
FLAGS AND HITS
 DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO
DRUG APPROVALS BY DR ANTHONY MELVIN CRASTO FACEBOOK
...................................................................Join me on twitter
FACEBOOK
...................................................................Join me on twitter
 ..................................................................Join me on google plus
..................................................................Join me on google plus
 Googleplus
GoogleplusMYSELF

Naxtarubicin, Annamycin
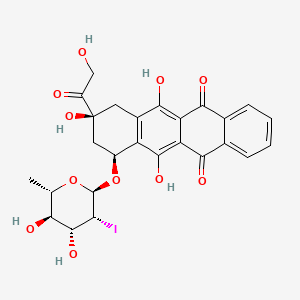
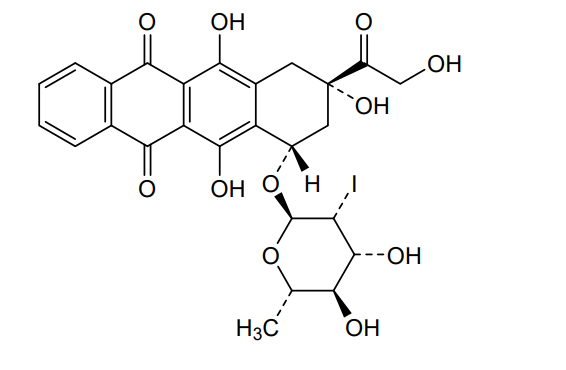
Naxtarubicin, Annamycin
CAS 92689-49-1
MF C26H25IO11 MW 640.4 g/mol
2′-Iodo-3′-hydroxy-4′-epi-4-demethoxydoxorubicin
(7S,9S)-7-[(2R,3R,4R,5R,6S)-4,5-dihydroxy-3-iodo-6-methyloxan-2-yl]oxy-6,9,11-trihydroxy-9-(2-hydroxyacetyl)-8,10-dihydro-7H-tetracene-5,12-dione
(7S,9S)-7-[(2,6-dideoxy-2-iodo-α-L-mannopyranosyl)oxy]-6,9,11-trihydroxy-9-(2-hydroxyacetyl)-7,8,9,10-
tetrahydrotetracene-5,12-dione
DNA topoisomerase II inhibitor, antineoplastic, Annamycin, Annamycin-LF, Annamycin-liposomal, L-ANNA, L-annamycin, Liposomal annamycin, S-ANNA, SNU299M83Q
- OriginatorUniversity of Texas M. D. Anderson Cancer Center
- DeveloperAronex Pharmaceuticals; Callisto Pharmaceuticals; Moleculin Biotech; University of Texas M. D. Anderson Cancer Center
- ClassAnthracyclines; Antineoplastics; Cytostatic antibiotics; Small molecules
- Mechanism of ActionType II DNA topoisomerase inhibitors
- Orphan Drug StatusYes – Soft tissue sarcoma; Precursor cell lymphoblastic leukaemia-lymphoma; Acute myeloid leukaemia
- Phase II/IIIAcute myeloid leukaemia
- Phase IIOvarian cancer
- Phase I/IISoft tissue sarcoma
- PreclinicalColorectal cancer; Liver cancer; Pancreatic cancer; Solid tumours
- DiscontinuedChronic myeloid leukaemia; Precursor cell lymphoblastic leukaemia-lymphoma; Triple negative breast cancer
- 30 Oct 2025Moleculin biotech plans future regulatory filings based on data from phase III MIRACLE trial
- 29 Oct 2025Moleculin Biotech has patent protection for Naxtarubicin in Australia
- 23 Oct 2025Moleculin Biotech plans to submit an IND application to the US FDA for Pancreatic cancer
Naxtarubicin is a lipophilic, anthracycline antineoplastic antibiotic.Naxtarubicin intercalates into DNA and inhibits topoisomerase II, thereby inhibiting DNA replication and repair as well as inhibiting RNA and protein synthesis. This agent appears to not be a substrate for the p-glycoprotein associated multidrug-resistance (MDR) transporter; therefore, overcoming the resistance pattern seen with other anthracycline compounds.
Annamycin is an anthracycline antibiotic being investigated for the treatment of cancer.
SYN
US 4537882
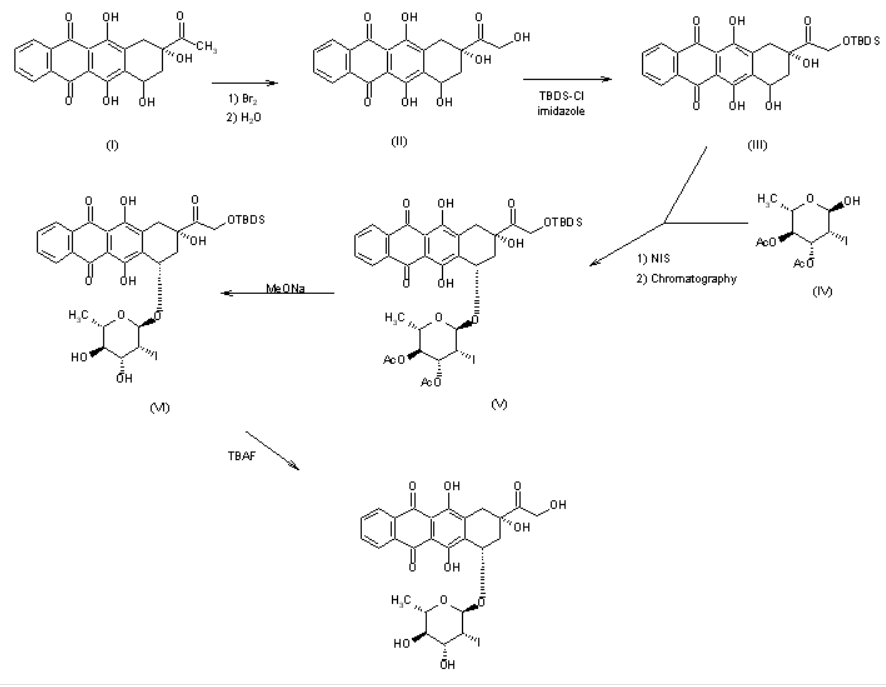
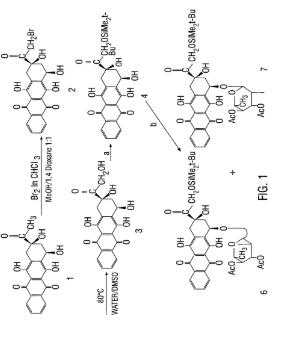
The reaction of racemic 4-demethoxydaunomycinone (I) with Br2 followed by hydrolysis in basic medium gives 4-demethoxyadriamycinone (II), which is treated with tert-butyldimethylsilyl chloride and imidazole in DMF to yield the monoprotected compound (III). The condensation of (III) with 3,4-di-O-acetyl-2,6-dideoxy-2-iodo-alpha-L-mannopyranose (IV) by means of N-iodosuccinimide (NIS), followed by chromatographic separation of the diastereomers affords (7S,9S)-14-O-(tert-butyldimethylsilyl)-4-demethoxy-7-O-(3,4-di-O-acetyl-2,6-dideoxy-2-iodo-alpha-L-mannopyranosyl)adriamycinone (V). The hydrolysis of (V) with sodium methoxide in methanol gives the silylated compound (VI), which is finally desilylated with tetrabutylammonium fluoride (TBAF) in dichloromethane/THF/pyridine.
SYN
https://patents.google.com/patent/US5977327A/en
EXAMPLE VIIIPURIFICATION OF ANNAMYCIN
Crude product was purified further by triple precipitation from THF. To accomplish this, approximately 87 mL of THF was used to redissolve each gram of Annamycin product and an equal volume of one of the following solvents was added to precipitate the Annamycin in each successive precipitation step. In the preferred method, the first precipitation was accomplished by adding an equal volume of a 7:3 mixture of hexane\diethylether, the second precipitation was accomplished by the addition of an equal volume of hexane, and the third precipitation was by addition of an equal volume of water and evaporation of half of the THF. Product obtained in this way (9.0146 g; 59%) was a complex containing 3 molecules of Annamycin per 2 molecules of THF and its purity by HPLC analysis was better than 98%. HPLC analysis was on an analytical C-18 reverse phase column with increasing concentrations of methanol/acetonitrile in water. The purity was determined by measuring the area of the absorbance peaks. 1 H NMR (DMSO-d6) d 1.20 (d, 3H, J6′, 5′ =6.2 Hz, H-6′), 1.75 (m, 2.7H, Ha from THF), 2.10 (dd, 1H, J8a,7 =5.6 Hz, J8a,8e =14.5 Hz, H-8a), 2.18 (dd, 1H, J8e,8a =14.8 Hz, J8e,7 =2.9 Hz, H-8e), 250 (DMSO peak), 2.75 (dd, 1H, J3′,2′ =3.9 Hz, J3′,4′ =8.8 Hz, H-3′), 2.95 (d, 1H, J10a,10e =18.4 Hz, H-10a), 3.00 (d, 1H, J10e,10a =18.4 Hz, H-10e), 3.20 (t, 1H, SJ=18.1 Hz, H-4′), 3.59 (m, 2.7H, Hb from THF), 3.95 (m, 1H, H-5′), 4.30 (d, 1H, J2′,3′ =4.0 Hz, H-2′), 4.55 (s, 2H, H-14), 4.89 (t, 1H, exchangeable, OH), 4.92 (m, 1H, H-7), 5.18 (d, 1H, exchangeable, OH), 5.38 (d, 1H, exchangeable, OH), 5.49 (s, 1H, H-1′), 5.50 (d, 1H, exchangeable, OH), 7.9, 8.4 (2m, 4H,H-1,2,3,4); 13 C NMR (DMSO-d6) d 17.0(s, 1C, C-6′), 24.5 (s, 1C, THFb), 31.7 (s, 1C, C-2′), 31.9 (s, 1C, C-10), 36.4 (s, 1C, C-8), 63.0 (s, 1C, C-3′), 66.4 (s, 1C, C-5′), 67.4 (s, 1C, THFa), 69.4, 13 C-NMR (DMSO-d6) δ 17.9 (s, 1C, C-6′), 25.1 (s, 1C, THFb), 40.6, 36.6, 32.1 (3s, 3C, C-2′,8,10), 63.6 (s, 1C, C-14), 67.0, 67.5, 70.4, 69.7 (4s, 4C, C-7, 5′, 3′, THFa), 74.2, 74.7 (2s, 2C, C-9, 4′), 104.5 (s, 1C, C-1′), 110.1, 110.8 (2s, 1C, C-11a, 5a), 126.6, 132.6, 132.8, 134.4, 135.1, 135.0, 136.0 (7s, 8C, C-2, 3, 1, 4, 4a, 12a, 10a), 136.0 (s, 1C, C-6a), 155.1, 156.4 (2s, 2C, C-6, 11), 186.2, 186.3 (2s, 2C, C-5, 12), 214 (s, 1C, C-13).
SYN
SYN
SYN
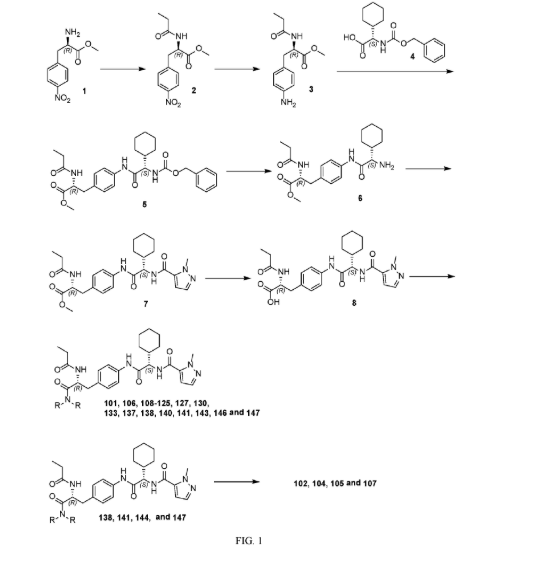
EXAMPLE I. SYNTHESIS OF (+)-4-DEMETHOXY-14-O-TERT-BUTYL
DIMETHYLSILYL-7-O-(2,6-DIDEOXY-2-IODO-α-L-MANNOPYRANOSYL)ADRIAMYCINONE (8)
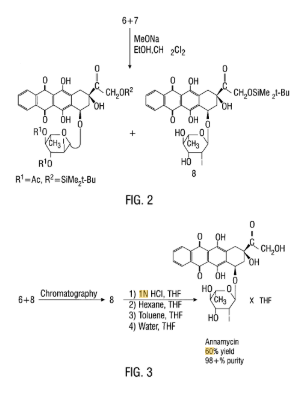
To a solution consisting of a mixture of compounds (6) and (7), shown in Figure 1 , (1.8530g, 2.21mmol) in CH2CI2 (48 mL) and EtOH (16 mL), a IN MeONa solution in MeOH (1.6 mL) was added at room temperature with stirring. Next 1.6 mL of a IN MeONa solution in MeOH (1.6 mL) was added after 50 min. After 1.5 hr. the reaction was checked by TLC developed with CCl4/MeOH (96:4), and the reaction mixture was diluted with dichloromethane (300 mL) and 0.05N HCL (100 mL) was added. The resulting mixture was shaken in a separatory funnel and, after separation, the organic layer was washed with water (2 x 50 mL), dried over Na2SO4, filtered and evaporated. The residue left after evaporation was precipitated from 4 mL of CH2CI2 by addition of 35 mL of hexane. The precipitate was filtered, washed with hexane (40 mL) and then dried in vacuo (1 lmbar) at ambient temperature for 30 min. to give crude product (8) (1.3618g, 82%). The crude product was then filtered through silica with a solution of 95:5 toluene/acetone and precipitated from CH2CI2 by addition of hexane. Product was then dried in vacuo (1 lmbar) at ambient temperature for 30 minutes to give pure compound (8) (1.358g; 55%): ^H NMR d 0.15 (s, 6H, Me2Si), 0.95 (s, 9H, CMe3), 1.40 (d, 3H, J6′,5’=6.2Hz, H-6′), 2.18 (dd, 1H, J8a,7=4.4Hz, J8a,8e=l 5.0Hz, H-8a), 2.35 (d, 1H, J8e,8a=14.9Hz, H-8e), 2.85 (dd, 1H, J3′,2’*=4-0Hz, J3′54’=8.9Hz, H-3′), 3.02 (d, 1H, Jl0a,10e=19.0Hz, H-lOa), 3.24 (d, 1H, Jl0e,10a=l 9.0Hz, H-lOe), 3.58 (t, 1H, SJ=18.2Hz, H-4′), 3.94 (m, 1H, H-5′), 4.18 (s, 1H, 9OH), 4.54 (d, 1H, J2′,3’=3.9Hz, H-2′) 4.84, 4.90 (2d, 2H, H-14), 5.22 (bs, 1H, H-7), 5.75 (s, 1H, H-l’), 7.9, 8.4 (2m, 4H, H-1,2,3,4).
