 225(1): 1-26). Consistent with these findings, the transduction of signaling and subsequent biological effects of HGF/c-Met pathway have been shown to be important for epithelial-mesenchymal interaction and regulation of cell migration, invasion, cell proliferation and survival, angiogenesis, morphogenesis and organization of three-dimensional tubular structures (e.g. renal tubular cells, gland formation) during development. The specific consequences of c-Met pathway activation in a given cell/tissue are highly context-dependent.
Dysregulated c-Met pathway plays important and sometimes causative (in the case of genetic alterations) roles in tumor formation, growth, maintenance and progression (Birchmeier, C. et al., Nat. Rev. MoI. Cell. Biol. 2003, 4(12):915-925; Boccaccio, C. et al., Nat. Rev. Cancer 2006, 6(8):637-645; Christensen, J.G. et al., Cancer Lett. 2005, 225(1): 1-26). HGF and/or c-Met are overexpressed in significant portions of most human cancers, and are often associated with poor clinical outcomes such as more aggressive disease, disease progression, tumor metastasis and shortened patient survival. Further, patients with high levels of HGF/c-Met proteins are more resistance to chemotherapy and radiotherapy, hi addition to the abnormal HGF/c-Met expression, c-Met receptor can also be activated in cancer patients through genetic mutations (both germline and somatic) and gene amplification. Although gene amplification and mutations are the most common genetic alterations that have been reported in patients, the receptor can also be activated by deletions, truncations, gene rearrangement, as well as abnormal receptor processing and defective negative regulatory mechanisms.
The various cancers in which c-Met is implicated include, but are not limited to: carcinomas (e.g., bladder, breast, cervical, cholangiocarcinoma, colorectal, esophageal, gastric, head and neck, kidney, liver, lung, nasopharygeal, ovarian, pancreas, prostate, thyroid); musculoskeletal sarcomas (e.g., osteosarcaoma, synovial sarcoma, rhabdomyosarcoma); soft tissue sarcomas (e.g., MFH/fibrosarcoma, leiomyosarcoma, Kaposi’s sarcoma); hematopoietic malignancies (e.g., multiple myeloma, lymphomas, adult T cell leukemia, acute myelogenous leukemia, chronic myeloid leukemia); and other neoplasms (e.g., glioblastomas, astrocytomas, melanoma, mesothelioma and Wilm’s tumor (www.vai.org/met/; Christensen, J. G. et al., Cancer Lett. 2005, 225(1): 1-26).
The notion that the activated c-Met pathway contributes to tumor formation and progression and could be a good target for effective cancer intervention has been further solidified by numerous preclinical studies (Birchmeier, C. et al., Nat. Rev. MoI. Cell Biol. 2003, 4(12):915-925; Christensen, J.G. et al., Cancer Lett. 2005, 225(l):l-26; Corso, S. et al., Trends in MoI. Med. 2005, 11(6):284-292). For example, studies showed that the tpr-met fusion gene, overexpression oϊc-met and activated c-met mutations all caused oncogenic transformation of various model cell lines and resulted in tumor formation and metastasis in mice. More importantly, significant anti-tumor (sometimes tumor regression) and anti-metastasis activities have been demonstrated in vitro and in vivo with agents that specifically impair and/or block HGF/c-Met signaling. Those agents include anti-HGF and anti-c-Met antibodies, HGF peptide antagonists, decoy c-Met receptor, c-Met peptide antagonists, dominant negative c-Met mutations, c-Met specific antisense oligonucleotides and ribozymes, and selective small molecule c-Met kinase inhibitors (Christensen, J.G. et al., Cancer Lett. 2005, 225(1): 1-26).
In addition to the established role in cancer, abnormal HGF/c-Met signaling is also implicated in atherosclerosis, lung fibrosis, renal fibrosis and regeneration, liver diseases, allergic disorders, inflammatory and autoimmune disorders, cerebrovascular diseases, cardiovascular diseases, conditions associated with organ transplantation (Ma, H. et al., Atherosclerosis. 2002, 164(l):79-87; Crestani, B. et al., Lab. Invest. 2002, 82(8):1015-1022; Sequra-Flores, A. A. et al., Rev. Gastroenterol. Mex. 2004, 69(4)243-250; Morishita, R. et al., Curr. Gene Ther. 2004, 4(2)199-206; Morishita, R. et al., Endocr. J. 2002, 49(3)273-284; Liu, Y., Curr. Opin. Nephrol. Hypertens. 2002, l l(l):23-30; Matsumoto, K. et al., Kidney Int. 2001, 59(6):2023-2038; Balkovetz, D.F. et al., Int. Rev. Cytol. 1999, 186:225-250; Miyazawa, T. et al., J. Cereb. Blood Flow Metab. 1998, 18(4)345-348; Koch, A.E. et al., Arthritis Rheum. 1996, 39(9):1566-1575; Futamatsu, H. et al., Circ. Res. 2005, 96(8)823-830; Eguchi, S. et al., Clin. Transplant. 1999, 13(6)536-544).
Inhibitors of c-Met and other kinases are reported in U.S. Ser. No. 11/942,130, including the compound 2-fluoro-N-methyl-4-[7-(quinolin-6-ylmethyl)imidazo[l ,2-b][l ,2,4]triazin-2-yl]benzamide (I) having the structure indicated below.

(I)
New or improved forms of existing agents which inhibit kinases such as c-Met are continually needed for developing more effective pharmaceuticals to treat cancer and other diseases. The salts, compositions, and methods described herein are directed toward these needs and other ends.
PATENT
Example 8 4-Bromo-3-fluoro-N-methoxy-iV-methylbenzamide (3)
To a suspension of 4-bromo-3-fluorobenzoic acid (1, 967.9 g, 4.4 mol) in dichloromethane (5.9 L) and DMF (21 mL) was slowly added a solution of oxalyl chloride ((COCl)2, 560 mL, 6.4 mol, 1.45 equiv) in dichloromethane (520 mL) at room temperature. The resulting reaction mixture was stirred at room temperature for 20 h and then cooled to 0 0C by ice-water bath. iV,0-dimethyl hydroxylamine hydrochloride (826 g, 8.4 mol, 1.9 equiv) was added followed by slow addition of triethylamine (TEA, 2.5 L, 17.7 mol, 4.0 equiv) at 0 0C. The reaction mixture was then gradually warmed to room temperature and stirred at room temperature overnight. Once the coupling reaction was complete, the reaction mixture was washed with saturated aqueous sodium bicarbonate solution (NaHCO3, 2 L). The aqueous phase was back extracted with dichloromethane (1 L). The combined organic phases were washed with water (1 L), brine (1 L), and concentrated under reduced pressure. The resulting solid residue was dissolved into methyl tert-butyl ether (MTBE, 5 L), washed sequentially with water (5 x 1 L), brine (1 L), and dried over anhydrous sodium sulfate (Na2SO4). The filtrated solution was concentrated under reduced pressure and the resulting solid was dried in a vacuum oven at 45 0C to afford 4-bromo-3-fluoro-Λr-methoxy-Λr-methylbenzamide (3, 1106 g, 1153 g theoretical, 95.9% yield) which was used for the subsequent reaction without further purification. For 3: 1H NMR (400 MHz, DMSO-J6) δ ppm 7.78 (t, IH, J= 7.47 Hz), 7.56 (dd, IH, J= 9.3, 1.6 Hz), 7.18 (d, IH, J= 8.1 Hz), 3.53 (s, 3H), 3.25(s, 3H); C9H9BrFNO2 (MW 262.08), LCMS (EI) mle 262.0/ 264.0 (M+ + H).
Scheme 1 (Examples 8-14)
C7H4BrFO2 C7H3BrCIFO C9H9BrFNO2 MoI. Wt: 219.01 MoI. Wt: 237.45 MoI. Wt: 26208
C8H6BrFO C8H4BrFO2 Ci2Hi4BrFO3 MoI. Wt: 217.04 MoI. Wt: 231.02 MoI. Wt: 305.14
13
C22H13FN3 MoI. Wt: 380.38
Example 9 l-(4-Bromo-3-fluorophenyl)ethanone (4)
To a solution of crude 4-bromo-3-fluoro-N-methoxy-iV-methylbenzamide (3, 1106 g, 4.2 mol) in anhydrous tetrahydrofuran (THF, 11 L) was slowly added a 3.0 M solution of methylmagnesium chloride (MeMgCl, 2.5 L, 7.5 mol, 1.7 equiv) in THF at 0 0C. The resulting reaction mixture was stirred at 0 0C for 2 h and then quenched very carefully with saturated aqueous ammonium chloride (NH4Cl, 1.5 L). The resulting solution was concentrated under reduced pressure to remove most of THF. The residue was then diluted with ethyl acetate (EtOAc, 5 L) and the resulting solution was washed with water (2 L). The aqueous phase was extracted with ethyl acetate (EtOAc, 2 x 2 L). The combined organic phases were washed with water (2 L), brine (2 L) and dried over anhydrous sodium sulfate (Na2SO4). The filtered solution was concentrated under reduced pressure and the resulting solid was dried in a vacuum oven at 45 0C to afford l-(4-bromo-3-fluorophenyl)ethanone (4, 890.8 g, 911.6 g theoretical, 97.7% yield) as a solid which was used in the subsequent reaction without further purification. For 4: 1H NMR (400 MHz, OMSO-d6) δ ppm 7.89-7.84 (m, 2H), 7.71 (dd, IH, J= 8.30, 1.87 Hz), 2.57 (s, 3H).