EXAMPLE II. DESILYLATION IN THF/HCl
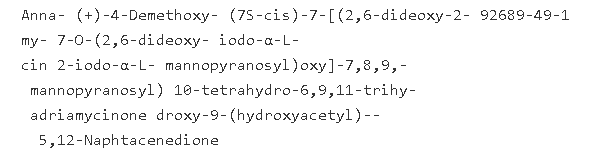
To a solution of compound (8), (16.5928g, 21.99mmol) in THF (415 mL), IN HC1 (415 mL) was added. After 25 minutes the progress of the reaction was checked by TLC developed in toluene/acetone (6:4 or 5:1) and half of the THF was evaporated in vacuo at 20°C (35mbar). The precipitate was filtered off and washed with water until the pH reached neutral (14 x 40 mL), then washed with ether (Et2θ, 5 x 32 mL) and subsequently with water (3 x 40 mL). The crude product was pre-dried on a Buchner funnel and then dried in vacuo (0.08mbar) at room temperature for 38 hrs.
EXAMPLE III. DESILYLATION IN METHANOL/HC1
To a solution/suspension of compound (8) (1.0064 g, 1.33 mmol) in methanol (45 mL), IN HC1 (10 mL) was added. The progress of the reaction was monitored by TLC developed in toluene/acetone, 6:4 and chloroform methanol, 94:6. After 45 min. 5 mL of IN HC1 solution was added to the reaction mixture. After 1 hr. 15 min. the product of the reaction was precipitated by addition of 30 mL water and filtered off. Product was washed with water until neutral pH (4 x 10 mL), diethylether (3 x 10 mL) and again with water (2 x 10 mL). Crude product was pre-dried on Buchner funnel and then dried in vacuo (0.1 mbar) at room temperature for 24 hrs. to give 0.6722 g (79% yield) of deep red powder.
EXAMPLE IV. DESILYLATION IN METHANOL/H2SO4
To a solution suspension of compound (8) (1.0065 g, 1.33 mmol) in methanol (45 mL), 10 mL of IN H2SO4 was added. The progress of the reaction was monitored by TLC developed in toluene/acetone, 6:4 and chloroform/methanol, 94:6. After 15 min. the product of the reaction was precipitated by adding 35 mL of water and filtered off. Product was washed with water until neutral pH (4 x 10 mL), diethylethe (3 x 10 mL) and again with water (2 x 10 mL). Crude product was pre-dried on Buchner funnel and then dried in vacuo (0.1 mbar) at room temperature for 24 hrs. to give 0.6318 g (74% yield) of deep red powder. EXAMPLE V. DESILYLATION IN ACETONE/H2SO4
To a solution of compound (8) (0.7592 g, 1.01 mmol) in acetone (30 mL) 3.5 mL IN H2SO4 was added. The progress of the reaction was monitored by TLC developed in toluene/acetone, 6:4 and chloroform/methanol, 94:6. After 1 hr. the product of the reaction was precipitated by addition of 35 mL water and filtered off. The product was washed with water until neutral pH (4 x 10 mL), dicthyleher (3 x 10 mL) and again with water (2 x 10 mL). Crude product was pre-dried on Buchner funnel and then dried in vacuo (0.1 mbar) at room temperature for 48 hrs. to give 0.4994 g (77% yield) of deep red powder.
EXAMPLE VI. DESILYLATION IN DMSO/HC1
To a solution of compound (8) (0.7815 g, 1.04 mmol) in DMSO (30 mL) 7.5 mL of IN HC1 was added. Progress of the reaction was monitored by TLC developed in toluene/acetone, 6:4 and chloroform/methanol, 94:6. After 1 hr. 20 min. the product of the reaction was precipitated by addition of water (37 mL) and filtered off. The product was washed with water until neutral pH (4 x 10 mL), dietheylether (3 x 10 mL) and again with water (2 x 10 mL). Crude product was pre-dried on Buchner funnel and then dried in vacuo (0.1 mbar) at room temperature for 48 hrs. to give 0.5165 g (78% yield) of deep red powder. EXAMPLE VII. DESILYLATION IN DMSO/H2SO
To a solution of compound (8) (0.7613 g, 1.01 mmol) in DMSO (5 mL) and ethanol
(10 mL) 1 mL of IN H2SO4 was added. Progress of the reaction was monitored by TLC developed in toluene/acetone, 6:4 and chloroform/methanol, 94:6. After 1 hr. 10 min. product of the reaction was precipitated by addition of water (15 mL) and filtered off. Product was washed with water until neutral pH (4 x 10 mL), diethylether (3 x 10 mL) and again with water (2 x 10 mL). Crude product was pre-dried on Buchner funnel and then dried in vacuo (0.1 mbar) at room temperature for 48 hrs. to give 0.5338 g (83% yield) of deep red powder. EXAMPLE VIII. PURIFICATION OF ANNAMYCIN
Crude product was purified further by triple precipitation from THF. To accomplish this, approximately 87 mL of THF was used to redissolve each gram of Annamycin product and an equal volume of one of the following solvents was added to precipitate the .Annamycin in each successive precipitation step. In the preferred method, the first precipitation was accomplished by adding an equal volume of a 7:3 mixture of hexane\diethylether, the second precipitation was accomplished by the addition of an equal volume of hexane, and the third precipitation was by addition of an equal volume of water and evaporation of half of the THF. Product obtained in this way (9.0146g; 59%) was a complex containing 3 molecules of .Annamycin per 2 molecules of THF and its purity by HPLC analysis was better than 98%. HPLC analysis was on an analytical C-18 reverse phase column with increasing concentrations of methanol/acetonitrile in water. The purity was determined by measuring the area of the absorbance peaks. H NMR (DMSO-d6) d 1.20 (d, 3H, J6′,5′-=6.2Hz, H-6′), 1.75 (m, 2.7H, Ha from THF), 2.10 (dd, IH, J8a,7=5.6Hz, J8a,8e=14.5Hz, H-8a), 2.18 (dd, IH, J8e,8a=14.8Hz, J8e,7=2.9Hz, H-8e), 2.50 (DMSO peak), 2.75 (dd, IH, J3′,2’=3.9Hz, J3′,4’=8.8Hz, H-3′), 2.95 (d, IH, Jl0a,10e=18.4Hz, H-10a), 3.00 (d, IH, Jl0e,10a=18.4Hz, H-lOe), 3.20 (t, IH, SJ=18.1Hz, H-4′), 3.59 (m, 2.7H, Hb from THF), 3.95 (m, IH, H-5′), 4.30 (d, IH, J2′,3’=4.0Hz, H-2′), 4.55 (s, 2H, H-14), 4.89 (t, IH, exchangeable, OH), 4.92 (m, IH, H-7), 5.18 (d, IH, exchangeable, OH), 5.38 (d, IH, exchangeable, OH), 5.49 (s, IH, H-l’), 5.50 (d, IH, exchangeable, OH), 7.9, 8.4 (2m, 4H,H- 1,2,3,4); 13C NMR (DMSO-d6) d 17.0(s, IC, C-6′), 24.5 (s, IC, THFb), 31.7 (s, IC, C-2′), 31.9 (s, IC, C-10), 36.4 (s, IC, C-8), 63.0 (s, IC, C-3′), 66.4 (s, IC, C-5′), 67.4 (s, IC, THFa), 69.4, ,3C-NMR (DMSO-d6) δ 17.9 (s, IC, C-6′), 25.1 (s, IC, THFb), 40.6, 36.6, 32.1 (3s, 3C, C-2′, 8, 10), 63.6 (s, IC, C-14), 67.0, 67.5, 70.4, 69.7 (4s, 4C, C-7, 5′, 3′, THFa), 74.2, 74.7 (2s, 2C, C-9, 4′), 104.5 (s, IC, C-l’), 110.1, 110.8 (2s, IC, C-lla, 5a), 126.6, 132.6, 132.8, 134.4, 135.1, 135.0, 136.0 (7s, 8C, C-2, 3, 1, 4, 4a, 12a, 10a), 136.0 (s, IC, C-6a), 155.1, 156.4 (2s, 2C, C-6, 11), 186.2, 186.3 (2s, 2C, C-5, 12), 214 (s, IC, C-13).
PAT
- Co-solvent compositions and methods for improved delivery of dantrolene therapeutic agentsPublication Number: US-2011160261-A2
- HER2 mutation inhibitorsPublication Number: US-12447153-B2Grant Date: 2025-10-21
- Submicron liposome suspensions obtained from preliposome lyophilizatesPublication Number: US-7238366-B1Priority Date: 1995-06-06Grant Date: 2007-07-03
- Submicron liposome suspension obtained from freeze-dried preliposomePublication Number: JP-H11507369-APriority Date: 1995-06-06
- Submicron liposome suspensions obtained from preliposome lyophilizatesPublication Number: EP-1800665-A3Priority Date: 1995-06-06
- Submicron liposome suspensions obtained from preliposome lyophilizatesPublication Number: EP-0831781-A1Priority Date: 1995-06-06
- Process for preparing aminoglycsidic antibioticsPublication Number: CS-202570-B2Priority Date: 1976-04-14
- Methods and systems for assessing biological materials using optical and spectroscopic detection techniquesPublication Number: US-2004052730-A1Priority Date: 1995-10-04
- Submicron liposome suspensions obtained from preliposome lyophilizatesPublication Number: EP-1800665-A2Priority Date: 1995-06-06
- Submicron liposome suspensions obtained from preliposome lyophilizatesPublication Number: US-5902604-APriority Date: 1995-06-06Grant Date: 1999-05-11
- Submicron liposome suspensions obtained from preliposome lyophilizatesPublication Number: WO-9639121-A1Priority Date: 1995-06-06
- Submicron liposome suspensions obtained from preliposome lyophilizatesPublication Number: CA-2221341-A1Priority Date: 1995-06-06
- Compounds and methods for the selective treatment of cancer and bacterial infectionsPublication Number: WO-9739007-A1Priority Date: 1996-04-12
- Compounds and methods for the selective treatment of cancer and bacterial infectionsPublication Number: US-6218519-B1Priority Date: 1996-04-12Grant Date: 2001-04-17
- Methods and systems for assessing biological materials using optical and spectroscopic detection techniquesPublication Number: US-6573063-B2Priority Date: 1995-10-04Grant Date: 2003-06-03
- Methods and systems for assessing biological materials using optical and spectroscopic detection techniquesPublication Number: US-6319682-B1Priority Date: 1995-10-04Grant Date: 2001-11-20
- Methods and systems for assessing biological materials using optical and spectroscopic detection techniquesPublication Number: US-2002055092-A1Priority Date: 1995-10-04



AS ON OCT2025 4.511 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT

join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE

join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com

Further reading
- Priebe W (1995). “Mechanism of action-governed design of anthracycline antibiotics: a “turn-off/turn-on” approach”. Current Pharmaceutical Design. 1 (1): 51–68. doi:10.2174/1381612801666220524190711. S2CID 90406009.
- Trevino AV, Woynarowska BA, Herman TS, Priebe W, Woynarowski JM (November 2004). “Enhanced topoisomerase II targeting by annamycin and related 4-demethoxy anthracycline analogues”. Mol Cancer Ther. 3 (11): 1403–10. doi:10.1158/1535-7163.1403.3.11. PMID 15542779.
External links
| Clinical data | |
|---|---|
| ATC code | none |
| Identifiers | |
| IUPAC name | |
| CAS Number | 92689-49-1 |
| PubChem CID | 115212 |
| ChemSpider | 103088 |
| UNII | SNU299M83Q |
| KEGG | D12844 |
| CompTox Dashboard (EPA) | DTXSID901027238 |
| ECHA InfoCard | 100.235.298 |
| Chemical and physical data | |
| Formula | C26H25IO11 |
| Molar mass | 640.379 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| SMILES | |
| InChI | |
//////////naxtarubicin, DNA topoisomerase II inhibitor, antineoplastic, Annamycin, Annamycin-LF, Annamycin-liposomal, L-ANNA, L-annamycin, Liposomal annamycin, S-ANNA, SNU299M83Q
Navepdekinra
Navepdekinra
CAS 2467732-66-5
MF C33H48FN7O4 MW625.78
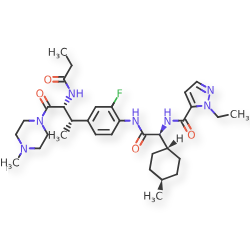
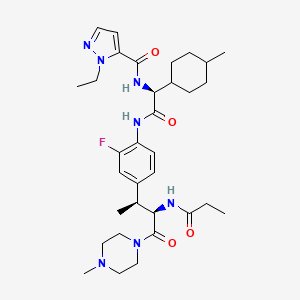
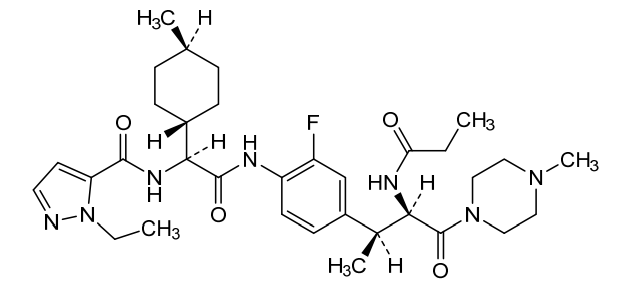
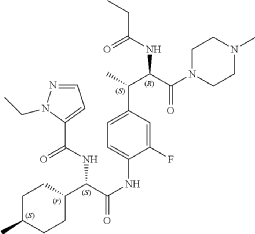
1H-Pyrazole-5-carboxamide, 1-ethyl-N-[(1S)-2-[[2-fluoro-4-[(1S,2R)-1-methyl-3-(4-methyl-1-piperazinyl)-3-oxo-2-[(1-oxopropyl)amino]propyl]phenyl]amino]-1-(trans-4-methylcyclohexyl)-2-oxoethyl]-
1-ethyl-N-{(1S)-2-{2-fluoro-4-[(2S,3R)-4-(4-methylpiperazin-1-yl)-4-oxo-3-propanamidobutan-2-yl]anilino}-1-[(1r,4S)-4-methylcyclohexyl]-2-oxoethyl}-1H-pyrazole-5-carboxamide
1-ethyl-N-{(1S)-2-{2-fluoro-4-[(2S,3R)-4-(4-methylpiperazin-1-yl)-4-oxo-3-propanamidobutan-2-
yl]anilino}-1-[(1r,4S)-4-methylcyclohexyl]-2-oxoethyl}-1H-pyrazole-5-carboxamide
interleukin-17A (IL-17A) inhibitor, anti-inflammatory, DC-806, LY4100504, DC 806, LY 4100504, Y64F9MC2QM
Navepdekinra (also known as DC-806 or LY4100504) is an experimental, orally active small-molecule inhibitor of interleukin-17A (IL-17A). It was primarily developed to treat autoimmune and inflammatory conditions, such as psoriasis, by disrupting the interaction between IL-17A and its receptor.
Key Properties and Development
- Mechanism: It is a potent inhibitor with an IC50 of 10.81 nM, designed to provide an oral alternative to existing injectable IL-17 biologic therapies.
- Acquisition: The drug was originally developed by DICE Therapeutics, which was acquired by Eli Lilly and Company in 2023 for approximately $2.4 billion to bolster their immunology pipeline.
Navepdekinra (DC-806) is an orally active, potent interleukin-17A (IL-17A) inhibitor (IC50 = 10.81 nM). Navepdekinra disrupts the IL-17A protein-receptor interaction, suppressing the downstream pro-inflammatory signaling pathway. Navepdekinra inhibits arthritis in a collage-induced arthritis (CIA) rat model. Navepdekinra can be used for psoriasis, psoriatic arthritis, and ankylosing spondylitis
SYN
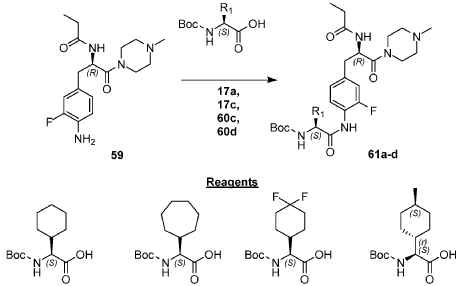
Example 210: N-[(2R,3S)-3-{4-[(2S)-2-[(1-ethyl-1H-pyrazol-5-yl)formamido]-2-[(1r,4S)-4-methylcyclo hexyl]acetamido]-3-fluorophenyl}-1-(4-methylpiperazin-1-yl)-1-oxobutan-2-yl]propanamide) (234)
Following General Procedure R, 0.227 g, 0.310 mmol, 1.0 eq) of 82d in DMF (1 mL) were added 1-ethyl-1H-pyrazole-5-carboxylic acid (0.052 g, 0.372 mmol, 1.2 eq), DIPEA (0.43 mL, 2.482 mmol, 8.0 eq) and then HATU (0.177 g, 0.465 mmol, 1.5 eq.) and the resulting mixture was stirred at RT for 1 h. The mixture was concentrated to dryness and the residue was purified via reverse phase column chromatography on a 120 g C18 cartridge eluting with a 5-95% H 2O:MeCN eluent (0.1% ammonia) to afford 234 (0.025 g) as a white solid. 1H NMR (400 MHz, DMSO-d 6) δ 9.86 (s, 1H), 8.46 (d, J=8.3 Hz, 1H), 8.26 (d, J=8.7 Hz, 1H), 7.75 (t, J=8.3 Hz, 1H), 7.47 (d, J=2.1 Hz, 1H), 7.15-7.07 (m, 1H), 7.05-6.97 (m, 2H), 4.86 (t, J=9.4 Hz, 1H), 4.53 (t, J=8.4 Hz, 1H), 4.47 (q, J=7.2 Hz, 2H), 3.46-3.38 (m, 2H), 3.29-3.14 (m, 2H), 3.12-2.99 (m, 2H), 2.25-2.03 (m, 5H), 1.98 (s, 3H), 1.81 (ddt, J=15.0, 9.9, 5.6 Hz, 2H), 1.74-1.60 (m, 4H), 1.58-1.47 (m, 1H), 1.28 (t, J=7.1 Hz, 4H), 1.20 (d, J=7.0 Hz, 3H), 1.14-1.02 (m, 1H), 0.99 (t, J=7.6 Hz, 3H), 0.93-0.87 (m, 1H), 0.86 (d, J=6.5 Hz, 3H). UPLC-MS (basic 4 min): rt=1.76 min; m/z=626.4 for [M+H] +.
PAT
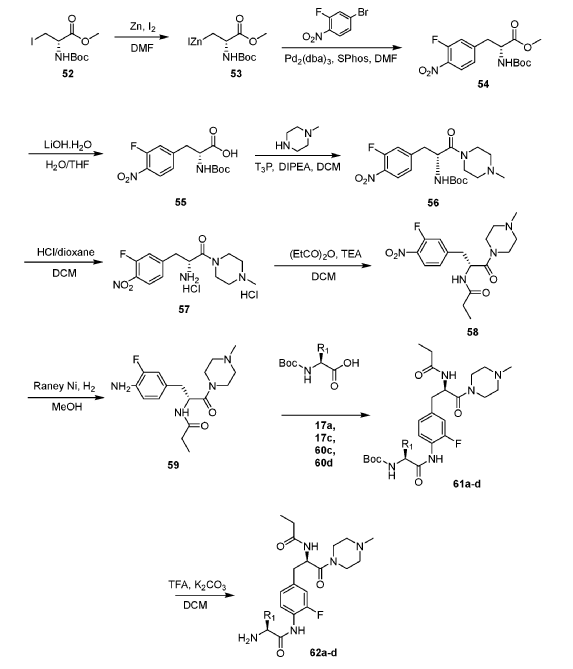
Example 1: Exemplary Scheme—Synthesis of Intermediate Compounds 62a-62d
PAT
IL-17 Ligands And Uses Thereof
Publication Number: US-2020247785-A1
Priority Date: 2019-02-06
- Substituted benzenecarboxamides as IL-17A modulatorsPublication Number: US-11274094-B2Priority Date: 2019-09-16Grant Date: 2022-03-15
- Il-17a modulators and uses thereofPublication Number: US-2021101886-A1Priority Date: 2019-09-16
- IL-17 ligands and uses thereofPublication Number: US-11447468-B2Priority Date: 2019-02-06Grant Date: 2022-09-20
- Il-17 ligands and uses thereofPublication Number: US-2023053746-A1Priority Date: 2019-02-06
- IL-17 ligands and uses thereofPublication Number: US-12234225-B2Priority Date: 2019-02-06Grant Date: 2025-02-25
- Mannose 6-phosphate or asgpr receptor binding compounds for the degradation of extracellular proteinsPublication Number: WO-2023028338-A2Priority Date: 2021-08-27
- Potent asgpr-binding compounds for the degradation of immunoglobulins and other proteinsPublication Number: WO-2022235699-A2Priority Date: 2021-05-03
- Il-17a modulators and uses thereofPublication Number: WO-2021055376-A1Priority Date: 2019-09-16
- Substituted benzenecarboxamides as il-17a modulatorsPublication Number: US-2023141212-A1Priority Date: 2019-09-16
- Substituted benzenecarboxamides as il-17a modulatorsPublication Number: US-2023145481-A1Priority Date: 2019-09-16
AS ON OCT2025 4.511 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
- [1]. Paul R. Fatheree, et al. IL-17 Ligands And Uses Thereof. US20200247785A1.[2]. Kim D, et al. Next-Generation Anti-IL-17 Agents for Psoriatic Disease: A Pipeline Review. Am J Clin Dermatol. 2025 May;26(3):307-320. [Content Brief][3]. Xiaobing Deng, et al. The Critical and Unexpected Role of a Methyl Group in Interleukin-17A Inhibitors. bioRxiv 2025.10.02.680113
//////////navepdekinra, interleukin-17A (IL-17A) inhibitor, anti-inflammatory, DC-806, LY4100504, DC 806, LY 4100504, Y64F9MC2QM
Napazimone
Napazimone
CAS 1800405-30-4
MF C14H12N2O2 MW240.26 g/mol
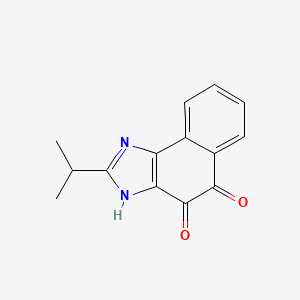
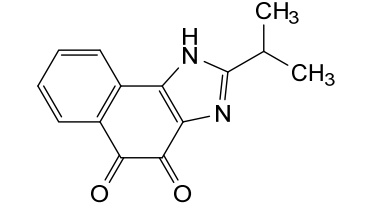
2-(propan-2-yl)-1H-naphtho[1,2-d]imidazole-4,5-dione
NAD(P)H dehydrogenase [quinone] 1 (NQO1) activator, KL 1333, KL-1333, NA2ZOL5UGM
Napazimone (also known as KL1333) is an investigational small molecule drug currently being developed for the treatment of primary mitochondrial disease. It is an orally available modulator that aims to improve energy production in patients with rare genetic conditions affecting mitochondrial DNA (mtDNA).
Mechanism of Action
According to ProbeChem.com and Synapse, Napazimone works through the following mechanisms:
- NAD+ Modulation: It increases intracellular levels of NAD+ by reacting with the enzyme NQO1, which helps shift the NAD+/NADH ratio.
- Signaling Pathway Activation: The drug activates the SIRT1/AMPK/PGC-1α signaling network, which is critical for regulating mitochondrial biogenesis and function.
- Mitochondrial Improvement: In laboratory studies using MELAS (Mitochondrial Encephalomyopathy, Lactic Acidosis, and Stroke-like episodes) fibroblasts, the compound increased ATP levels and decreased harmful reactive oxygen species (ROS) and lactate.
Clinical Development and Indications
Napazimone is being developed by Pharming Group for adult patients with primary mitochondrial disease, a condition often characterized by extreme fatigue and muscle weakness.
- Trial Status: As of early 2026, the drug is in Phase II/III clinical trials.
- FALCON Trial: A pivotal study known as the FALCON trial is currently ongoing, with a data readout expected in 2027.
- Potential Indications: It is primarily being investigated for mtDNA-driven mitochondrial diseases and has shown potential in research for protecting against hearing loss (ototoxicity) caused by chemotherapy drugs like cisplatin.
Chemical Properties
The following specifications are provided by Inxight Drugs and PubChem:
- Chemical Name: 2-isopropyl-3H-naphtho[1, 2-d]imidazole-4,5-dione.
- Molecular Formula: C14H12N2O2.
- Molecular Weight: 240.26 g/mol.
Would you like more information on the FALCON clinical trial or details about the mitochondrial diseases Napazimone is intended to treat?
- Efficacy of KL1333 in Adult Patients With Primary Mitochondrial DiseaseCTID: NCT05650229Phase: Phase 2Status: RecruitingDate: 2025-10-09
- A Phase Ia/Ib, SAD and MAD Study of of KL1333 in Healthy Subjects and Patients With Primary Mitochondrial DiseaseCTID: NCT03888716Phase: Phase 1Status: CompletedDate: 2021-10-20
- Drug-drug Interaction Study of KL1333 in Healthy SubjectsCTID: NCT04643249Phase: Phase 1Status: CompletedDate: 2021-10-20
- Safety, Tolerability and Pharmacokinetic Study of KL1333 in Healthy Male VolunteersCTID: NCT03056209Phase: Phase 1Status: CompletedDate: 2018-04-27
SYN
Example 1 [Synthesis of Compound 1]: 2-isopropyl-lH-naphtho [2, l-d] imidazole-4,5-dione
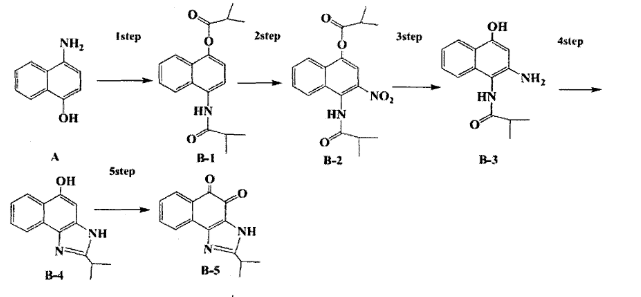
1) IStep Pyridine (5 ml) is added to compound A (4-amino-1 -naphthol hydrochloride, 500 mg, 2.55 mmol), and the ice bath is dehydrated and cooled. This is followed by dropwise isobutyric anhydride (1.7 ml, 10.2 mmol). The reaction product is stirred for 2.5 hours at the same temperature. The reactants are quenched with methanol and concentrated under reduced pressure to remove any pyridine. After adding EA and distilled water, adjust pH to about 6.5 with 1 N HC1 solution, and then wash the organic layer several times to remove the remaining pyridine. The organic layer was dried over Na 2 S0 4 , filtered and concentrated under reduced pressure. The concentrated reaction product was purified by silica gel column chromatography to obtain compound B-1 (686 mg, 90%).
2) 2Step
Add Acetic anhydride (3 ml) to Compound B-1 (300 mg, 1.00 mmol) and dropwise fuming nitric acid (0.20 ml, 2.00 mmol) at 0 ° C. The reaction product is stirred for 1 hour and then filtered. The filtered solid is then washed several times with Hexane with compound B-2. compound B-2 (217 mg, 63%).
1 H NMR (300 MHz, Acetone-d 6 ) δ 9.55 (s, IH), 8.33 (d, J = 6.6 Hz, IH), 8.06 (d, J = 6.2 Hz, IH), 7.86 (s, IH), 7.81-7.73 (m, 2H), 3.16-3.07 (m, IH), 2.96-2.87 (m, IH), 1.41 (d, J-7.0 Hz, 6H), 1.25 (d, J-7.0 Hz, 6H)
3) 3 Step
Compound B-2 (500 mg, 1.45 mmol) is dissolved in ethanol (5 ml), and then Pd / C (50 mg) and Hydrazine (0.29 ml, 5.81 mmol) are added in this order. The reaction is allowed to react for 1 hour at 70 degrees. The reaction product is cooled to room temperature and the Pelite / C is removed by celite filter. The filtrate is concentrated under reduced pressure and purified by silica gel column chromatography to obtain compound B-3 (232 mg, 51%).
MR NMR (300 MHz, CD 3 OD) δ 8.02 (d, J = 8.4 Hz, IH), 7.50 (d, J = 8.0 Hz, IH), 7.35 (t, J-8.0 Hz, IH), 7.13 (t, J = 8.1 Hz, IH), 6.47 (s, IH), 2.85-2.83 (m, IH), 1.31 (d, J = 7.0 Hz, 6H)
LC-MS m / z 245.1 (M + l)
4) 4Step
Acetic acid (15 ml) is added to Compound B-3 (700 mg, 2.86 mmol), and the mixture is stirred and refluxed for 3 hours. Acetic acid is removed by concentration under reduced pressure, and purified by silica gel column chromatography to obtain compound B-4 (575 mg, 89%) ¾-
MR NMR (300 MHz, CD 3 OD) δ 8.30 (d, J = 8.4 Hz, 2H), 7.60 (t, J = 8.0 Hz, IH), 7.47
(t, J = 8.1 Hz, IH), 6.99 (s, IH), 3.35-3.28 (m, IH), 1.46 (d, J = 7.0 Hz, 6H)
LC-MS m / z 227.0 (M + l)
5) 5 Step
Dissolve DMF (2.5 ml) in Compound B-4 (50 mg, 0.22 mmol), and add IBX (159 mg, 0.26 mmol). The reaction is reacted at room temperature for 1 hour. After adding EA, the organic layer is washed with NaHC0 3 saturated aqueous solution. The separated organic layer was dried over MgS0 4 and filtered. The filtrate was concentrated under reduced pressure and purified by column chromatography to obtain compound B-5 (47 mg, 89%).