Example 10 2-(4-Bromo-3-fluorophenyl)-2-oxoacetaldehyde (5)
To a solution of l-(4-bromo-3-fluorophenyl)ethanone (4, 890.8 g, 4.1 mol) in DMSO (4 L) was slowly added a solution of 48% aqueous hydrogen bromide (HBr, 1420 mL, 12.5 mol, 3.0 equiv). The reaction temperature was gradually increased from 2O0C to 50 0C during the course of the addition. The reaction mixture was subsequently heated to 60 0C and stirred at 60 0C overnight. The resulting dimethyl sulfide was removed by distillation and the residue was poured into ice water (28 L). The resulting yellow precipitate was collected by filtration (save the filtrate) and washed with water (5 L). The yellow solid was dissolved in ethyl acetate (EtOAc, 5 L), washed with brine (1 L) and dried over anhydrous sodium sulfate (Na2SO4). The solution was then concentrated under the reduced pressure and the resulting solid was dried in a vacuum oven at 45 0C to give the desired product, 2-(4-bromo-3-fluorophenyl)-2-oxoacetaldehyde, as its hydrate (hydrate of 5, 730.6 g, 1020.9 g theoretical, 71.6% yield). The aqueous phase (filtrate) was extracted with ethyl acetate (3 x 5 L) and the combined organic phase was washed with water (2 x 2 L), brine (2 L) and dried over anhydrous sodium sulfate (Na2SO4). The solution was concentrated under reduced pressure and the resulting solid was dried in a vacuum oven at 45 0C to give the second crop of 2-(4-bromo-3-fluorophenyl)-2-oxoacetaldehyde hydrate (hydrate of 5, 289.4 g, 1020.9 g theoretical, 28.3% yield; total 1020 g, 1020.9 g theoretical, 99.9% yield) which was used in the subsequent reaction without further purification. For hydrate of 5: H NMR (400 MHz, DMSO-</6) δ ppm 8.00-7.70 (m, 3H), 6.69 (br s, 2H), 5.59 (s, IH).
Example 11 l-(4-Bromo-3-fluorophenyl)-2,2-diethoxyethanone (6)
A 22 L flask was charged with the hydrate of (4-bromo-3-fluorophenyl)-2-oxoacetaldehyde (5, 1020 g, 4.41 mol), toluene (7.5 L), triethyl orthoformate (1633 g, 1.8 L, 11.04 mol, 2.5 equiv), para-toluene sulfonic acid (33.5 g, 0.176 mol, 0.4 equiv) at room temperature, and the resulting reaction mixture was heated to 110 0C and stirred at 1 10 0C for 6 h. When HPLC showed that the reaction was complete, the reaction mixture was cooled down to room temperature before being poured into a 50 L separation funnel along with ethyl acetate (7.5 L) and the saturated aqueous sodium bicarbonate solution (NaHCO3, 3 L). The mixture was stirred and the layers were separated. The aqueous layer was extracted with ethyl acetate (2 L). The combined organic layers were washed with brine (4 L), dried with sodium sulfate (Na2SO4), and concentrated under the reduced pressure to afford crude l-(4-bromo-3-fluorophenyl)-2,2-diethoxyethanone (6, 1240 g, 1345.7 g theoretical, 92.1% yield) which was used in the subsequent reaction without further purification. For 6: 1H NMR (400 MHz, DMSO-J6) δ ppm 7.94-7.94 (m, 2H), 7.78 (dd, IH, J= 8.51, 2.08 Hz), 5.40 (s, IH), 3.77-3.60 (m, 4H), 1.16-1.14 (m, 6H).
Example 12 6-(4-Bromo-3-fluorophenyl)-l,2,4-triazin-3-amine (7)
A 22 L flask was charged with l-(4-bromo-3-fluorophenyl)-2,2-diethoxyethanone (6, 1240 g, 4.07 mol), ethanol (11 L), water (1.4 L), potassium hydroxide (KOH, 910 g, 16.3 mol, 4.0 equiv), and aminoguanidine bicarbonate (1105 g, 8.13 mol, 2.0 equiv) at room temperature. The resulting reaction mixture was then heated to 75 0C for 14 h. When HPLC showed the condensation reaction was deemed complete, the reaction mixture was cooled down to room temperature before being filtered. The filtrate was then concentrated under the reduced pressure to remove the most of the solvents. The residual aqueous solution was extracted with ethyl acetate (EtOAc, 3 x 6 L). The organic layers were combined and concentrated under the reduced pressure to give a dark brown solid. This solid was dissolved in ethanol (4 L) and the resulting solution was treated with a solution of 0.2 M aqueous hydrochloric acid solution (4 L). The resulting slurry was subsequently heated to 50 0C for 6 h before being allowed to cool down to room temperature. A solution of saturated aqueous sodium bicarbonate solution (NaHCO3, 2 L) was slowly added to the slurry and the resulting mixture was then concentrated under the reduced pressure to remove most of the solvents. The aqueous residue was then treated with ethyl acetate (20 L) to dissolve the solids. The two layers were separated and the aqueous layer was extracted with ethyl acetate (2 x 2 L). The combined organic layers were concentrated under the reduced pressure. The dark brown solids were treated with methyl ter/-butyl ether (MTBE, 4 L) and the resulting slurry was heated to 30 0C and stirred at 30 0C for 30 min. The mixture was filtered and the solids (green to orange in color) were collected (save the filtrate) and washed with methyl tert-buty\ ether (MTBE, 2 L) to give the first crop of the crude desired product (7). The filtrate was evaporated under the reduced pressure, and the resulting dark brown solids were treated with methyl tert-butyl ether (MTBE, 2 L). The resulting slurry was heated to 30 0C and stirred at 30 0C for 30 min. The mixture was filtered to give the second crop of the crude desired product (7) which was washed with MTBE (1 L). The combined solids were dried in vacuum at 40 – 45 0C to afford 6-(4-bromo-3-fluorophenyl)-l,2,4-triazin-3-amine (7, 585 g, 1095.1 g theoretical, 53.4 % yield) which was used in the subsequent reaction without further purification. For 7: 1H NMR (400 MHz, DMSO-J6) δ ppm 8.86 (s, IH), 7.97 (d, IH, J= 10.79 Hz), 7.81 (m, 2H), 7.52 (br s, 2H); C9H6BrFN4 (MW 269.07), LCMS (EI) mle 269.0/271.1 (M+ + H).
Example 13 6-((2-(4-Bromo-3-fluorophenyl)imidazo[l,2-6][l,2,4]triazin-7-yl)methyl)quinoline (12) l-(2-Chloro-l-hydroxy-3-(quinolin-6-yl)propyl)pyrrolidine-2,5-dione (11, 228 g, 0.74 mol, 1.1 equiv) and 6-(4-bromo-3-fluorophenyl)-l,2,4-triazin-3-amine (7, 181 g, 0.673 mol) were suspended in 1-butanol (1800 mL) and the resulting suspension was heated to 110 0C and stirred at 110 0C for 18 h (the reaction mixture becomes homogeneous at this point). The reaction mixture was then gradually cooled down to room temperature before being further cooled down to 10 0C in an ice bath. The resulting yellow solid was collected by filtration (save the 1 -butanol filtrates), washed with cold 1-butanol (3 x 100 mL) and dried by suction. This solid was then suspended in the saturated aqueous sodium bicarbonate solution (NaHCO3, 500 mL) and the resulting suspension was stirred at room temperature for 1 h to neutralize the corresponding hydrochloride salt. The free base was then filtered, washed with water (500 mL) and dried in a vacuum oven at 45 0C for 18 h to afford the first crop of the crude 6-((2-(4-bromo-3-fluorophenyl)imidazo[l,2-6][l,2,4]triazin-7-yl)methyl)quinoline (12, 125.1 g, 292.3 g theoretical, 42.8% yield). The 1-butanol filtrates were then concentrated under the reduced pressure and the resulting solids were dissolved in dichloromethane (CH2Cl2, 2 L). The solution was wash with the saturated aqueous sodium bicarbonate solution (NaHCO3, 1 L), dried over sodium sulfates (Na2SO4), and concentrated under the reduced pressure. The residue was then purified by flash column chromatography (SiO2, O – 10% MeOH-CH2Cl2 gradient elution) to afford the second crop of 6-((2-(4-bromo-3-fluorophenyl)imidazo[l,2-&][l ,2,4]triazin-7-yl)methyl)-quinoline (12, 19.7 g, 292.3 g theoretical, 6.7% yield; total 144.8 g, 292.3 g theoretical, 49.5% yield) as yellow solids. For 12: 1H NMR (400 MHz, DMSO-^6) δ ppm 9.23 (s, IH), 9.11 (dd, IH, J= 4.98, 1.55 Hz), 8.85 (d, IH, J= 8.09 Hz), 8.25 – 8.18 (m, 2H), 8.12 -8.00 (m, 3H), 7.93 – 7.86 (m, 3H), 4.70 (s, 2H); C21H13BrFN5 (MW 434.26), LCMS (EI) mle 434.00/435.95 (M+ + H).