1 H NM (300 MHz, CDC1 3 ) δ 9.96 (NH, s, IH), 8.06 (d, J = 7.7 Hz, IH), 7.99 (d, J = 7.7 Hz, IH), 7.65 (t, J = 7.7 Hz, IH), 7.44 (t, J = 7.7 Hz, IH), 3.26-3.17 (m, IH), 1.45 (d, j = 7.0 Hz, 6H)
PAT
1,2-naphthoquinone based derivative and method of preparing the same
Publication Number: US-10766882-B2
Priority Date: 2013-12-30
Grant Date: 2020-09-08
- 1,2-naphthoquinone based derivative and method of preparing the samePublication Number: US-2016376258-A1Priority Date: 2013-12-30
- 1,2-naphthoquinone based derivative and method of preparing the samePublication Number: CA-2935317-CPriority Date: 2013-12-30Grant Date: 2022-11-22
- 1,2-naphthoquinone derivative and method for preparing samePublication Number: EP-3091003-B1Priority Date: 2013-12-30Grant Date: 2025-06-04
- 1,2-naphthoquinone derivative and method for preparing samePublication Number: EP-4582424-A2Priority Date: 2013-12-30
- 1, 2-naphthoquinone derivative and preparation method thereofPublication Number: CN-105992759-BPriority Date: 2013-12-30Grant Date: 2020-10-30
AS ON OCT2025 4.511 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
////////////napazimone, NAD(P)H dehydrogenase [quinone] 1 (NQO1) activator, KL 1333, KL-1333, NA2ZOL5UGM
Nacresertib
Nacresertib
CAS 2629977-59-7
MF C22H26N4O4, 410.5 g/mol
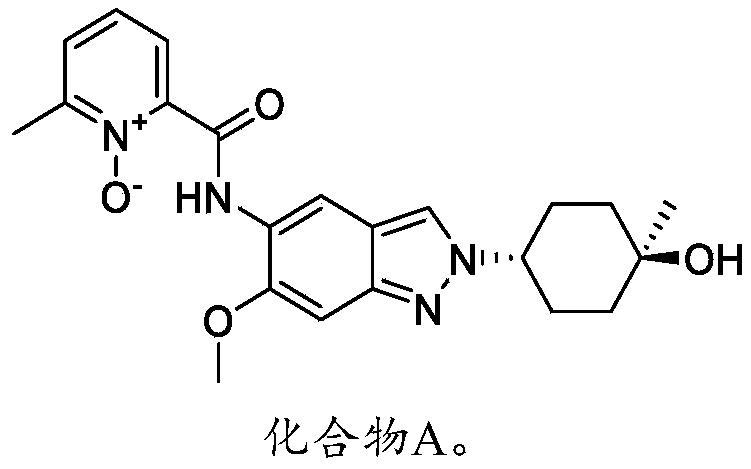
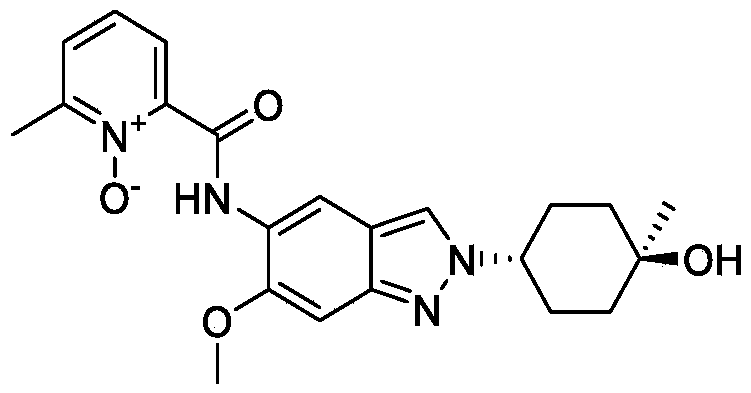
N-[2-(4-hydroxy-4-methylcyclohexyl)-6-methoxyindazol-5-yl]-6-methyl-1-oxidopyridin-1-ium-2-carboxamide
2-({2-[(1r,4r)-4-hydroxy-4-methylcyclohexyl]-6-methoxy-2H-indazol-5-yl}carbamoyl)-6-methylpyridine
1-oxide
serine/threonine kinase inhibitor, MB3QBD4BE7,
SYN
Example 1: Synthesis of Compound 001
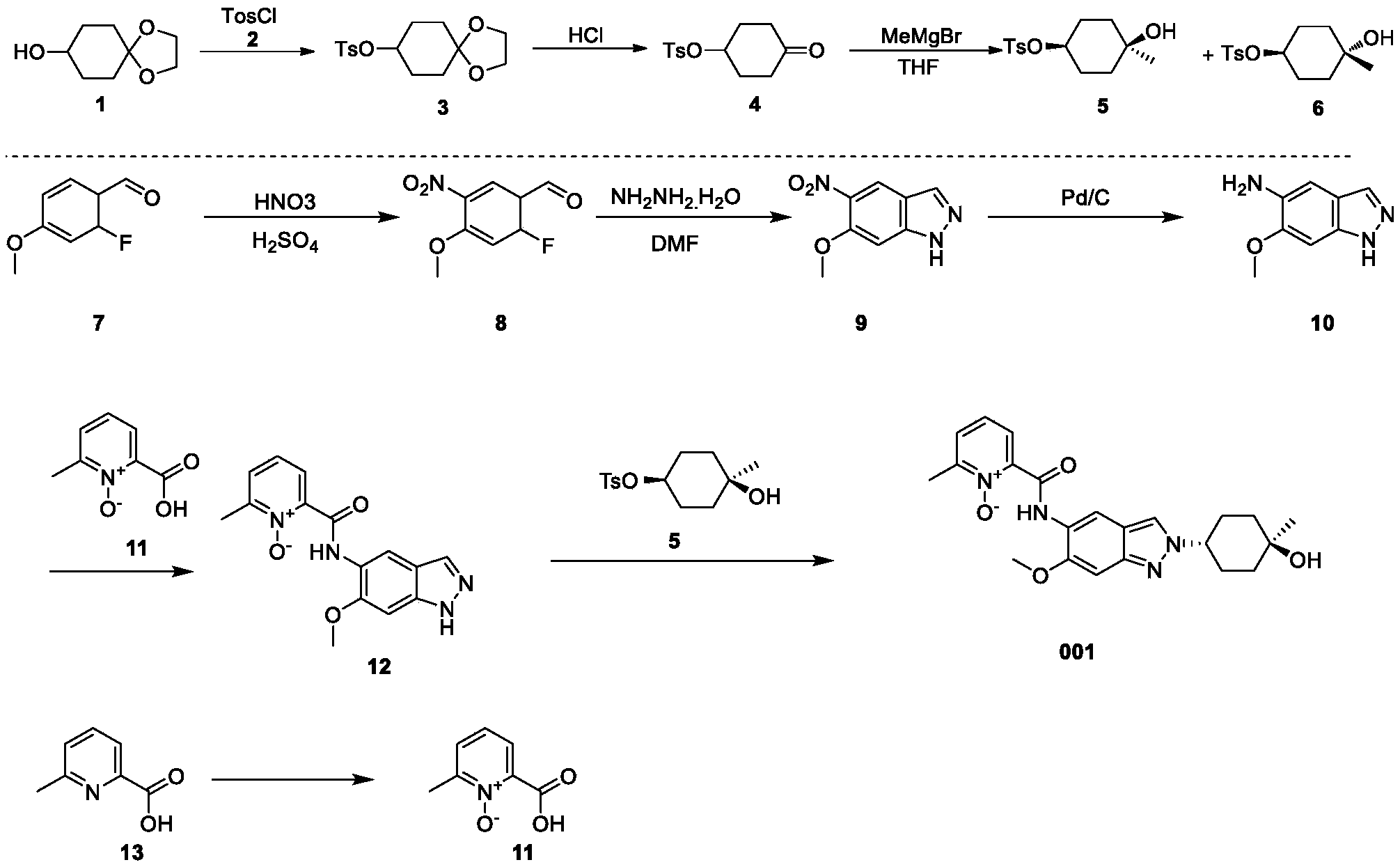
ynthesis of compound 001, namely 2-((2-(trans-4-hydroxy-cis-4-methylcyclohexyl)-6-methoxy-2H-indazol-5-yl)carbamoyl)-6-methylpyridine 1-oxide [0133]
[0134]Cesium carbonate (985 mg) was added to 5 mL of a DMF solution containing compound 12 (300 mg) and compound 5 (344 mg) at 25°C. The reaction mixture was stirred at 90°C for 16 hours. The reaction mixture was then added to 30 mL of water and extracted with ethyl acetate (10 mL * 3). The organic phase was concentrated under reduced pressure, and the residue was purified by preparative high-performance liquid chromatography (HPLC) using a column (CH3CN :
H2O ( 0.1 % NH4HCO3 ) = 15-45%, UV: 214 nm, flow rate: 15 mL/min) to obtain compound 001 (70 mg, yield 17%).[0135]
1 H NMR (400MHz, DMSO-d6): δ14.16(s,1H),8.78(s,1H),8.34(s,1H),8.32-8.30(m,1H),7.77(d,J=7.6Hz,1H),7.58(t,J=8.0Hz,1H),7.13(s,1 H),4.45(s,1H),4.43-4.40(m,1H),3.95(s,3H),2.53(s,3H),2.09-2.00(m,4H),1.68-1.58(m,4H),1.22(s,3H).LCMS: Rt=3.646min,[M+H] + =411.1.
SYN
2-((2-(trans-4-hydroxy-cis-4-methylcyclohexyl)-6-methoxy-2H-indazol-5-yl)carbamoyl)-6-methylpyridine 1-oxide as shown in the following formula:
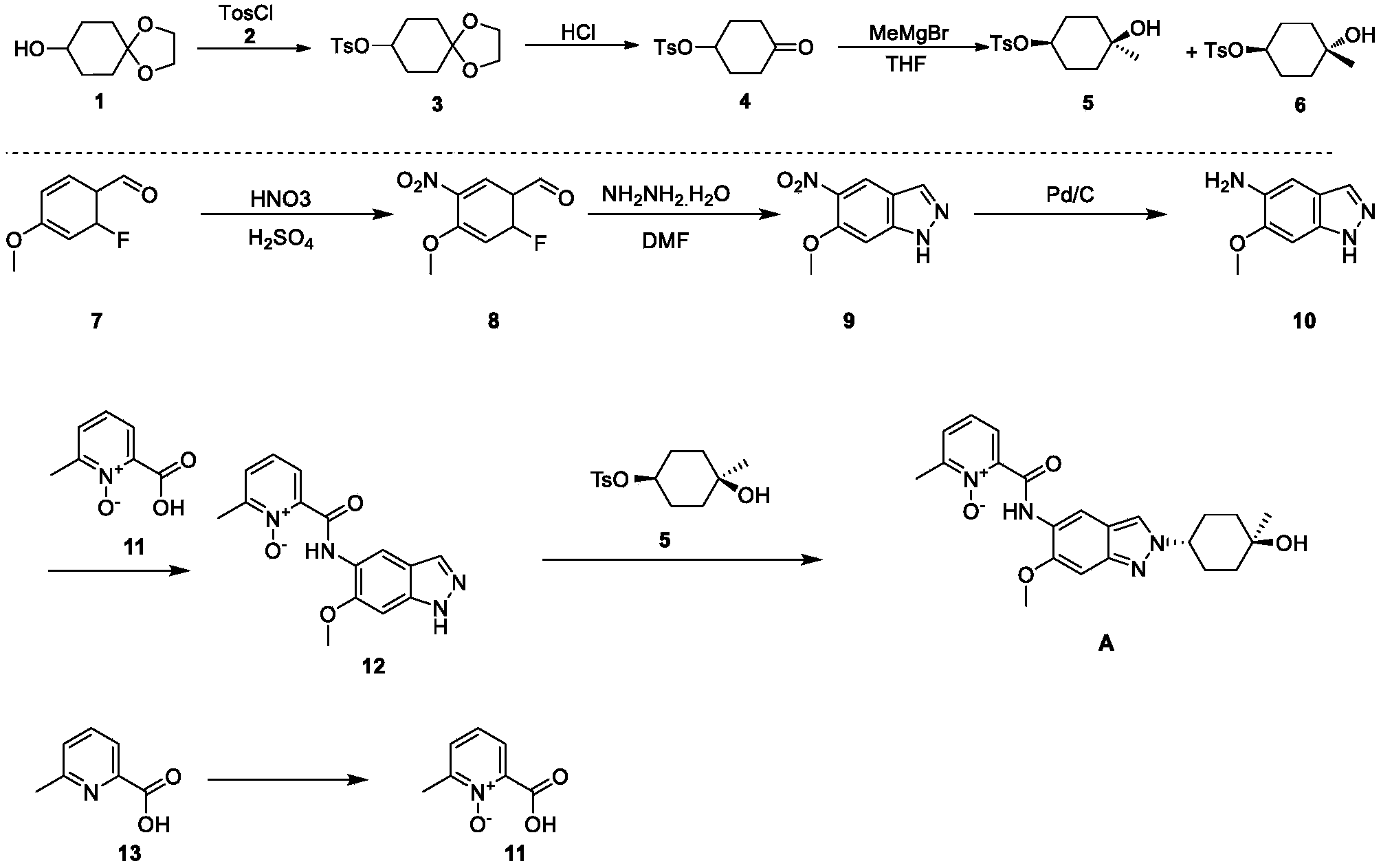
[0257](1) Synthesis of compound 3
[0258]DMAP (42.5 g), compound 2 (63.4 g), and triethylamine (63.9 g) were added sequentially to a 500 mL solution of compound 1 (50 g) in dichloromethane at 15°C, and the mixture was stirred at 25°C for 18 hours. Dichloromethane (200 mL) was added to the reaction mixture, followed by washing with water (300 mL × 2), then with 1 M dilute hydrochloric acid (300 mL × 3). The organic phase was dried over anhydrous sodium sulfate, filtered, and concentrated under reduced pressure to obtain 98 g of a yellow solid, yield: 99% (i.e., compound 3).
[0259](2) Synthesis of compound 4
[0260]1M dilute hydrochloric acid (300 mL) was added to a tetrahydrofuran solution (50 g) of compound 3 at 15°C, and the mixture was stirred at 25°C for 20 hours. The mixture was cooled to 0°C. The pH was adjusted to 9 with 1M sodium hydroxide solution. Extraction was performed with ethyl acetate (200 mL × 3). The extract was washed with saturated sodium chloride solution (300 mL). The solution was dried over anhydrous sodium sulfate. The mixture was filtered. The solution was concentrated under reduced pressure, and the residue was slurried with petroleum ether (150 mL) to give 39 g of a white solid, 91% yield (i.e., compound 4).
[0261](3) Synthesis of compounds 5 & 6
[0262]At -40°C, a tetrahydrofuran solution (200 mL) of compound 4 (34.5 g) was added dropwise to a tetrahydrofuran solution (500 mL) of methyl magnesium bromide (85.8 mL). The mixture was stirred at -40°C for 4 hours. The reaction was quenched with a saturated ammonium chloride solution (100 mL). The mixture was extracted with ethyl acetate (500 mL × 3). The extract was washed with saturated brine (300 mL), dried over anhydrous sodium sulfate, filtered, concentrated under reduced pressure, and the residue was purified by silica gel column chromatography (petroleum ether: ethyl acetate = 5:1) to give a colorless oily compound 5 (4.3 g, 10%), a colorless oily compound 6 (7.0 g, 17%), and a mixture of 12 g.