Example 14 2-Fluoro-4-(7-(quinolin-6-ylmethyl)imidazo[l,2-6][l,2,4]triazin-2-yl)benzonitrile (13)
6-((2-(4-Bromo-3-fluorophenyl)imidazo[ 1 ,2-b] [ 1 ,2,4]triazin-7-yl)methyl)quinoline (12, 200 g, 0.461 mol), zinc cyanide (ZnCN2, 32.7 g, 0.277 mol, 0.6 equiv), zinc powder (Zn, 6.0 g, 0.093 mol, 0.2 equiv) and Pd(dppf)2Cl2 (22.6 g 0.028 mol, 0.06 eqiv) were suspended in premixed solution of ΛyV-dimethyl acetamide (DMAC, 2000 mL) and water (H2O, 40 mL). The resulting suspension was then degassed with a stream of nitrogen for 20 min before being heated to 110 0C and stirred at 110 0C for 1 – 2 h (homogeneous solution was observed). When LC/MS indicated the reaction was deemed complete, the reaction mixture was cooled first to room temperature and then in an ice bath to 5 0C. The cooled reaction mixture was diluted with a mixture of the saturated aqueous ammonium chloride solution (aq. NH4Cl), the concentrated ammonium hydroxide aqueous solution (aq. NH4OH), and water (4:1 :4 by volumn, 8.1 L) and the resulting mixture was stirred at room temperature for 30 min. The resulting solids were collected by filtration and dried in a vacuum oven overnight at 45 0C to afford the crude desired product (13). This crude material was then purified by flash chromatography (SiO2, gradient elution with 1% triethylamine in dichloromethane, 2.5 % acetone and 1% triethylamine in dichloromethane, 5.0 % acetone and 1% triethylamine in dichloromethane, and 10.0 % acetone and 1% triethylamine in dichloromethane sequentially) to afford the pure 2-fluoro-4-(7-(quinolin-6-ylmethyl)-imidazo[l,2-έ][l,2,4]triazin-2-yl)benzonitrile (13, 127.4 g, 175.4 g theoretical, 72.6% yield) as yellow solids. For 13: 1H NMR (400 MHz, DMSO-^6) δ ppm 9.24 (s, IH), 8.81 (dd, IH, J= 4.15, 1.66 Hz), 8.26 – 8.12 (m, 4H), 8.02 (s, IH), 7.95 – 7.93 (m, 2H), 7.76 (dd, IH, J= 8.71, 2.08 Hz), 7.47 (dd, IH, J= 8.70, 4.15 Hz), 4.62 (s, 2H); C22HnFN6 (MW 380.38), LCMS (EI) mle 381.0 (M+ + H).
Example 15 6-(3,3-Diethoxyprop-l-ynyl)quinoline (22)
A mixture of 6-bromoquinoline (8, 2.63 g, 12.6 mmol), propargylaldehyde diethyl acetal (3.73 niL, 25.2 mmol, 2.0 equiv), triethylamine (TEA, 12.7 mL, 90.8 mmol, 7.2 equiv), copper(I) iodide (CuI, 24.0 mg, 0.126 mmol, 0.01 equiv), and triphenylphosphine (PPh3, 0.39716 g, 1.5142 mmol, 0.12 equiv) in JV^V-dimethylformamide (DMF, 15.6 mL, 202 mmol) was degassed with nitrogen bubbling for 5 min. Palladium acetate (Pd(OAc)2, 0.08499 g, 0.3786 mmol, 0.03 equiv) was added and the mixture was degassed with nitrogen bubbling for 5 min. The reaction mixture was heated to 90 0C under nitrogen with stirring. After 3 h and 10 min, HPLC indicated that the reaction was complete. The reaction mixture was diluted with ethyl acetate (EtOAc, 100 mL) and washed with water (H2O, 2 x 100 mL). The aqueous layer was extracted with ethyl acetate (EtOAc, 20 mL). The combined organic extracts were then concentrated under the reduced pressure to give the crude product as a black oil. The crude product was purified by flash column chromatography (SiO2, 0 – 40% EtOAc in hexane gradient elution) to afford 6-(3,3-diethoxyprop-l-ynyl)quinoline (22, 3.2 g, 3.22 g theoretical, 99% yield) as a colorless oil. For 22: 1H NMR (400 MHz, OMSO-d6) δ ppm 8.92 (dd, IH, J= 4.35 Hz, 1.86 Hz), 8.36 (d, IH, J= 8.40 Hz, 1.66 Hz), 8.20 (d, IH, J= 1.78 Hz), 7.99 (d, IH, J= 8.71 Hz), 7.76 (dd, IH, J= 8.71 Hz, 1.87 Hz), 7.57 (dd, IH, J= 8.09 Hz, 4.05 Hz), 5.58 (s, IH), 3.75 – 3.55 (m, 4H), 1.17 (t, 6H, J= 7.16 Hz); Ci6H17NO2 (MW 255.31), LCMS (EI) m/e 256.0 (M+ + H).
Scheme 2 (Examples 15-18)
Method C
![]()
Example 16 6-(3,3-Diethoxypropyl)quinoline (23)
Method A. 3,3-Diethoxy-l-propene (548 g, 4.2 mol, 1.75 equiv) was added to a 22 L flask charged with 0.5 M solution of 9-borabicyclo[3.3.1] nonane in tetrahydrofuran (9-BBN solution in THF, 8.4 L, 4.2 mol, 1.75 equiv) at room temperature (the internal temperature raised to 40 0C) over 1 h.. The resulting reaction mixture was stirred at room temperature for overnight. At which time 1H NMR of an aliquot of the reaction mixture indicated that all the 3,3-diethoxy-1-propene had been consumed. 6-Bromoquinoline (8, 500 g, 2.4 mol, 1.0 equiv), potassium carbonate (K2CO3, 662 g, 4.8 mol, 2.0 equiv), tricyclohexylphosphine (67.4 g, 0.24 mol, 0.1 equiv), palladium acetate (Pd(OAc)2, 27 g, 0.12 mol, 0.05 equiv) and water (90 mL) were added to the reaction mixture in that order followed by degassing with nitrogen for 0.5 h. The reaction mixture was then heated to reflux for 4 h. Once TLC and LC/MS showed that the starting material had been consumed, the reaction mixture was cooled to room temperature with stirring before being quenched with water (7.5 L) and ethyl acetate (EtOAc, 7.5 L). The layers were separated and the aqueous layer was extracted with ethyl acetate (EtOAc, 4 L). The combined organic layers were washed with a saturated brine solution (NaCl, 4 L), dried over magnesium sulfate (MgSO4) and concentrated under the reduced pressure. The residue was purified by column chromatography (SiO2, 10 – 60% of ethyl acetate in heptane gradient elution) to afford 6-(3,3-diethoxypropyl)quinoline (23, 520 g, 622.4 g theoretical, 83.5% yield) as a colorless oil. For 23: 1HNMR (DMSO-</6, 300MHz) δ ppm 8.81 (dd, IH, J= 4.23 Hz, 1.73 Hz), 8.28 (d, IH, J= 8.07 Hz), 7.91 (d, IH, J= 8.62 Hz ), 7.75 (s, IH), 7.61 (dd, lH, J= 8.63 Hz, 1.92 Hz), 7.46 (dd, IH, J= 8.25 Hz, 4.22 Hz), 4.46 (t, IH, J= 5.60 Hz), 3.61 – 3.38 (m, 4H), 2.79 (t, 2H, J= 8.53 Hz), 1.95 -1.85 (m, 2H), 1.11 (t, 6H, J= 6.84 Hz); Ci6H21NO2 (MW 259.34), LCMS (EI) m/e 260.2 (M+ + H).
Method A-Alternative. 9-BBN was generated in situ and used to prepare compound 23 as discribed as follows: under a nitrogen atmosphere anhydrous 1 ,2-dimethoxyethane (DME, 47.0 mL) was charged into a 500 mL 3-neck flask equipped with a distillation apparatus. Borane-dimethyl sulfide complex (12.1 g, 151 mmol, 2 equiv) was added and the solution temperature increased from 20 to 22 0C. To this solution, 1 ,5-cyclooctadiene (16.3 g, 151 mmol, 2 equiv) was added dropwise over a period of 30 min to maintain a reaction temperature of 50 – 60 0C, during which time a small amount of dimethyl sulfide was collected by the distillation apparatus. The reaction mixture was then distilled under nitrogen until the distillate temperature reach 84 0C. The distillates collected had a volume of ~ 21 mL. The oil bath was removed and anhydrous THF (49 mL) was added. A small sample of the reaction mixture was taken for 1H NMR analysis and the result indicated the olefin was consumed. This 9-BBN solution was used directly for the next step.
To the above 9-BBN solution, 3,3-diethoxy-l-propene (19.3 g, 142 mmol, 1.89 equiv) was added dropwise while maintaining the temperature below 30 0C. The reaction is slightly exothermal and white precipitate slowly dissolved. The reaction mixture was then stirred at room temperature for 18 h.
To the solution prepared above, 6-bromoquinoline (8, 15.7 g, 75.4 mmol, 1 equiv), tricyclohexylphosphine (1.27 g, 4.52 mmol, 0.06 equiv), potassium carbonate (20.8 g, 151 mmol, 2 equiv), and water (0.421 mL, 23.4 mmol) were added. The mixture was degassed with nitrogen bubbling for 10 – 15 min. Palladium acetate (Pd(OAc)2, 0.508 g, 2.26 mmol, 0.03 equiv) was added and the nitrogen bubbling was continued for an additional 10 min. The reaction mixture was heated to 75 0C and maintained at 75 – 78 0C for 2 – 3 h. When HPLC showed the completion of the reaction, the heating was discontinued and the reaction mixture was cooled to room temperature. Ethyl acetate (EtOAc, 162 mL) and water (H2O, 162 mL) were added and the organic layer was separated. The aqueous layer was extracted with ethyl acetate (EtOAc, 2 x 60 mL) and the combined organic extracts were dried over sodium sulfate (Na2SO4) and concentrated under the reduced pressure. The residue was purified by flash column chromatography (silica gel, 0 – 40% EtOAc in hexane gradient elution) to afford 6-(3,3-diethoxypropyl)quinoline (23, 17.6 g, 19.6 g theoretical, 90% yield) as a clear oil, which was found to be identical to the meterial made from Method A in every comparable aspect.
Method B. A mixture of 6-(3,3-diethoxyprop-l-yn-l-yl)quinoline (22, 56 mg, 0.22 mmol) and 10% palladium on carbon (5 mg) in THF (5 mL) was hydrogenated under H2 at 1 atm for 6 h. The reaction mixture was filtered through a celite bed and the celite bed was washed with THF (2 x 2 mL). The combined filtrates were concentrated under the reduced pressure to afford 6-(3,3-diethoxypropyl)quinoline (23, 56 mg, 57 mg theoretical, 98% yield) as a clear oil, which was found to be sufficiently pure to be used in the subsequent reaction without further purification and was identical to the meterial made from Method A in every comparable aspect.
Example 17 3-(Quinolin-6-yl)propanal (9)
Method 1. A 22 L flask was charged with tris(dibenzylideneacetone)dipalladium(0) (70.0 g, 0.076 mol, 0.015 equiv), tri-tert-butylphosphonium tetrafluoroborate (44 g, 0.152 mol, 0.03 equiv), and dioxane (12 L) at room temperature. The resulting solution was then degassed with a steady stream of nitrogen for 20 min before 6-bromoquinoline (8, 1055 g, 5.07 mol, 1.0 equiv), allyl alcohol (588 g, 10.1 mol, 2.0 equiv), and 7V-methyl-iV-cyclohexylcyclohexylamine (1186 g, 6.08 mol, 1.2 equiv) were added at room temperature. The resulting reaction mixture was stirred at 50 – to 55 °C for 8 – 12 h. When TLC and LC/MS showed that the reaction was deemed complete, the reaction mixture was cooled to room temperature before methyl fert-butyl ether (MTBE, 10 L) was added to the reaction mixture. The resulting mixture was stirred at room temperature for 10 min before being filtered through a plug of celite. The filtrate was concentrated under the reduced pressure and the residue was purified by flash column chromatography (SiO2, 20 – 80 % ethyl acetate in heptane gradient elution) to afford 3-(quinolin-6-yl)propanal (9, 495 g, 939.1 g theoretical, 52.7%) as a yellow oil, which solidified partially upon standing at 0 – 5 0C. For 9: 1H NMR (400 MHz, DMSO-J6) δ ppm 9.75 (t, IH, J= 1.24 Hz), 8.83 (dd, IH, J= 4.15 Hz, 1.66 Hz), 8.25 (dd, IH, J= 8.3, 1.03 Hz), 7.93 (d, IH, J= 8.71 Hz), 7.76 (d, IH, J= 1.45 Hz), 7.64 (dd, IH, J= 8.72 Hz, 2.08 Hz), 7.48 (dd, IH, J= 8.30 Hz, 4.36 Hz), 3.05 (t, 2H, J= 7.26 Hz), 2.89 (t, 2H, J= 7.26 Hz); Ci2HnNO (MW 185.22), LCMS (EI) We 186 (M+ + H).
Method 2. A solution of 6-(3,3-diethoxypropyl)quinoline (23, Method A of Example 16, 520 g , 2.08 mol, 1.0 equiv) in ethyl acetate (EtOAc, 2.2 L) was cooled to 0 0C before a 2 N aqueous hydrochloric acid (HCl) solution (2.2 L) was added over 1 h while keeping the reaction temperature below 5 0C. The resulting reaction mixture was stirred for an additional 2 h at 0 – 5 0C. When TLC and HPLC/MS indicated the reaction was complete, the reaction was quenched with an ice cold 3 N aqueous sodium hydroxide (NaOH) solution at 0 °C until the pH was between 8 to 9. The layers were separated and the aqueous layer was extracted with ethyl acetate (EtOAc, 2 L). The combined organic layers were washed with brine (2 L), dried with sodium sulfate (Na2SO4), and concentrated under the reduced pressure to afford crude 3-(quinolin-6-yl)propanal (9, 385.3 g, 385.3 g theoretical, 100%) as a yellow oil, which was found to be identical to the material obtained from Method 1 in every comparable aspect. Since this crude material was found to be sufficiently pure, it was used directly in subsequent reaction without further purification.
Method 5. A 22 L flask charged with 0.5 M solution of 9-borabicyclo[3.3.1] nonane in tetrahydrofuran (9-BBN, 5.75 L, 2.89 mol, 2.0 equiv) and tetrahydrofuran (THF, 6 L) was treated with 3,3-diethoxy-l-propene (393 g, 3.02 mol, 2.10 equiv) at 0 – 5 0C and the resulting reaction mixture was subsequently warmed to room temperature and stirred at room temperature for 14 h. 6-Bromoquinoline (8, 300 g, 1.44 mol, 1.0 equiv), palladium acetate (Pd(OAc)2, 16.1 g, 0.072 mol, 0.05 equiv), potassium carbonate (K2CO3, 398 g, 2.89 mol, 2.0 equiv), tricyclohexylphosphine (22.3 g, 0.079 mol, 0.055 equiv), and water (52 g, 2.8 mol) were added to the reaction mixture at room temperature before being degassed with nitrogen for 1 h. The resulting reaction mixture was heated to 75 0C for 1 h. When TLC and LC/MS showed the reaction was deemed complete, the reaction mixture was cooled to room temperature and water (2 L) was added to dissolve the salts. The resulting mixture was then concentrated under the reduced pressure to a volume of approximately 4 L before being filtered through a plug of Celite. The Celite plug was washed with ethyl acetate (EtOAc, 2 L). The filtrate was concentrated under the reduced pressure to a volume of approximately 2 L and this residual solution was then added slowly over 5 min to a flask containing a 2.0 M aqueous hydrochloric acid (HCl) solution (2 L) at 0 – 5 °C. The resulting solution was stirred at 0 – 5 °C for 14 h before being quenched with saturated aqueous sodium bicarbonate (NaHCO3) solution at 0 0C until the pH was between 8 to 9. The layers were separated and the aqueous layer was extracted with ethyl acetate (EtOAc, 2 L). The combined organic layers were washed with brine (1 L), dried with sodium sulfate (Na2SO4), and concentrated under the reduced pressure. The residue, which contains the crude 3-(quinolin-6-yl)propanal (9) was purified by flash column chromatography (SiO2, 20 – 80 % ethyl acetate in heptane gradient elution) to afford 3-(quinolin-6-yl)propanal (9, 139 g, 266.7 g theoretical, 52.1%) as a yellow oil, which was found to be identical to the material obtained from Methods 1 and 2.