[0264]
1H NMR (400MHz,CDCl3 ) : δ7.79(d,J=8.0Hz,2H), 7.32(d,J=8.4Hz,2H), 4.52-4.41(m,1H), 2.44(s,3H), 1.95-1.80(m,2H), 1.77-1.61(m,4H), 1.46-1.35(m,2H), 1.19(s,3H).
[0266]
1H NMR (400MHz,CDCl3 ) : δ7.79(d,J=8.4Hz,2H), 7.33(d,J=8.0Hz,2H), 4.74-4.64(m,1H), 2.44(s,3H), 1.92-1.79(m,2H), 1.77-1.62(m,4H), 1.49-1.38(m,2H), 1.23(s,3H).
[0267](4) Synthesis of compound 8
[0268]A mixture of concentrated sulfuric acid (1.6 mL, 98%) and nitric acid (1.6 mL, 70%) was added dropwise to a solution of compound 7 (2.0 g) in concentrated sulfuric acid (12 mL, 98%) at -15°C. After the addition was complete, the mixture was stirred at -15°C for 2 hours. The reaction solution was then slowly poured into ice water and stirred for 5 minutes. The mixture was filtered, washed with water, and the solid was collected and dried under reduced pressure to give 2.5 g of a yellow solid, yield: 97% (i.e., compound 8).
[0269](5) Synthesis of compound 9
[0270]Hydrazine hydrate (2.4 mL, 98%) was added to a DMF (20 mL) solution of compound 8 (2.0 g) at room temperature. After the addition was complete, the mixture was heated to 120 °C and stirred for 16 hours. After cooling to room temperature, the mixture was slowly poured into ice water and stirred. The mixture was filtered, the solid was washed with water, and the solid was collected and concentrated under reduced pressure to obtain 1.3 g of yellow solid. Yield: 67% (i.e., compound 9).
[0271](6) Synthesis of compound 10
[0272]Compound 9 (12.4 g) and palladium on carbon (7 g, 10%) were added sequentially to 400 mL of ethyl acetate at 15°C. After the addition was complete, the mixture was stirred for 18 hours under hydrogen protection at 15°C. The palladium on carbon was filtered off from the reaction solution, and the filtrate was concentrated and evaporated to dryness to obtain 10.4 g of white solid product, with a yield of 99% (i.e., compound 10).
[0273](7) Synthesis of compound 12
[0274]EDCI.HCl (2.6 g) was added to a Py (15 mL) solution of compound 10 (1.5 g) and compound 11 (1.4 g) at 25°C. The reaction mixture was stirred at 25°C for 16 hours. The reaction mixture was concentrated and evaporated to dryness. The residue was slurried by passing MeOH/H₂O ( 20 mL/20 mL) to obtain 1.3 g of a yellow solid product, with a yield of 48% (i.e., compound 12).
[0275](8) Synthesis of compound A
[0276]
[0277]Cesium carbonate (985 mg) was added to 5 mL of a DMF solution containing compound 12 (300 mg) and compound 5 (344 mg) at 25°C. The reaction mixture was stirred at 90°C for 16 hours. The reaction mixture was then added to 30 mL of water and extracted with ethyl acetate (10 mL × 3). The organic phase was concentrated under reduced pressure, and the residue was purified by preparative high-performance liquid chromatography (HPLC) using a column (CH3CN :
H2O (
0.1 % NH4HCO3
) = 15-45%, UV: 214 nm, Flowrate: 15 mL/min) to obtain 70 mg of a yellow solid, with a yield of 17% (i.e., compound A).
[0278]
1H NMR(400MHz,DMSO-d6):δ14.16(s,1H),8.78(s,1H),8.34(s,1H),8.32-8.30(m,1H),7.77(d,J=7.6Hz,1H),7.58(t,J=8.0Hz,1H),7.13(s,1H),4.45(s,1H),4.43-4.40(m,1H),3.95(s,3H),2.53(s,3H),2.09-2.00(m,4H),1.68-1.58(m,4H),1.22(s,3H).LCMS:Rt=3.646min,[M+H] +=411.1.
PAT
- Irak inhibitor and preparation method therefor and use thereofPublication Number: EP-4015513-B1Priority Date: 2019-09-24Grant Date: 2023-11-01
- An IRAK inhibitor and its preparation method and usePublication Number: CN-114391013-BPriority Date: 2019-09-24Grant Date: 2024-01-26
- Irak inhibitor and preparation method therefor and use thereofPublication Number: US-2022298139-A1Priority Date: 2019-09-24
- A kind of IRAK inhibitor and its preparation method and usePublication Number: CN-114391013-APriority Date: 2019-09-24
- A kind of polymorphic form of compound and its preparation method and applicationPublication Number: CN-115109035-APriority Date: 2021-03-19
- Polymorphic forms of compound and preparation method therefor and application thereofPublication Number: EP-4310080-A1Priority Date: 2021-03-19
- Polymorphic forms of compound and preparation method therefor and application thereofPublication Number: US-2024182443-A1Priority Date: 2021-03-19
- Preparation method for fused pyrazole-type compoundPublication Number: US-2023250064-A1Priority Date: 2020-06-23
- An IRAK inhibitor and its preparation method and usePublication Number: CN-118146193-APriority Date: 2019-09-24
- IRAK4 inhibitor composition, and preparation method and application thereofPublication Number: CN-115252609-BPriority Date: 2022-08-01Grant Date: 2023-05-26
- Irak4 inhibitor composition, preparation method therefor and use thereofPublication Number: EP-4566607-A1Priority Date: 2022-08-01
- Composition of IRAK4 inhibitor, preparation method and application thereofPublication Number: CN-115252609-APriority Date: 2022-08-01
- Use of indazoles for treating psoriasisPublication Number: CN-114404415-APriority Date: 2022-02-25
- Use of indazole compound for treating psoriasisPublication Number: US-2025161283-A1Priority Date: 2022-02-25
AS ON OCT2025 4.511 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
//////////nacresertib, serine/threonine kinase inhibitor, MB3QBD4BE7,
Mosperafenib
Mosperafenib
CAS 2649372-20-1
MF C20H17F2N5O4S MW 461.4 g/mol
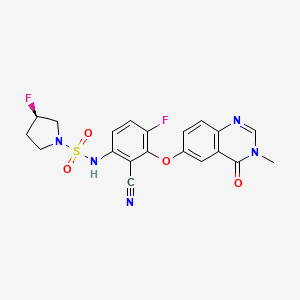
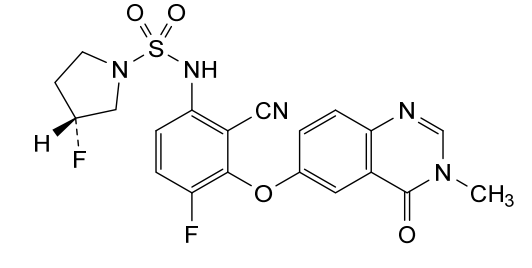
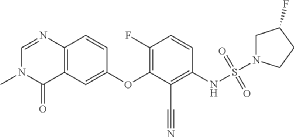
- (3R)-N-{2-cyano-4-fluoro-3-[(3-methyl-4-oxo-3,4-dihydroquinazolin-6-yl)oxy]phenyl}-3-fluoropyrrolidine-1-sulfonamide
- (3R)-N-(2-cyano-4-fluoro-3-((3-methyl-4-oxo-3,4-dihydroquinazolin-6-yl)oxy)phenyl)-3-fluoropyrrolidine-1-sulfonamide
(3R)-N-{2-cyano-4-fluoro-3-[(3-methyl-4-oxo-3,4-dihydroquinazolin-6-yl)oxy]phenyl}-3-fluoropyrrolidine-1-sulfonamide
B-Raf (BRAF) inhibitor, antineoplastic, RG6344, RO7276389, RG 6344, RO 7276389, 881-730-4, B-Raf IN 2
Mosperafenib is a small molecule drug. The usage of the INN stem ‘-rafenib’ in the name indicates that Mosperafenib is a Raf (rapidly accelerated fibrosarcoma) kinase inhibitor. Mosperafenib has a monoisotopic molecular weight of 461.1 Da.
Mosperafenib (RG6344, RO7276389) is an investigational, oral, “paradox-breaker” BRAF inhibitor developed by Roche for treating BRAF-mutated cancers, particularly BRAF V600E-mutant metastatic colorectal cancer. It acts as a potent, selective inhibitor that avoids MAPK pathway overactivation in non-V600E contexts, showing superior preclinical activity and brain penetration compared to existing inhibitors like encorafenib.
Key Aspects of Mosperafenib:
- Mechanism: As a “paradox-breaker” BRAF inhibitor, it avoids the paradoxical MAPK pathway activation seen with earlier inhibitors. It inhibits BRAF mutants (
) and is effective in RAF dimer-mediated resistant models.
- Clinical Development: Currently in Phase I clinical trials for BRAF V600E-mutant colorectal cancer.
- Preclinical Performance: In studies, it demonstrated higher antitumor activity than encorafenib/cetuximab combinations, even in BRAFi-naïve models.
- Combination Potential: It is being evaluated in combination with cetuximab and FOLFOX.
- Targeting: It targets BRAF V600E/K/A/D mutations.
- OriginatorRoche
- ClassAntineoplastics; Fluorinated hydrocarbons; Fluorobenzenes; Nitriles; Phenyl ethers; Pyridones; Pyrrolidines
- Mechanism of ActionProto-oncogene protein b-raf inhibitors
- Phase IMalignant melanoma; Solid tumours
- 18 Sep 2025Chemical structure information added.
- 30 May 2025Efficacy, pharmacokinetics and adverse events data from a phase I trial in Solid tumors presented at the 61st Annual Meeting of the American Society of Clinical Oncology (ASCO-2025)
- 25 Apr 2025Efficacy, pharmacokinetics and adverse events data from a phase I trial in Solid tumors presented at the 116th Annual Meeting of the American Association for Cancer Research (AACR-2025)
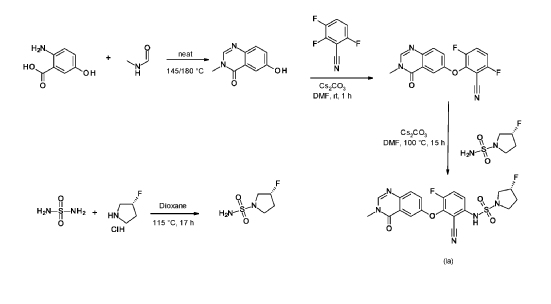
SYN
SYN
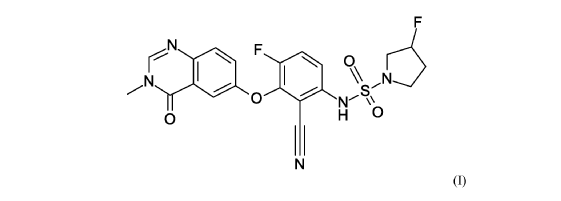
3R)-N-[2-cyano-4-fluoro-3-(3-methyl-4-oxo-quinazolin-6-yl)oxy-phenyl]-3-fluoro-pyrrolidine-1-sulfonamide (Example 1)
R)-3-Fluoropyrrolidine-1-sulfonamide (1.26 g, 7.51 mmol, Eq: 2.1) and cesium carbonate (2.56 g, 7.87 mmol, Eq: 2.2) were suspended in dry DMF (10.2 ml) under an argon atmosphere. The reaction was stirred at 50° C. for 30 min. The reaction mixture was cooled to rt and a solution of 3,6-difluoro-2-((3-methyl-4-oxo-3,4-dihydroquinazolin-6-yl)oxy)benzonitrile (1.12 g, 3.58 mmol, Eq: 1.0) in DMF (25.5 ml) was added. The reaction mixture was stirred at 100° C. for 15 h, then concentrated in vacuo. The residue was taken up in sat. aq. NH 4Cl (100 mL) and EtOAc (100 mL). The phases were separated, and the aqueous layer was extracted further with 2×100 mL EtOAc. The combined organic layers were washed with water (200 mL) and brine (200 mL), dried (Na 2SO 4), filtered and concentrated in vacuo. The water layer was back-extracted with EtOAc (3×100 mL). The combined organic extracts were washed with brine (200 mL), dried (Na 2SO 4), filtered and concentrated in vacuo. The residue was diluted with DCM and MeOH, and concentrated onto silica. Purification by flash chromatography (120 g, 0.5-2% MeOH/DCM) gave an off-white solid which was triturated with 1:1 heptane/DCM (20 mL) with sonication, then dried in vacuo to give the title compound as a colourless solid (1.087 g, 66% yield). MS (ESI) m/z: 426.2 [M+H] +. Chiral SFC: RT=4.594 min [Chiralpak IC column, 4.6×250 mm, 5 μm particle size (Daicel); gradient of 20-40% MeOH containing 0.2% NHEt 2 over 8 min; flow: 2.5 mL/min; 140 bar backpressure].
SYN
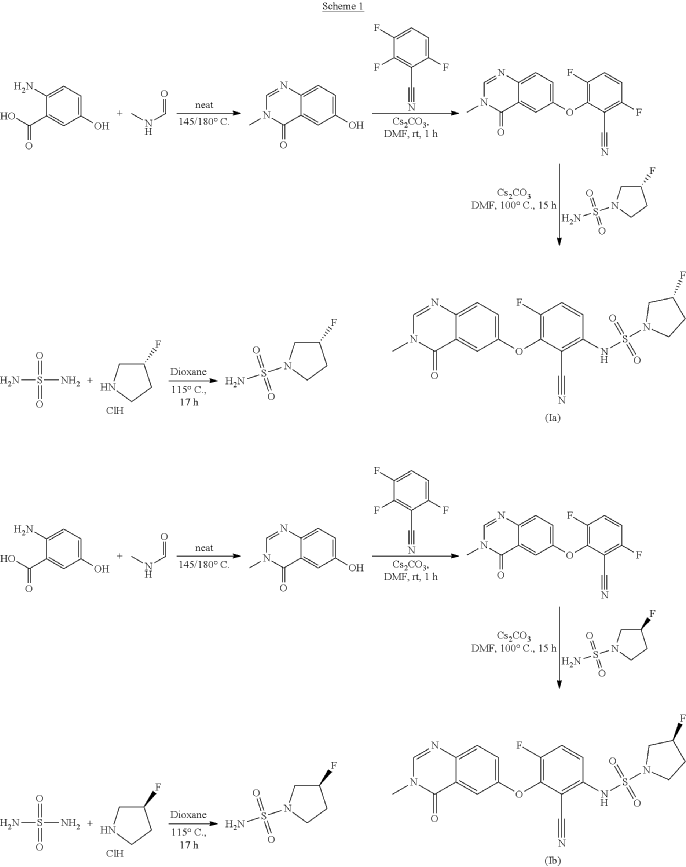
Refences compounds AR-25, AR-30 and AR-31 were prepared according to the synthesis disclosed in WO2012/118492 in example 25, example 30 and example 31 respectively.