Example 18 l-(2-Chloro-l-hydroxy-3-(quinolin-6-yI)propyl)pyrrolidine-2,5-dione (11)
Method I. A solution of 3-(quinolin-6-yl)propanal (9, 407 g, 2.2 mol, 1.0 equiv) in chloroform (CHCl3, 1700 mL) was cooled to 0 0C before proline (52 g, 0.44 mol, 0.2 equiv) and iV-chlorosuccinimide (NCS, 303 g, 2.31 mol, 1.05 equiv) were added. The resulting reaction mixture was allowed to slowly warm to room temperature (becomes homogeneous) and stirred at room temperature for overnight. The reaction was exothermal to around 40 0C when it reaches room temperature and a precipitate had formed at this point. Once TLC and LC/MS showed that the reaction was deemed complete, the reaction mixture was diluted with ethyl acetate (EtOAc, 1700 mL) and the resulting mixture was cooled to 0 0C. The solid was collected by filtration and the collected wet solid cake was placed in a flask and triturated with water (750 mL). The resulting suspension was stirred at room temperature for 30 min before the solids were collected by filtration. The collected solids were washed with water (250 mL) and methyl tert-bntyl ether (MTBE, 500 mL) and dried in a vacuum oven at 45 0C to constant weight to afford l-(2-chloro-l-hydroxy-3-(quinolin-6-yl)propyl)pyrrolidine-2,5-dione (11, 378.7 g, 701.3 g theoretical, 54 % yield) as off-white powder. For 11: 1HNMR (DMSO-J6, 400MHz) δ ppm 8.86 (dd, IH, J= 4.15 Hz, 1.66 Hz), 8.33 (dd, IH, J= 8.51 Hz, 1.04 Hz), 7.98 (d, IH, J= 8.72 Hz), 7.85 (d, IH, J= 1.66 Hz), 7.68 (dd, IH, J= 8.51 Hz, 1.87 Hz), 7.51 (dd, IH, J= 8.29 Hz, 4.15 Hz), 7.36 (d, IH, J = 7.05 Hz), 5.28 (dd, IH, J= 9.54 Hz, 6.85 Hz), 5.07 (dt, IH, J= 9.75 Hz, 2.70 Hz), 3.65 (dd, IH, J= 14.52 Hz, 2.49 Hz), 3.09 (dd, IH, J= 14.52 Hz, 9.75 Hz), 2.64 (s, 4H); C16H15ClN2O3 (MW 318.75), LCMS (EI) m/e 319.2 (M+ + H).
Method II. A solution of 3-quinolin-6-ylpropanal (9, 74.8 g, 0.404 mol) in acetonitrile (202 mL, 3.87 mol) was cooled to 0 0C before L-proline (4.70 g, 0.0404 mol, 0.10 equiv), benzoic acid (4.96 g, 0.0404 mol, 0.10 equiv), and iV-chlorosuccinimide (NCS, 57.8 g, 0.424 mol, 1.05 equiv) were added at 0 0C. The reaction mixture was stirred at 0 °C for 3 h and the resulting clear solution was allowed to warm to room temperature and stirred at room temperature for 18 h. The reaction mixture became a thick suspension and LCMS showed the completion of the reaction. Ethyl acetate (EtOAc, 202 mL) was added to the reaction mixture and the resulting mixture was stirred at room temperature for 1 h. The solids were collected by filtration, washed with ethyl acetate (EtOAc, 100 mL) and dried under vacuum at 40 – 45 0C to constant weight to afford l-(2-chloro-l-hydroxy-3-(quinolin-6-yl)propyl)pyrrolidine-2,5-dione (11, 88.8 g, 128.8 g theoretical, 69 % yield) as an off-white powder, which was found to be identical to the material made from method I in every comparable aspect.
Scheme 3 (Examples 19-21)
15 21, dihydrochloride
C23H17FN6O C23H19Q2FN6O MoI Wt 412 42 MoI Wt 485 34
Example 19
2-Fluoro-4-(7-(quinolin-6-ylmethyl)imidazo[l,2-Z>] [l,2,4]triazin-2-yl)benzoic acid (14)
A suspension of 2-fluoro-4-(7-(quinolin-6-ylmethyl)imidazo[l ,2-&][l ,2,4]triazin-2-yl)benzonitrile (13, 277.5 g, 0.73 mol, 1.0 equiv) in concentrated hydrochloric acid (2500 mL) and water (250 mL) was heated to 1000C (homogenous at this point) and stirred at around 100 0C for 18 h. When LC/MS indicated the reaction was deemed complete, the reaction mixture was cooled down to 70 – 80 0C before being diluted with water (2500 mL). The resulting diluted reaction mixture was then cooled down to room temperature (yellow solid forms at 40 – 50 0C) and subsequent to 0 – 5 0C. The solids were then collected by filtration, washed with a small amount of IN aqueous HCl (100 mL), and dried in a vacuum oven at 45 0C to constant weight to afford 2-fluoro-4-(7-(quinolin-6-ylmethyl)imidazo[l,2-έ][l,2,4]triazin-2-yl)benzoic acid (14, 271 g, 291.5 g theoretical, 93% yield) as yellow to bright-yellow powders. For 14: 1H NMR (400 MHz, OMSO-d6) δ ppm 9.34 (s, IH), 9.23 (dd, IH, J- 5.19 Hz, 1.45 Hz), 9.08 (d, IH, J= 8.29 Hz), 8.38 (d, IH, J= 8.92 Hz), 8.30 (d, IH, J= 1.24 Hz), 8.18 (dd, IH, J= 8.72 Hz, 1.87 Hz), 8.12 (s, IH), 8.08 – 8.00 (m, 4H), 4.75 (s, 2H); C22H16Cl2FN5O2 (MW 472.30), C22H14FN5O2 (free base: MW 399.38), LCMS (EI) mle 400.0 (M+ + H).
Example 20 2-Fluoro-7V-methyl-4-(7-(quiiiolin-6-ylmethyl)imidazo[l,2-^][l,2,4]triazin-2-yl)benzainide
(15).
A suspension of 2-fluoro-4-(7-(quinolin-6-ylmethyl)imidazo[l ,2-b][l ,2,4]triazin-2-yl)benzoic acid (14, 431.4 g, 0.914 mol, 1.0 equiv) and (benzotriazol-1-yloxy)tripyrrolidinophosphonium hexafluorophosphate (PyBOP, 570 g, 1.1 mol, 1.2 equiv) in ΛyV-dimethylformamide (DMF, 3700 mL) was treated with a solution of 2 M methylamine in THF (1830 mL, 3.656 mol, 4.0 equiv) over 15 min at room temperature. The reaction temperature increased to 30 0C during the addition of methylamine and the reaction mixture became homogeneous once the addition of methylamine was complete. Triethylamine (TEA, 382 mL, 2.742 mol, 3.0 equiv) was then added to the reaction mixture and the resulting reaction mixture was stirred at room temperature for 2 – 4 h. When LC/MS showed the coupling reaction was deemed complete, the reaction mixture was treated with water (950 mL). The resulting suspension was cooled down to 0 – 5 0C in an ice-bath and stirred at 0 – 5 0C for 30 min. The solids were collected by filtration and washed with water (200 mL). The wet solid cake was then suspended in a mixture of water and acetonitrile (1/1 by volume, 2000 mL) and the resulted suspension was stirred at room temperature for Ih. The solids were collected by filtration, washed with water and acetonitrile, and dried in a vacuum oven at 40 – 45 0C to constant weight to afford 2-fluoro-Λ/-methyl-4-(7-(quinolin-6-ylmethyl)imidazo[l ,2-έ>][l ,2,4]triazin-2-yl)benzamide (15, 322 g, 377 g theoretical, 85.4% yield) as yellow to bright-yellow powders. For 15: 1H NMR (400 MHz, DMSO-J6) δ ppm 9.20 (s, IH), 8.82 (dd, IH, J= 4.05, 1.56 Hz), 8.38 (br m, IH), 8.27 (dd, IH, J= 8.50 Hz, 1.25 Hz), 8.06 – 7.93 (m, 5H), 7.81 – 7.74 (m, 2H), 7.49 (dd, IH, J= 8.40 Hz, 4.35 Hz), 4.62 (s, 2H), 2.78 (d, 3H, J= 4.36 Hz); C23H17FN6O (MW 412.42), LCMS (EI) mle 413.1 (M+ + H).
Example 21
2-Fluoro-Λr-methyl-4-(7-(quinoIin-6-ylmethyl)imidazo[l,2-6][l,2,4]triazm-2-yl)benzamide dihydrochloride (21, dihydrochloride)
A suspension of 2-fluoro-iV-methyl-4-[7-(quinolin-6-ylmethyl)imidazolo[l ,2-6][l,2,4]triazin-2-yl]benzamide (15, 421.2 g, 1.021 mol) in methanol (MeOH, 6600 mL) was heated to 55 0C before a premixed solution of aqueous concentrated hydrochloric acid (cone.
HCl, 37 wt.%, 12 M, 420 mL, 5.10 mol, 5.0 equiv) in isopropyl alcohol (IPA, 1510 mL) was added dropwise at 55 0C. The resulting clear solution was stirred at 55 0C for 30 min before methyl tert-butyl ether (MTBE, 6750 mL) was added via an additional runnel over 30 min. The solids were slowly precipitated out after addition of methyl tert-butyl ether. The resulting mixture was stirred at 55 0C for an additional 1 h before being gradually cooled down to room temperature. The mixture was stirred at room temperature for overnight. The solids were collected by filtration, washed with methyl tert-butyl ether (MTBE, 3 x 500 mL), and dried in vacuum oven at 45 – 55 0C to constant weight. The desired 2-fluoro-Λr-methyl-4-[7-(quinolin-6-ylmethyl)imidazolo[l,2-£][l,2,4]triazin-2-yl]benzamide dihydrochloride (21, dihydrochloride, 470.7 g, 495.5 g theoretical, 95% yield) was obtained as off-white to light yellow crystalline solids. For 21 (dihydrochloride): mp (decom.) 222 0C; 1H NMR (400 MHz, DMSO-J6) δ ppm 9.46 (s, IH), 9.25 (dd, IH, J= 5.4 Hz, 1.4 Hz), 9.12 (d, IH, J= 8.3 Hz), 8.51 (m, IH), 8.47 (d, IH, J= 0.9 Hz), 8.34 (d, IH, J= 1.3 Hz), 8.23 (s, IH), 8.21 (dd, IH, J= 9.0 Hz, 1.8 Hz), 8.09-8.02 (m, 3H), 7.79 (dd, IH, J= 7.5 Hz, 8.3 Hz), 4.77 (s, 2H), 2.78 (s, 3H, J= 4.5 Hz); 13C NMR (100 MHz, DMSO-^6) δ ppm 163.4, 159.4 (d, J= 249.9 Hz), 145.8, 145.4, 144.5, 143.8, 140.4, 138.8, 136.8, 135.9, 135.7 (J= 8.6 Hz), 131.2 ( J= 3.1 Hz), 130.7, 128.7, 128.2, 126.2 (J- 14.9 Hz), 126.0, 123.1 (J= 3 Hz), 122.5, 121.0, 114.9 (J= 5.6 Hz), 28.4, 26.3; 19F NMR (376.3 MHz, DMSO-^6) δ ppm -113.2; C23H17FN6O (free base, MW 412.42), LCMS (EI) mle 413.1 (M+ + H) and 435.0 (M+ + Na).
Scheme 4 (Examples 22-25)

C7H3BrFN C13H15BFN2O2 MoI. Wt: 200.01 MoI. Wt: 247.07 Example 22 l,2,4-Triazin-3-amine (16)
An aqueous solution of glyoxal (57 Kg of 40 wt% aqueous solution, 393 mol, 0.73 equiv) was added to a suspension of aminoguanidine bicarbonate (73 Kg, 536.3 mol) in water (400 L) at room temperature. The evolution of carbon dioxide (CO2) began almost immediately. The reaction mixture was then stirred at room temperature for 18 h and the evolution of gas had virtually ceased after about 2 h. The reaction mixture was then filtered, and the filtrate was evaporated to dryness under the reduced pressure. The residue was then extracted with cold methanol (MeOH, 3 x 120 L), and the combined methanol solution was cooled down to 0 – 5 0C before being filtered to remove the residual solids. The filtrate was then concentrated under the reduced pressure, and the residue was recrystallized in acetonitrile to afford l,2,4-triazin-3-amine (16, 34 Kg, 37.76 Kg theoretical, 90% yield) as fine, white needles. For 16: 1H NMR (400 MHz, DMSO-J6) δ ppm 8.54 (d, IH, J- 2.33 Hz), 8.20 (d, IH, J= 2.33 Hz), 7.15 (br s, 2H).
Example 23 6-Bromo-l,2,4-triazin-3-amine (17)
A solution of 1 ,2,4-triazin-3-amine (16, 33 Kg, 343.4 mol) in water (500 L) and acetonitrile (300 L) was treated with jV-bromosuccinimide (NBS, 66 Kg, 370 mol, 1.08 equiv) at 5 – 15 0C, and the resulting reaction mixture was stirred at 10 – 15 0C for 1 – 4 h. When TLC and LC/MS showed that the bromination reaction was deemed complete, the reaction mixture was treated with an aqueous solution of saturated sodium carbonate (Na2CO3). The resulting solution was then extracted with ethyl acetate (EtOAc, 3 x 500 L). The combined organic extracts were washed with water (2 x 100 L), dried over magnesium sulfate (MgSO4), and concentrated under the reduced pressure to afford 6-bromo-l,2,4-triazin-3-amine (17, 10.3 Kg, 60 Kg theoretical, 17.2% yield) as yellow to brown powders. For 17: 1H NMR (400 MHz, DMSO-J6) δ ppm 8.39 (s, IH), 7.47 (br, 2H); C3H3BrN4 (MW 174.99), LCMS (EI) mle 175.0/176.9 (M+ + H).
Example 24 2-Fluoro-4-(4,4,5,5-tetramethyl-l,3,2-dioxaborolan-2-yl)benzonitrile (19) Step 1. A solution of 2-fluro-4-bromobenzonitrile (18, 12.5 Kg, 62.5 mol) in anhydrous tetrahydrofuran (THF, 30 L) was treated with a solution of isopropylmagnesium chloride generated from magnesium (Mg, 1.8 Kg, 150 mol, 1,2 equiv) an 2-chloropropane (7.2 Kg, 92 mol, 1.47 equiv) in THF (20 L) and 2-(2-(dimethylamino)ethoxy)-τV/vr-dimethylethanamine (11 Kg, 69 mol, 1.1 equiv) at room temperature. The resulting mixture was then stirred at 12 – 20 0C for an additional 2 h before being treated with trimethylborate (9 Kg, 86.7 mol, 1.4 equiv) at 10 -15 0C. The reaction mixture was stirred at 7 – 16 0C for 40 min. When TLC and LC/MS showed that the reaction was deemed complete, the reaction mixture was quenched with 1 N aqueous hydrochloric acid (HCl, 35 Kg) at room temperature. The quenched aqueous reaction mixture was then extracted with ethyl acetate (EtOAc, 4 x 35 L). The combined organic extracts were washed with water (50 L), dried over magnesium sulfate (MgSO4), and concentrated under the reduced pressure. The residual solids were then recrystallized from acetonitrile (20 L) and hexanes (45 L) to afford the corresponding crude 3-fluoro-4-cyanophenyl boronic acid (5.0 Kg, 48% yield).
Step 2. A suspension of the crude 3-fluoro-4-cyanophenyl boronic acid (9.2 Kg, 55.8 mol) in cyclohexane (150 L) was treated with pinacol (13.2 Kg, 111.6 mol, 2.0 equiv) at room temperature, and the resulting reaction mixture was warmed to 40 0C for 4 h. When TLC and LC/MS showed that the reaction was deemed complete, the reaction mixture was cooled down to room temperature before being washed with water (2 x 75 L). The organic layer was then dried over magnesium sulfate (MgSO4) and concentrated under the reduced pressure to afford 2-fluoro-4-(4,4,5,5-tetramethyl-l,3,2-dioxaborolan-2-yl)benzonitrile (19, 11.8 Kg, 13.8 Kg theoretical, 85.6% yield) as a light yellow solid. For 19: 1H NMR (300 MHz, DMSO-J6) δ ppm 7.92 (t, IH, J- 7.00 Hz), 7.62 (m, 2H), 1.29 (s, 12 H).
Example 25 4-(3-Amino-l,2,4-triazin-6-yI)-2-fluorobenzonitrile (20).