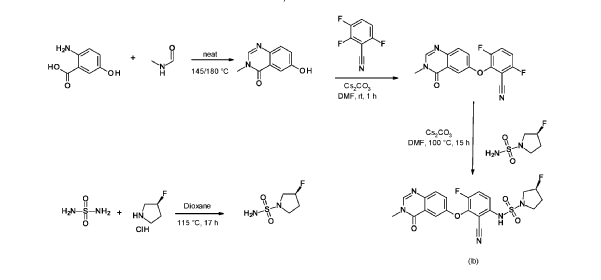
6-hydroxy-3-methyl-quinazolin-4-one
2-Amino-5-hydroxybenzoic acid (10 g, 65.3 mmol, Eq: 1.0) and A-methylformamide (30 g, 29.9 mL, 503 mmol, Eq: 7.7) were heated at 145 °C for 21 h 45 min, then cooled to rt. The reaction mixture was diluted with 50 mL H2O and stirred at rt for 20 min. The resulting precipitate was collected by filtration. The light brown solid was washed 3 × with 20 mL water. The solid was taken up in toluene and evaporated to dryness (3 ×). The solid was dried in vacuo at 40 °C overnight under high vacuum to give the title compound as a light brown solid (10.3 g, 89% yield). MS (ESI) mlz: 177.1 [M+H]+.
3.6-difluoro-2-(3-methyl-4-oxo-quinazolin-6-yl)oxy-benzonitrile
Cesium carbonate (3.22 g, 9.79 mmol, Eq: 1.15) was added at rt to a solution of 6-hydroxy-3-methylquinazolin-4-one (1500 mg, 8.51 mmol, Eq: 1.0) in N,N-dimethylformamide (35 mL). The mixture was stirred for 30 min at rt then 2,3,6-trifluorobenzonitrile (1.47 g, 1.08 ml, 9.37 mmol, Eq: 1.1) was added. After 1 h, the reaction was cooled on ice and diluted with water (120 mL). The resultant solid was collected by filtration, washed with iced water (100 mL) and heptane (100 mL) and suction-dried. The solid was taken up in toluene and evaporated to dryness (3 ×) then dried overnight in vacuo to give the title compound as a light brown solid (2.58 g, 97% yield). MS (ESI) m/z: 314.1 [M+H]+.
(3R)-3 -fluoropyrrolidine- 1 -sulfonamide
(R)-3 -Fluoropyrrolidine hydrochloride (1.8 g, 14.3 mmol, Eq: 1.2) was added to a solution of sulfuric diamide (1.148 g, 11.9 mmol, Eq: 1.0) and triethylamine (2.42 g, 3.33 mL, 23.9 mmol, Eq: 2) in dioxane (10 mL). The reaction was stirred in a sealed tube at 115 °C for 15.5 h then cooled to rt and concentrated in vacuo. The residue was diluted with DCM, evaporated with silica gel to dryness and transferred to a column. Purification by flash chromatography (40 g silica, 80% EtOAc) gave the title compound as a white crystalline solid (1.82 g, 91% yield). MS (ESI) m/z: 169.1 [M+H]+.
(3S)-3 -fluoropyrrolidine- 1 -sulfonamide
Triethylamine (304 mg, 419 μl, 3.01 mmol, Eq: 2.0) was added to a suspension of sulfuric diamide (146 mg, 1.5 mmol, Eq: 1.0) and (S)-3 -fluoropyrrolidine hydrochloride (234 mg, 1.8 mmol, Eq: 1.2) in dioxane (1.3 ml). The reaction was stirred in a sealed tube at 115°C for 16 h 35 min, then concentrated in vacuo. The residue was diluted with MeOH and evaporated with silica gel to dryness and transferred to a column. Purification by flash chromatography (40 g silica, 0-8% MeOH/DCM) gave the title compound as a light yellow solid (193 mg, 75% yield). MS (ESI) m/z: 169.1 [M+H]+.
(3R)-N-[2-cyano-4-fluoro-3-(3-methyl-4-oxo-quinazolin-6-yl)oxy-phenyl]-3-fluoro-pyrrolidine-1 -sulfonamide (Example 1)
(R)-3-Fluoropyrrolidine-1-sulfonamide (1.26 g, 7.51 mmol, Eq: 2.1) and cesium carbonate (2.56 g, 7.87 mmol, Eq: 2.2) were suspended in dry DMF (10.2 ml) under an argon atmosphere. The reaction was stirred at 50 °C for 30 min. The reaction mixture was cooled to rt and a solution of 3,6-difluoro-2-((3-methyl-4-oxo-3,4-dihydroquinazolin-6-yl)oxy)benzonitrile (1.12 g, 3.58 mmol, Eq: 1.0) in DMF (25.5 ml) was added. The reaction mixture was stirred at 100 °C for 15 h, then concentrated in vacuo. The residue was taken up in sat. aq. NH4Cl (100 mL) and EtOAc (100 mL). The phases were separated, and the aqueous layer was extracted further with 2 x 100 mL EtOAc. The combined organic layers were washed with water (200 mL) and brine (200 mL), dried (Na2SO4), filtered and concentrated in vacuo. The water layer was back-extracted with EtOAc (3 x 100 mL). The combined organic extracts were washed with brine (200 mL), dried (Na2SO4), filtered and concentrated in vacuo. The residue was diluted with DCM and MeOH, and concentrated onto silica. Purification by flash chromatography (120 g, 0.5-2% MeOH/DCM) gave an off-white solid which was triturated with 1 : 1 heptane/DCM (20 mL) with sonication, then dried in vacuo to give the title compound as a colourless solid (1.087 g, 66% yield). MS (ESI) mlz: 426.2 [M+H]+. Chiral SFC: RT = 4.594 min [Chiralpak IC column, 4.6 x 250 mm, 5μm particle size (Daicel); gradient of 20 – 40% MeOH containing 0.2% NHEt2 over 8 min; flow: 2.5 mL/min; 140 bar backpressure],
(3S)-N-[2-cyano-4-fluoro-3-(3-methyl-4-oxo-quinazolin-6-yl)oxy-phenyl]-3-fluoro-pyrrolidine-1 -sulfonamide (Example 2)
(S)-3-Fluoropyrrolidine-1-sulfonamide (181 mg, 1.08 mmol, Eq: 2.1) was dissolved in DMF (1.6 ml). At rt cesium carbonate (368 mg, 1.13 mmol, Eq: 2.2) was added and the reaction mixture was stirred at 50 °C for 30 min. The reaction mixture was cooled to rt and a solution of 3,6-difluoro-2-((3-methyl-4-oxo-3,4-dihydroquinazolin-6-yl)oxy)benzonitrile (160.8 mg, 513 μmol, Eq: 1.0) in DMF (4 ml) was added. The reaction mixture was stirred at 105 °C for 2 h 50 min then concentrated in vacuo. The residue was taken up in DCM and washed with sat. aq. NH4Cl. The aq. layer was back-extracted twice with DCM. The combined organic layers were dried over Na2SO4, filtrated and evaporated. The residue (brown oil) was diluted with DCM and transferred to a column. Purification by flash chromatography (80 g, 0-100% EtOAc in DCM) gave a solid which was further purified by SFC to give the title compound as a light yellow solid (119 mg, 50% yield). MS (ESI) m/z: 426.2 [M+H]+. Chiral SFC: RT = 4.411 min [Chiralpak IC column, 4.6 x 250 mm, 5μm particle size (Daicel); gradient of 20 – 40% MeOH containing 0.2% NHEt2 over 8 min; flow: 2.5 mL/min; 140 bar backpressure].
PAT
New methylquinazolinone derivatives
Publication Number: AU-2020403443-A1
Priority Date: 2019-12-10
- Methylquinazolinone derivativesPublication Number: US-2024174621-A1Priority Date: 2019-12-10
- New methylquinazolinone derivativesPublication Number: EP-4073065-B1Priority Date: 2019-12-10Grant Date: 2025-02-19
- Methylquinazolinone derivativesPublication Number: US-2022298119-A1Priority Date: 2019-12-10
- Novel BRAF inhibitors as anomalous breakersPublication Number: CN-114746405-BPriority Date: 2019-12-10Grant Date: 2024-03-26
- New BRAF inhibitors as paradox breakersPublication Number: AU-2020403082-A1Priority Date: 2019-12-10
AS ON OCT2025 4.511 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
////////////////mosperafenib, B-Raf (BRAF) inhibitor, antineoplastic, RG6344, RO7276389, RG 6344, RO 7276389, 881-730-4, B-Raf IN 2
Mocaciclib
Mocaciclib
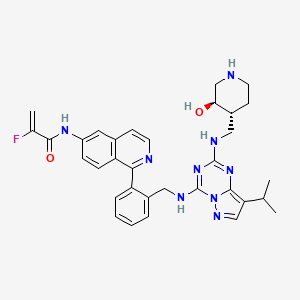
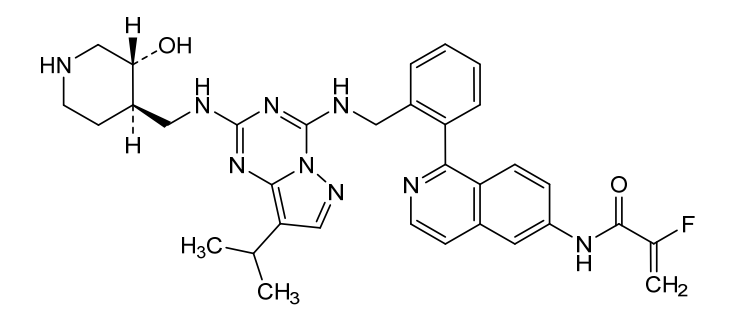
CAS 2766124-39-2
MF C33H36FN9O2 MW609.71
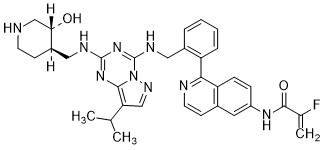
- 2-fluoro-N-[1-[2-[[[2-[[(3R,4R)-3-hydroxypiperidin-4-yl]methylamino]-8-propan-2-ylpyrazolo[1,5-a][1,3,5]triazin-4-yl]amino]methyl]phenyl]isoquinolin-6-yl]prop-2-enamide
- 2-Fluoro-N-[1-[2-[[[2-[[[(3R,4R)-3-hydroxy-4-piperidinyl]methyl]amino]-8-(1-methylethyl)pyrazolo[1,5-a]-1,3,5-triazin-4-yl]amino]methyl]phenyl]-6-isoquinolinyl]-2-propenamide
- 2-fluoro-N-[1-[2-[[[2-[[(3R,4R)-3-hydroxypiperidin-4-yl]methylamino]-8-propan-2-ylpyrazolo[1,5-a][1,3,5]triazin-4-yl]amino]methyl]phenyl]isoquinolin-6-yl]prop-2-enamide

cyclin-dependent kinase (CDK) inhibitor, antineoplastic, Q 901, CDK7-IN-21,
- OriginatorThe Lead Discovery Center; The Max Planck Institute of Biochemistry
- DeveloperQurient Co
- ClassAntineoplastics; Small molecules
- Mechanism of ActionCyclin-dependent kinase-activating kinase inhibitors
- Phase I/IISolid tumours
- 31 May 2024Preliminary efficacy, pharmacodynamics, pharmacokinetics and adverse events data from a phase I/II trial in Solid tumours presented at the 60th Annual Meeting of the American Society of Clinical Oncology (ASCO-2024)
- 21 May 2024Qurient Therapeutics enters into an Cooperative Research and Development Agreement (CRADA) with the US National Cancer Institute (NCI) for phase I/II trial in Small cell lung cancer (SCLC) and Solid tumours
- 21 May 2024Qurient Therapeutics plans phase I/II trial in Small cell lung cancer (SCLC) and Solid tumours
Mocaciclib (Q-901) is an orally bioavailable, selective cyclin-dependent kinase (CDK) inhibitor with potent activity against CDK2, CDK4, and CDK6. Preclinical data show that Mocaciclib inhibits CDK2/cyclin E with an IC₅₀ of 1.1 nM, CDK4/cyclin D1 with an IC₅₀ of 2.5 nM, and CDK6/cyclin D3 with an IC₅₀ of 4.1 nM, demonstrating high potency in enzymatic assays. In cancer cell lines, Mocaciclib suppresses retinoblastoma protein (Rb) phosphorylation, leading to G1 cell cycle arrest and growth inhibition in Rb-positive tumor models. It has shown antiproliferative effects in various preclinical models, including breast and lung cancers.
Mocaciclib is a selective inhibitor of cyclin-dependent kinase 7 (CDK7), with potential antineoplastic activity. Upon administration, mocaciclib selectively targets, covalently binds to and inhibits the activity of CDK7, thereby inhibiting CDK7-mediated signaling. The inhibition of CDK7 prevents phosphorylation of the carboxy-terminal domain (CTD) of RNA polymerase II, thereby preventing transcription of important cancer-promoting genes. It prevents phosphorylation of the cell cycle kinases CDK1, 2, 4, and 6, thereby disrupting uncontrolled cell cycle progression. Altogether, this may induce apoptosis, cause cell cycle arrest, inhibit DNA damage repair and inhibit tumor cell proliferation in certain cancers that are dependent on CDK7-mediated transcriptional regulation and signaling. CDK7, a serine/threonine kinase, plays a role in controlling cell cycle progression and transcriptional regulation, and promotes the expression of key oncogenes through the phosphorylation of RNA polymerase II. It is overexpressed in multiple cancers.
SYN
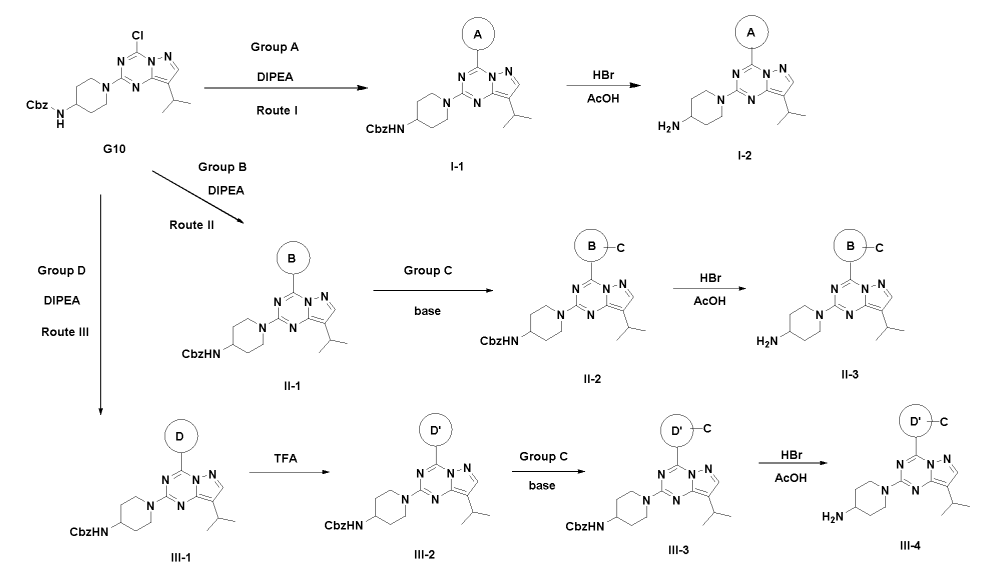
SYN
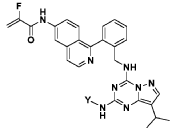
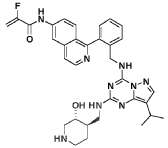
This is compound 64, as disclosed in WO2O19/197546.