A mixture of 6-bromo- 1,2, 4-triazin-3 -amine (17, 100.0 g, 571.47 mmol) and 2-fluoro-4-(4,4,5,5-tetramethyl-l,3,2-dioxaborolan-2-yl)benzonitrile (19, 145.43 g, 588.61 mmol, 1.03 equiv) in 1,4-dioxane (1200 mL) was stirred at room temperature for 10 min before potassium carbonate (K2CO3, 355.4 g, 2572 mmol) in water (600 mL) was added to give a deep red solution. The mixture was degassed by bubbling with nitrogen for 10 min before 1,1′-bis(diphenyl phosphino)ferrocene dichloropalladium(II) complex with dichloromethane (1 :1) (Pd(dppf)2Cl2, 14.14 g, 17.14 mmol, 0.03 equiv) was added at room temperature. The resulting reaction mixture was degassed by bubbling with nitrogen for 10 min and then heated at 86 0C under nitrogen. After 2 h, HPLC showed that the reaction was deemed complete, and the reaction mixture was cooled to room temperature and then to 0 – 5 0C with an ice-water bath. 1 ,4-Dioxane (400 mL) was added to the cooled reaction mixture before a solution of 3.3 M aqueous hydrochloric acid solution (HCl, 1900 mL) was added dropwise with stirring to adjust pH to 0.40- 0.93. The mixture was stirred at room temperature for 30 min and filtered. The solid collected was stirred with 1,4-dioxane (260 mL) and then added IN HCl (400 mL). The mixture was stirred at room temperature for 10 min and filtered. The filtrate was combined with the filtrate obtained earlier and washed with ethyl acetate (EtOAc, 2 x 2 L). The combined ethyl acetate extracts was extracted with 1 N aqueous hydrochloric acid solution (HCl, 3 x 200 mL). The combined aqueous solution was then treated with activated charcoal (20 g) and stirred at room temperature for 30 min. The mixture was filtered through a celite bed and the filtrate was cooled to 0 – 5 0C with an ice- water bath. A solution of 50% of sodium hydroxide in water (NaOH, 240 mL, 4500 mmol) was added drowise at 5-12 0C to adjust pH tolθ.6 – 11.6. The mixture was stirred at 0 – 5 0C for 30 min and then filtered. The solids collected were washed with aqueous ammonium hydroxide (1 to 3 of 28% concentrated NH4OH to water, 1900 mL) and dried under vacuum at 40 – 45 0C to constant weight to afford 4-(3-amino-l,2,4-triazin-6-yl)-2-fluorobenzonitrile (20, 101.2 g, 122.9 g theoretical, 82.3% yield) as a off-white powder. For 20: 1H NMR (400 MHz, DMSO-J6) δ ppm 8.94 (s, IH), 8.12 (d, IH, J= 11.41 Hz), 8.08 – 8.00 (m, 2 H), 7.71 (br s, 2 H); Ci0H6FN5 (MW 215.19), LCMS (EI) mle 215.9 (M+ + H).
Scheme 5 (Example 26)

20 13
C10H6FN5 C16H15ON2O3 C22H13FN6 MoI. Wt: 215.19 MoI. Wt 318.75 MoI. Wt: 380.38 Example 26 2-Fluoro-4-(7-(quinolin-6-ylmethyl)imidazo[l,2-Z>][l,2,4]triazin-2-yl)benzonitrile (13).
Step 1. A 22 L reactor equipped with a overhead stirring, a thermocouple, a distillation apparatus, and a nitrogen inlet was purged with nitrogen before 4-(3-amino-l,2,4-triazin-6-yl)-2-fluorobenzonitrile (20, 300 g, 1.39 mol), l-(2-chloro-l-hydroxy-3-(quinolin-6-yl)propyl)pyrrolidine-2,5-dione (11, 635 g, 1.99 mol, 1.43 equiv), and ethylene glycol (3.0 L) were charged to the reactor at room temperature. The resulting reaction mixture was heated to 130-140 °C with nitrogen bubbled through continuously. The distillate was collected with the distillation apparatus. After 3 – 4 h, HPLC indicated the reaction was deemed complete (presence of < 1.5% of starting material 20). The reaction mixture was gradually cooled to room temperature. A 2.5% aqueous sodium carbonate solution (Na2CO3, 14.1 L) was added with stirring to the reactor over 60 min and the mixture was stirred at room temperature for 1 – 2 h. The mixture was then filtered, and the solid was washed with water (9.6 L) and dried under vacuum to afford the desired crude product (13, 980.4 g), which was combined with several other batches for purification as described below.
Step 2. A solution of crude product (13, 2754 g) in methylene chloride (CH2Cl2, 37.8 L) and methanol (0.54 L) was treated with silica gel (SiO2, 2700 g) at room temperature, and the resulting mixture was stirred at room temperature for 90 min. The mixture was filtered and the filter cake was washed with a mixture OfCH2Cl2(18 L) and methanol (0.26 L). The combined filtrates were treated with silica gel (SiO2J 800 g) and the resulting mixture was stirred at room temperature for 90 min and then filtered. The filter cake was washed with a mixture of CH2Cl2 (18 L) and methanol (0.26 L). The combined filtrates were concentrated under the reduced pressure at 20 – 60 0C to about 8 – 12 L. The residue was treated with a mixture of isopropanol (IPA) and water (1 : 1 , 9 L) in portions and the distillation was continued at 1 atm pressure until the temperature reached 68 – 75 0C. The mixture was cooled to room temperature and the solids were collected by filtration. The solids collected were washed with isopropanol (IPA, 3.6 L) and dried under vacuum at 40 – 45 0C to constant weight to afford pure 2-fluoro-4-(7-(quinolin-6-ylmethyl)imidazo[l,2-ό][l,2,4]triazin-2-yl)benzonitrile (13, 940.27g) as a bright yellow powder.
The above reaction and purification process gave product 13 in 59 – 64% yield. The spectroscopic data of compound 13 made by this synthetic process was found to be identical to those obtained from material made by cyanation of compound 12 described previously. For 13: 1H NMR (400 MHz, OMSO-d6) δ ppm 9.24 (s, IH), 8.81 (dd, IH5 J= 4.15, 1.66 Hz), 8.26 – 8.12 (m, 4H), 8.02 (s, IH), 7.95 – 7.93 (m, 2H), 7.76 (dd, IH, J= 8.71, 2.08 Hz), 7.47 (dd, IH, J = 8.70, 4.15 Hz), 4.62 (s, 2H); C22Hi3FN6 (MW 380.38), LCMS (EI) m/e 381.0 (M+ + H).
Scheme 6 (Examples 27-29)

14 15
C22H14FN5O2 C23H17FN6O MoI. Wt: 399.38 MoI. Wt: 412.42
I I) SOd2 aq. HCl/ acetone { 2) MeNH2

15 (.{hydrochloride
C23H17FN6O C23H19CI2FN6O MoI. Wt: 412.42 MoI. Wt: 485.34
Example 27
2-Fluoro-4-(7-(quinolin-6-ylmethyl)imidazo [1,2-6] [1,2,4] triazin-2-yl)benzoic acid (14).
To a 22 L reactor equipped with a overhead stirring, a thermocouple, and a nitrogen inlet was charged compound 13 (900 g, 2.37 mol), water (0.9 L), and concentrated HCl (9.1 L) at room temperature. The resulting reaction mixture was heated at 100 0C for 12 h. When HPLC showed the reaction was complete, the reaction mixture was cooled to 90 0C and water (4.9 L) was added over 15 min while maintaining the temperature at 65 – 90 0C. The reaction mixture was further cooled to room temperature and stirred at room temperature for 3 h. The solids were collected by filtration, washed with water (1.2 L) and dried in vacuum at 40 – 45 0C to constant weight to afford 2-fluoro-4-(7-(quinolin-6-ylmethyl)imidazo[l,2-6][l,2,4]triazin-2-yl)benzoic acid (14, 945 g, 946.5 g theoretical, 99.8% yield) as a light yellow solid, which was found to be identical to the material made by earlier method. For 14: 1H NMR (400 MHz, DMSO-J6) δ ppm 9.34 (s, IH), 9.23 (dd, IH, J= 5.19 Hz, 1.45 Hz), 9.08 (d, IH5 J= 8.29 Hz), 8.38 (d, IH, J = 8.92 Hz), 8.30 (d, IH, J= 1.24 Hz), 8.18 (dd, IH, J= 8.72 Hz, 1.87 Hz), 8.12 (s, IH), 8.08-8.00 (m, 4H), 4.75 (s, 2H); C22Hi6Cl2FN5O2 (MW 472.30), C22H14FN5O2 (free base: MW 399.38), LCMS (EI) mle 400.0 (M+ + H).
Example 28
2-Fluoro-iV-methyl-4-(7-(quinolin-6-yImethyl)iinidazo [ 1 ,2-6] [ 1 ,2,4] triazin-2-yl)benzamide
(15).