PAT
- Compounds having cyclin-dependent kinase(cdk)-inhibitory functionPublication Number: WO-2022117504-A1Priority Date: 2020-12-02
- Substituted pyrazolo[1,5-a]pyrimidines and pyrazolo[1,5-a][1,3,5]triazines as CDK inhibitorsPublication Number: US-11858937-B2Priority Date: 2018-04-11Grant Date: 2024-01-02
- Pharmaceutically active pyrazolo-triazine and/or pyrazolo-pyrimidine derivativesPublication Number: US-2021139483-A1Priority Date: 2018-04-11
AS ON OCT2025 4.511 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
//////////mocaciclib, cyclin-dependent kinase (CDK) inhibitor, antineoplastic, Q 901, CDK7-IN-21,
Mobinitinib
Mobinitinib
CAS1402709-93-6
MF C22H23Cl2N7 MW456.37
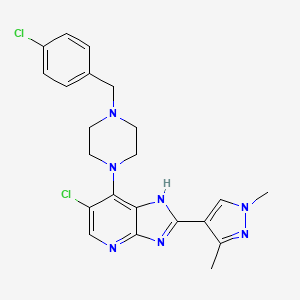
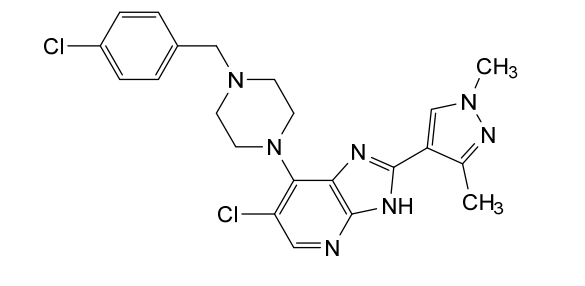
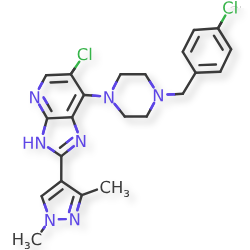
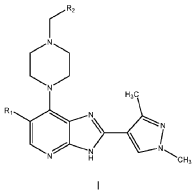
6-chloro-7-{4-[(4-chlorophenyl)methyl]piperazin-1-yl}-2-(1,3-dimethyl-1Hpyrazol-4-yl)-3H-imidazo[4,5-b]pyridine
6-chloro-7-{4-[(4-chlorophenyl)methyl]piperazin-1-yl}-2-(1,3-dimethyl-1Hpyrazol-4-yl)-3H-imidazo[4,5-b]pyridine
dual FMS-like tyrosine kinase-3 (FLT3)-Aurora kinase inhibitor, antineoplastic, CCT241736, CCT 241736, ZE94SP78UG, EP0042, EP 0042
Mobinitinib (CCT241736) is an investigational, orally bioavailable, small-molecule, dual inhibitor targeting Aurora kinase and FLT3 (including ITD and D835Y mutations). It shows potent antineoplastic activity in preclinical models, including acute myeloid leukemia (AML), by inhibiting tumor cell proliferation and disrupting mitotic spindle assembly. It is a distinct compound from similarly named drugs like Momelotinib or Binimetinib.
Key Details About Mobinitinib (CCT241736)
- Mechanism of Action: Acts as a dual inhibitor of Aurora kinases (A and B) and FMS-related tyrosine kinase 3 (FLT3). By inhibiting these kinases, it interferes with mitotic spindle assembly and chromosome segregation, leading to cell cycle arrest.
- Target Indications: Primarily studied for its potential to treat hematological malignancies and solid tumors that overexpress FLT3 or Aurora kinases. Preclinical studies show effectiveness in FLT3-ITD positive AML cell lines (e.g., MOLM-13, MV4-11).
- Preclinical Activity: Demonstrates strong anti-proliferative activity with
values in the sub-micromolar range (e.g., 0.1–0.3
M) in certain human tumor cell lines. It has shown significant tumor growth inhibition in mouse xenograft models at doses of 50-100 mg/kg.
- Chemical Properties: It is a 1H-imidazo[5-b]pyridine derivative.
It is important to distinguish mobinitinib (CCT241736) from momelotinib, a JAK1/JAK2 inhibitor approved for myelofibrosis, and binimetinib, a MEK inhibitor for melanoma.
Mobinitinib is an orally bioavailable inhibitor of both the serine/threonine protein kinase Aurora kinase and FMS-related tyrosine kinase 3 (FLT3; STK1; CD135; FLK2), with potential antineoplastic activity. Upon oral administration, mobinitinib specifically binds to and inhibits Aurora kinase and FLT3, which interferes with the activation of Aurora kinase- and FLT3-mediated signal transduction pathways. This may result in the disruption of the assembly of the mitotic spindle apparatus, the disruption of chromosome segregation and the inhibition of cell proliferation in tumor cells that overexpress Aurora kinase and/or FLT3. Aurora kinase plays essential roles in mitotic checkpoint control during mitosis. Aurora kinase and FLT3 are overexpressed in a variety of cancers and play key roles in tumor cell proliferation.
MOBINITINIB is a small molecule drug with a maximum clinical trial phase of II and has 1 investigational indication.
Study to Evaluate the Safety and Tolerability of EP0042
CTID: NCT04581512
Phase: Phase 1/Phase 2
Status: Recruiting
Date: 2025-10-14
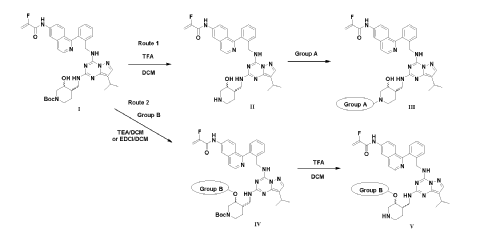
SYN
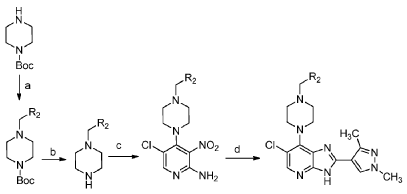
5-Chloro-4-(4-(4-chlorobenzyl)piperazin-1-yl)-3-nitropyridin-2-amine
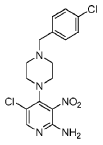
[00119] To a mixture of 2-amino-4,5-dichloro-3-nitropyridine (0.152 g, 0.73 mmol) and isopropanol (22 mL) was added 1 -(4-chlorobenzyl)piperazine (0.165 g, 0.78 mmol) followed by diisopropylethylamine (0.17 mL, 0.97 mmol). The reaction mixture was heated at 45 °C for 18 h, then allowed to cool to room temperature, and diluted with isopropanol (5 mL). The precipitate was collected by filtration, washed with isopropanol and diethyl ether. The title compound was thus obtained as a yellow solid (0.215 g, 77%); 1H-NMR (500 MHz, DMSO-d6) 2.48 (br s, obscured by DMSO peak, 4H, piperazine C-H), 3.06 (br t, J = 4.3 Hz, 4H, piperazine C-H), 3.52 (s, 2H, NCH2C6H4Cl), 6.95 (s, 2H, NH2), 7.35 (d, J = 8.5 Hz, 2H) and 7.38 (d, J = 8.5 Hz, 2H) (3,5-ArH and 2,6- ArH), 8.06 (s, 1 H, 6-H); LC – MS (ESI, m/z): Rt = 1 .70 min – 382, 384, 386 [(M+H)+, Cl2 isotopic pattern].
6-Chloro-7-(4-(4-chlorobenzyl)piperazin-1-yl)-2-(1,3-dimethyl-1H-pyrazol-4-yl)-3H-imidazo[4,5-b]pyridine
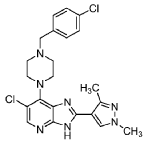
[00120] To a mixture of 5-chloro-4-(4-(4-chlorobenzyl)piperazin-1 -yl)-3-nitropyridin-2-amine (0.076 g, 0.20 mmol) and EtOH (4.0 ml.) was added 1 ,3-dimethyl-1 H-pyrazole-4-carbaldehyde (0.027 g, 0.22 mmol) followed by a freshly prepared aqueous solution of Na2S2O4 (1 M; 0.85 mL, 0.85 mmol). The reaction mixture was stirred at 80 °C for 24 h, it was then allowed to cool to room temperature, concentrated in vacuo, and the residue was absorbed on silica gel and placed on a 10 g isolute silica column. Elution with ethyl acetate / dichloromethane (v/v; 1 :1 ), and then 4% methanol in ethyl acetate / dichloromethane (v/v; 1 :1 ) afforded the title compound as a white solid after trituration with diethyl ether (0.023 g, 25%).
[00121 ] 1 H-NMR (500 MHz, DMSO-d6) 2.51 (s, obscured by solvent peak, pyrazole 3-CH3), 2.57 (br s, 4H, piperazine C-H), 3.54 (s, 2H, N-CH2C6H4Cl), 3.68 (br s, 4H, piperazine C-H), 3.84 (s, 3H, pyrazole N-Me), 7.37 (d, J = 8.5 Hz, 2H) and 7.40 (d, J = 8.5 Hz, 2H) (C6H4Cl), 8.02 (s, 1 H), and 8.18 (s, 1 H) (pyrazole 5-H, and imidazo[4,5-b]pyridine 5-H), 12.95 (br s, 1 H, imidazo[4,5-b]pyridine N-H); LC – MS (ESI, m/z): Rt = 1.97 min – 456, 458, 460 [(M+H)+, Cl2 isotopic pattern].
[00122] HRMS: Found: 456.1457, calculated for C22H24Cl2N7 (M+H)+: 456.1465.
LIT
- FLT3 Inhibitors in Acute Myeloid Leukemia: Challenges and Recent Developments in Overcoming ResistancePublication Name: Journal of Medicinal ChemistryPublication Date: 2021-03-10PMID: 33719439DOI: 10.1021/acs.jmedchem.0c01851
- Quizartinib-resistant FLT3-ITD acute myeloid leukemia cells are sensitive to the FLT3-Aurora kinase inhibitor CCT241736Publication Name: Blood AdvancesPublication Date: 2020-04-13PMCID: PMC7160287PMID: 32282883DOI: 10.1182/bloodadvances.2019000986
- Metabolism of the dual FLT-3/Aurora kinase inhibitor CCT241736 in preclinical and human in vitro models: Implication for the choice of toxicology speciesPublication Name: European journal of pharmaceutical sciences : official journal of the European Federation for Pharmaceutical SciencesPublication Date: 2019-11-01PMCID: PMC6892276PMID: 30953752DOI: 10.1016/j.ejps.2019.04.004
- Optimization of Imidazo[4,5-b]pyridine-Based Kinase Inhibitors: Identification of a Dual FLT3/Aurora Kinase Inhibitor as an Orally Bioavailable Preclinical Development Candidate for the Treatment of Acute Myeloid LeukemiaPublication Name: Journal of Medicinal ChemistryPublication Date: 2012-10-08PMCID: PMC3483018PMID: 23043539DOI: 10.1021/jm300952s
PAT
- Pharmaceutically active compoundsPublication Number: WO-2013190319-A1Priority Date: 2012-06-21
- Compound and, pharmaceutical compositionPublication Number: BR-112014032142-B1Priority Date: 2012-06-21
- Pharmaceutically active compoundsPublication Number: US-9447092-B2Priority Date: 2012-06-21Grant Date: 2016-09-20
- Pharmaceutically active compoundsPublication Number: CA-2876357-A1Priority Date: 2012-06-21
- Pharmaceutically active compoundsPublication Number: US-2015266868-A1Priority Date: 2012-06-21
- PHARMACEUTALLY ACTIVE COMPOUNDSPublication Number: RU-2015101702-APriority Date: 2012-06-21
- Pharmaceutically active compoundsPublication Number: SI-2864328-T1Priority Date: 2012-06-21
AS ON OCT2025 4.511 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
////////////////mobinitinib, antineoplastic, CCT241736, CCT 241736, ZE94SP78UG, EP0042, EP 0042
Mevrometostat
Mevrometostat
CAS 1844849-10-0
MF C22H24Cl2N2O5 MW467.3 g/mol
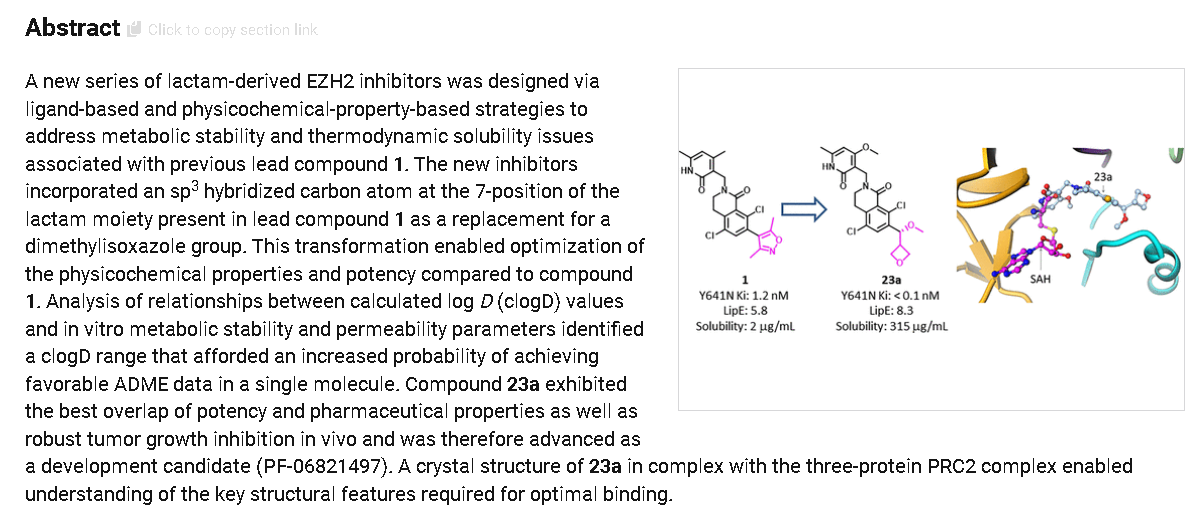
5,8-dichloro-2-[(4-methoxy-6-methyl-2-oxo-1H-pyridin-3-yl)methyl]-7-[(R)-methoxy(oxetan-3-yl)methyl]-3,4-dihydroisoquinolin-1-one
5,8-dichloro-7-[(R)-methoxy(oxetan-3-yl)methyl]-2-[(4-methoxy-6-methyl-2-oxo-1,2-dihydropyridin-3-yl)methyl]-3,4-
dihydroisoquinolin-1(2H)-one
enhancer of zeste homolog 2 (EZH2) inhibitor, antineoplastic, PF-06821497, PF 06821497, S4L4MM20B6
Mevrometostat (development code PF-06821497) is an investigational anticancer drug that functions as a potent and selective inhibitor of enhancer of zeste homolog 2 (EZH2).[1][2] Currently under development by Pfizer, mevrometostat is being investigated primarily for the treatment of metastatic castration-resistant prostate cancer (mCRPC) in combination with enzalutamide.