Method A. To a stirred solution of 2-fluoro-4-(7-(quinolin-6-ylmethyl)imidazo[l,2-6][l,2,4]triazin-2-yl)benzoic acid (14, 1000 g, 2.12 mol) in acetonitrile (5 L) and CH2Cl2(10 L) were charged HOBt (358 g, 2.65 mol, 1.25 equiv), and EDC hydrochloride (508.4 g, 2.65 mol, 1.25 equiv) at room temperature. Another portion OfCH2Cl2 (10 L) was then added to the reaction mixture and the resulting reaction mixture was stirred at room temperature for 20 min. A 2.0 M solution of methylamine (MeNH2) in THF (3.44 L, 6.88 mol, 3.25 equiv) was added with stirring while maintaining the temperature at 15 – 30 0C. The reaction mixture was stirred at room temperature for 2 h before an additional portion of 2.0 M solution of methylamine (MeNH2) in THF (1.06 L, 2.12 mol, 1 equiv) was added. The reaction mixture was stirred at room temperature for 1 h and a second portion of EDC hydrochloride (406 g, 2.12 mol, 1 equiv) was added and the stirring was continued for 6 h. When HPLC showed less than 1 % of starting material (14) was remaining, the reaction mixture was concentrated under the reduced pressure at < 50 0C. During distillation acetonitile (20 L) was added and distillation was continued until the remaining volume was about 20 L. The residue was treated with an aqueous solution of 2.5% sodium carbonate (Na2CO3, 40 L) and the resulting mixture was stirred at room temperature for 30 min. The solids were collected by filtration, washed with water (3 x 4.0 L), air dried by pulling vacuum on the filter to afford the crude desired product (15). The crude solids were treated with CH2Cl2 (17.6 L) and MeOH (5.2 L) at room temperature and resulting mixture was stirred until a clear solution was obtained. The solution was filtered to remove insoluble materials. With vigorous stirring a 2.5% aqueous solution of sodium carbonate (Na2CO3, 17.6 L) was added to the filtrate and the mixture was stirred at room temperature for 60 min to give a suspension. Heptane (20 L) was added and the mixture was stirred for an additional 60 min. The mixture was filtered and the solid was washed sequentially with water (3 x 4.0 L) and heptane (4.0 L), and dried in vacuum to afford 2-fluoro-./V-methyl-4-(7-(quinolin-6-ylmethyl)imidazo[l,2-b][l,2,4]triazin-2-yl)benzamide (15, 1095.3 g, 874.3 g theoretical) as a bright yellow solid, which was found to be not totally dry and to contain ~ 25% residual solvents. This wet solid was used directly for the subsequent dihydrochloride salt (21) formation reaction without further drying. A small sample was dried completely for spectroscopic analyses and the data were consistent with those obtained by earlier method: For 15: 1H NMR (400 MHz, DMSO-J6) δ ppm 9.20 (s, IH), 8.82 (dd, IH, J= 4.05, 1.56 Hz), 8.38 (br m, IH), 8.27 (dd, IH, J = 8.50 Hz, 1.25 Hz), 8.06 – 7.93 (m, 5H), 7.81 – 7.74 (m, 2H), 7.49 (dd, IH, J= 8.40 Hz, 4.35 Hz), 4.62 (s, 2H), 2.78 (d, 3H, J= 4.36 Hz); C23HnFN6O (MW 412.42), LCMS (EI) m/e 413.1 (M+ + H).
Method B. 2-Fluoro-4-[7-(quinolin-6-ylmethyl)imidazo[l,2-b][l,2,4]triazin-2-yl]benzoic acid dihydrochloride (14, 50.00 g, 0.1059 mol) was added toluene (300 mL) and followed by thionyl chloride (SOCl2, 77.2 mL, 1.06 mol, 10.0 equiv) at room temperature. The resulting reaction mixture was heated at 72 0C under N2 and the reaction was followed by HPLC analysis of the disappearance of the starting material benzoic acid (14). After 48 h, HPLC indicated ~4% starting material remaining and the reaction was stopped. The reaction mixture was concentrated to dryness by vacuum distillation at 40-50 0C. The residual solids were added toluene (300 mL) and the solvent was removed by vacuum distillation at 40-50 0C. THF (250 mL) was added and the mixture was cooled with an ice-water bath. A 2.0 M of methylamine (MeNH2) in THF (529 mL, 1.06 mol, 10 equiv) was added dropwise. The resulting reaction mixture was allowed to warm up to room temperature and stirred at room temperature for 17 h. Water (600 mL) was added to the reaction mixture and THF (400 – 500 mL) was removed by vacuum distillation at 40 0C. Sodium carbonate (15.60 g, 0.147 mol) was added and the mixture was stirred at room temperature for 30 min. The mixture was filtered and the solid was washed with water (3 x 30 mL) and dried. The solid was dissolved in pre-mixed methylene chloride (CH2Cl2, 1000 mL) and methanol (MeOH, 300 mL). With vigorous stirring, a solution of 0.236 M of sodium carbonate (Na2CO3) in water (1000 mL) was added dropwise. Solid was slowly precipitated out after addition of aqueous solution of sodium carbonate (Na2CO3). Hexane (1000 niL) was then added dropwise with stirring. The mixture was stirred at room temperature for 30 – 40 min and the solids were collected by filtration. The solids collected were washed with water (3 x 200 mL) and dried in vacuum at 40 – 500C to constant weight to afford 2-fluoro-Λr-methyl-4-(7-(quinolin-6-ylmethyl)imidazo[l,2-ό][l,2,4]triazin-2-yl)benzamide (15, 42.2 g, 43.67 g theoretical, 96.6% yield) as a bright yellow solid, which was found to be identical to the material made by Method A in every comparable aspect. For 15: 1H NMR (400 MHz, DMSO-J6) δ ppm 9.20 (s, IH), 8.82 (dd, IH, J= 4.05, 1.56 Hz), 8.38 (br m, IH), 8.27 (dd, IH, J= 8.50 Hz, 1.25 Hz), 8.06 – 7.93 (m, 5H), 7.81-7.74 (m, 2H), 7.49 (dd, IH, J= 8.40 Hz, 4.35 Hz), 4.62 (s, 2H), 2.78 (d, 3H, J= 4.36 Hz); C23H17FN6O (MW 412.42), LCMS (EI) mle 413.1 (M+ + H).
Example 29
2-Fluoro-iV-methyl-4-(7-(quinolin-6-ylmethyl)imidazo [ 1 ,2-b] [ 1 ,2,4] triazin-2-yl)benzamide dihydrochloride (21, dihydrochloride)
2-Fluoro-vV-methyl-4-(7-(quinolin-6-ylmethyl)imidazo[l, 2-Z?][l, 2,4]triazin-2-yl)benzamide (15, 210O g, containing ~25% residual solvents) and filtered USP water (7.6 L) were charged into a 50 L reactor at room temperature. With stirring a solution of 6 M aqueous hydrochloric acid (HCl, 3 L) was added with an additional funnel. The resulting reaction mixture was stirred at room temperature for 1.5 h. Acetone (30.5 L) was added to the reactor with stirring during 1 h and the resulting mixture was stirred at room temperature for 2.5 h. The solids were collected by filtration, washed with acetone (2 x 4.3 L) and dried in vacuum to constant weight to afford 2-fluoro-iV-methyl-4-(7-(quinolin-6-ylmethyl)imidazo[l ,2-b][ 1 ,2,4]triazin-2-yl)benzamide dihydrochloride (21, dihydrochloride, 1629.2 g, 1830.6 g theoretical, 89%) as a pale yellowish crystalline powder, which was found to be identical to the material made by previous method in every comparable aspect. For 21 (dihydrochloride): 1H NMR (400 MHz, DMSO-J6) δ ppm 9.46 (s, IH), 9.25 (dd, IH, J= 5.4 Hz, 1.4 Hz), 9.12 (d, IH, J= 8.3 Hz), 8.51 (m, IH), 8.47 (d, IH, J= 0.9 Hz), 8.34 (d, IH, J= 1.3 Hz), 8.23 (s, IH), 8.21 (dd, IH, J= 9.0, 1.8 Hz), 8.09 – 8.02 (m, 3H), 7.79 (dd, IH, J= 7.5, 8.3 Hz), 4.77 (s, 2H), 2.78 (s, 3H, J= 4.5 Hz); 13C NMR (100 MHz, DMSO-J6) δ ppm 163.4, 159.4 (d, J= 249.9 Hz), 145.8, 145.4, 144.5, 143.8, 140.4, 138.8, 136.8, 135.9, 135.7 (J= 8.6 Hz), 131.2 ( J= 3.1 Hz), 130.7, 128.7, 128.2, 126.2 (J= 14.9 Hz), 126.0, 123.1 (J= 3 Hz), 122.5, 121.0, 114.9 (J= 5.6 Hz), 28.4, 26.3; 19F NMR (376.3 MHz, DMSO-Z6) δ ppm -113.2; C23H17FN6O (free base, MW 412.42), LCMS (EI) mle 413.1 (M+ + H) and 435.0 (M+ + Na).\
PATENT
(S)-N-(54(R)-2-(2,5-difluoropheny1)-pyrrolidin-1-y1)-pyrazolo[1,5-a]pyrimidin-3-y1)-3-hydroxypyrrolidine-1-carboxamide.
/////////////////Capmatinib, INC 280, INC-280, капматиниб , كابماتينيب , 卡马替尼 , INCB 28060
CNC(=O)C1=CC=C(C=C1F)C1=NN2C(CC3=CC=C4N=CC=CC4=C3)=CN=C2N=C1
DR ANTHONY MELVIN CRASTO

ORGANIC SPECTROSCOPY
Read all about Organic Spectroscopy on
ORGANIC SPECTROSCOPY INTERNATIONAL