PF-06821497 is under investigation in clinical trial NCT03460977 (PF-06821497 Treatment Of Relapsed/Refractory SCLC, Castration Resistant Prostate Cancer, and Follicular Lymphoma).
Mevrometostat is an orally available selective inhibitor of the histone lysine methyltransferase (HMT) enhancer of zeste homolog 2 (EZH2), with potential antineoplastic activity. Upon oral administration, mevrometostat selectively targets, binds to and inhibits the activity of EZH2. Inhibition of EZH2 specifically prevents the methylation of histone H3 on lysine 27 (H3K27). This decrease in histone methylation alters gene expression patterns associated with cancer pathways and results in decreased proliferation of EZH2-expressing cancer cells. EZH2, an HMT class enzyme and the catalytic subunit of the polycomb repressive complex 2 (PRC2), is overexpressed or mutated in a variety of cancer cells and plays a key role in tumor cell proliferation; its expression is correlated with tumor initiation, progression, stem cell self-renewal, migration and angiogenesis.
MEVROMETOSTAT is a small molecule drug with a maximum clinical trial phase of II and has 1 investigational indication.
Synthesis
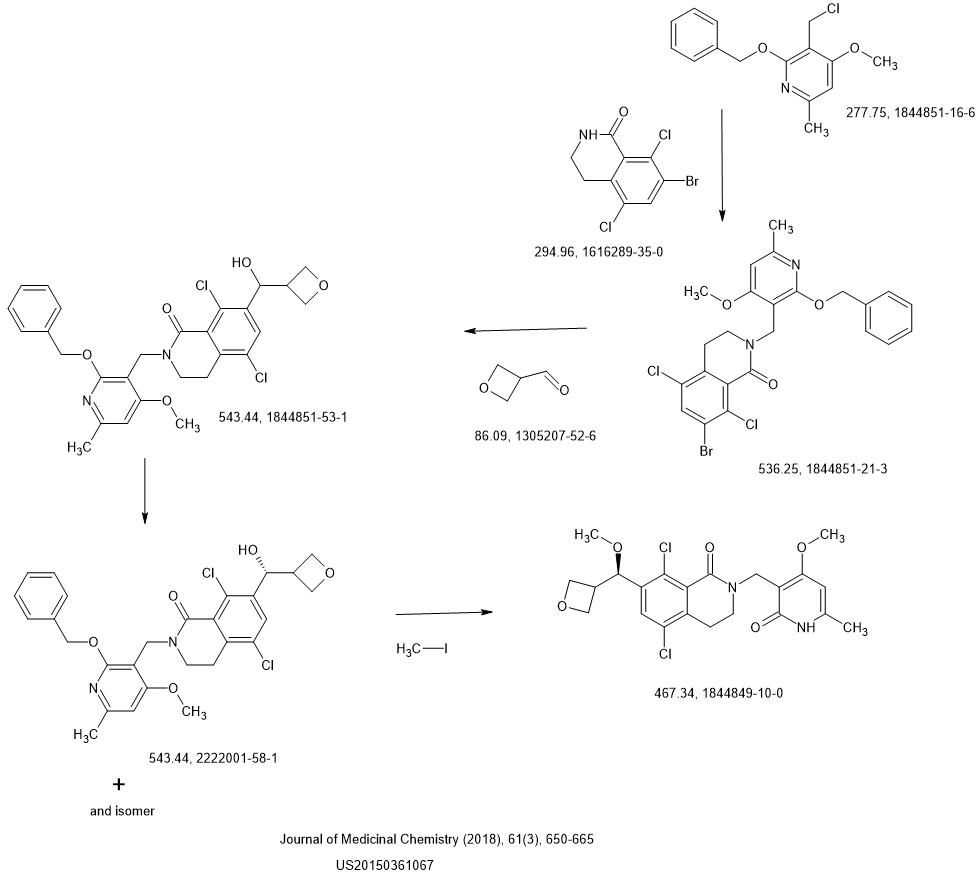
LAST STEP CONDITIONS
METHYL IODIDE REAGENT, Tetrahydrofuran , Potassium tert-butoxide
NEXT Hydrogen, Platinum dioxide,
SYN
Optimization of Orally Bioavailable Enhancer of Zeste Homolog 2 (EZH2) Inhibitors Using Ligand and Property-Based Design Strategies: Identification of Development Candidate (R)-5,8-Dichloro-7-(methoxy(oxetan-3-yl)methyl)-2-((4-methoxy-6-methyl-2-oxo-1,2-dihydropyridin-3-yl)methyl)-3,4-dihydroisoquinolin-1(2H)-one (PF-06821497)Publication Name: Journal of Medicinal ChemistryPublication Date: 2017-12-27PMID: 29211475DOI: 10.1021/acs.jmedchem.7b01375
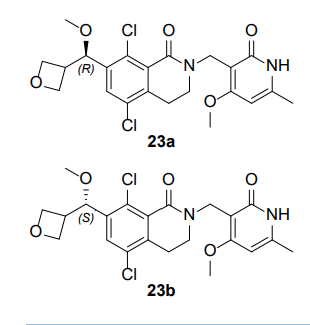
5,8-dichloro-2-[(4-methoxy-6-methyl-2-oxo-1,2-dihydropyridin-3-yl)methyl]-7-[(R)-
methoxy(oxetan-3-yl)methyl]-3,4-dihydroisoquinolin-1(2H)-one (23a) and 5,8-dichloro-2-[(4-
methoxy-6-methyl-2-oxo-1,2-dihydropyridin-3-yl)methyl]-7-[(S)-methoxy(oxetan-3-yl)methyl]-
3,4-dihydroisoquinolin-1(2H)-one (23b)
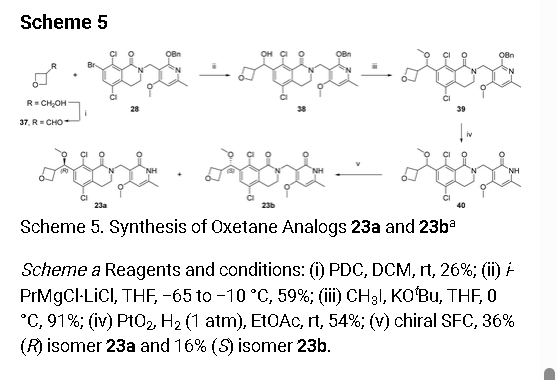
Multiple batches of (±)-5,8-dichloro-2-[(4-methoxy-6-
methyl-2-oxo-1,2-dihydropyridin-3-yl)methyl]-7-[methoxy-
(oxetan-3-yl)methyl]-3,4-dihydroisoquinolin-1(2H)-one 40
were combined (140 mg total), and the enantiomers separated
by preparative chiral SFC [Column: (R,R)Whelk O1
250mm*30mm,5µ; mobile phase: EtOH; wavelength: 220
nm] to give, after lyophilization, 23a (50.3 mg, 36%) as a
white solid, and 23b (22.8 mg, 16%) as a white solid. A
small-molecule X-Ray crystal structure of 23a showed it to
have absolute (R) stereochemistry. A small-molecule X-Ray crystal structure of 23b confirmed
the expected absolute (S) stereochemistry.
5,8-dichloro-2-[(4-methoxy-6-methyl-2-oxo-1,2-dihydropyridin-3-yl)methyl]-7-[(R)-
methoxy(oxetan-3-yl)methyl]-3,4-dihydroisoquinolin-1(2H)-one (23a). After chiral SFC and
lyophilization, 23a (50.3 mg, 36%) was obtained as a white solid. LCMS m/z 489 [M+Na]+; 1H
NMR (400 MHz, CDCl3) δ 12.34 (br s, 1H), 7.49 (s, 1H), 5.93 (s, 1H), 5.05 (d, J=6.0 Hz, 1H),
4.78-4.61 (m, 6H), 3.88 (s, 3H), 3.50-3.48 (m, 2H), 3.38-3.37 (m, 1H), 3.31 (s, 3H), 2.94 (t,
J=6.2 Hz, 2H), 2.35 (s, 3H). [α]D
22 +67.7° (c 0.1, MeOH); Chiral analysis: 100% ee; retention
time 9.85 min; column (R,R)Whelk O1, 250×4.6mm I.D., 5µ; mobile phase 50% ethanol (0.05%
DEA) in CO2; wavelength 220 nm. A crystalline sample of 23a was obtained by dissolving the
lyophilized powder in hot isopropanol in a 1 dram vial, then letting the vial stand in a capped
TLC chamber containing a layer of hexanes in the bottom, which allowed slow diffusion of hexanes into isopropanol. After two days, crystals (square plates) were collected. A smallmolecule X-Ray crystal structure of 23a showed it to have absolute (R) stereochemistry.
Crystallographic data are available in the Supporting Information.
syn
Pfizer Inc.
United States, US20150361067
REF
- Computational exploration in search for novel natural product-derived EZH2 inhibitors for advancing anti-cancer therapyPublication Name: Molecular DiversityPublication Date: 2025-02-19PMID: 39969739DOI: 10.1007/s11030-025-11128-3
- TTD: Therapeutic Target Database describing target druggability informationPublication Name: Nucleic Acids ResearchPublication Date: 2023-09-15PMCID: PMC10767903PMID: 37713619DOI: 10.1093/nar/gkad751
- BLM overexpression as a predictive biomarker for CHK1 inhibitor response in PARP inhibitor–resistant BRCA -mutant ovarian cancerPublication Name: Science Translational MedicinePublication Date: 2023-06-21PMCID: PMC10758289PMID: 37343085DOI: 10.1126/scitranslmed.add7872
- Structural modification aimed for improving solubility of lead compounds in early phase drug discoveryPublication Name: Bioorganic & Medicinal ChemistryPublication Date: 2022-02-15PMID: 35033884DOI: 10.1016/j.bmc.2022.116614
- High-Throughput Screening to Identify Inhibitors of the Type I Interferon–Major Histocompatibility Complex Class I Pathway in Skeletal MusclePublication Name: ACS Chemical BiologyPublication Date: 2020-05-27PMCID: PMC7859889PMID: 32459468DOI: 10.1021/acschembio.0c00343
- Translational Pharmacokinetic-Pharmacodynamic Modeling for an Orally Available Novel Inhibitor of Epigenetic Regulator Enhancer of Zeste Homolog 2Publication Name: The Journal of Pharmacology and Experimental TherapeuticsPublication Date: 2020-05PMID: 32094296DOI: 10.1124/jpet.119.263491
- Optimization of Orally Bioavailable Enhancer of Zeste Homolog 2 (EZH2) Inhibitors Using Ligand and Property-Based Design Strategies: Identification of Development Candidate (R)-5,8-Dichloro-7-(methoxy(oxetan-3-yl)methyl)-2-((4-methoxy-6-methyl-2-oxo-1,2-dihydropyridin-3-yl)methyl)-3,4-dihydroisoquinolin-1(2H)-one (PF-06821497)Publication Name: Journal of Medicinal ChemistryPublication Date: 2017-12-27PMID: 29211475DOI: 10.1021/acs.jmedchem.7b01375
- Somatic mutations at EZH2 Y641 act dominantly through a mechanism of selectively altered PRC2 catalytic activity, to increase H3K27 trimethylationPublication Name: BloodPublication Date: 2011-02-24PMCID: PMC3062411PMID: 21190999DOI: 10.1182/blood-2010-11-321208
PAT
- Novel 3-amino-3,4,6-trideoxyglycals, their production methods and anthracyclines obtained from these glycalsPublication Number: JP-S6110572-APriority Date: 1984-06-15
- CARBON HYDROGENATION METHOD WITH INCREASED RETENTION OF SOLIDS IN FLUID BED REACTORSPublication Number: DE-3245494-A1Priority Date: 1981-12-21
- Group extraction of organic compounds present in liquid samplesPublication Number: US-3966410-APriority Date: 1972-07-24Grant Date: 1976-06-29
- PRMT5 inhibitors and uses thereofPublication Number: US-12448388-B2Grant Date: 2025-10-21
- KRAS G12D modulating compoundsPublication Number: US-12448400-B2Grant Date: 2025-10-21
- Fungicidal, acaricidal and insecticidal composition comprising imidazole derivatives as active ingredient and process for producing the active ingredientsPublication Number: HU-206245-BPriority Date: 1987-03-13
- Fluorine derivatives of vitamin d _and process for producing the samePublication Number: CA-1297869-CPriority Date: 1986-10-20Grant Date: 1992-03-24
- Fluorine derivatives of vitamin d3 and process for producing the samePublication Number: EP-0264880-B1Priority Date: 1986-10-20Grant Date: 1991-03-13
- Fluorine derivatives of vitamin D3 and process for producing the samePublication Number: EP-0264880-A1Priority Date: 1986-10-20
- Process for production of new derivatives of imidasolil-alkyl-guanidin and medical preparatives containing these substancesPublication Number: HU-198024-BPriority Date: 1985-04-02
WO-0003990-A1 WO-0059513-A1 WO-0127114-A1 WO-02100354-A2 WO-2004029040-A1 WO-2004033420-A1 WO-2004078712-A2 WO-2004092118-A2 WO-2005000869-A1 WO-2005040109-A1 WO-2005082368-A1 WO-2006083424-A2 WO-2007022638-A1 WO-2007030089-A1 WO-2007058503-A1 WO-2008116833-A1 WO-2009005690-A2 WO-2009142969-A1 WO-2010015656-A2 WO-2010123599-A9 WO-2011102800-A1 WO-2011115818-A1 WO-2011139702-A2 WO-2012033149-A1 WO-2012037372-A2 WO-2012069856-A1 WO-2012097013-A1 WO-2012112969-A1 WO-2012129673-A1 WO-2012130912-A1 WO-2013096679-A1 WO-2013096680-A1 WO-2013102242-A1 WO-2013142525-A1 WO-2013177983-A1 WO-2014037498-A2 WO-2014057415-A2 WO-2015193765-A1 WO-2020190754-A1 WO-2021163064-A9 WO-2022053990-A1 WO-2022058405-A2 WO-2022087149-A2 WO-2022087230-A1 WO-2022164789-A1 WO-2022164789-A9 WO-2022212746-A1 WO-2022212748-A1 WO-2022221304-A1 WO-2022232435-A1 WO-2022261243-A1 WO-2022271650-A1 WO-2022271659-A1 WO-2022271677-A1 WO-2022271684-A1 WO-2023015164-A1 WO-2023041674-A1 WO-2023055885-A2 WO-2023061446-A1 WO-2023076554-A9 WO-2023076983-A1 WO-2023077030-A1 WO-2023100131-A1 WO-2023108563-A1 WO-2023111810-A1 WO-2023114460-A1 WO-2023122581-A2 WO-2023122615-A1 WO-2023147418-A1 WO-2023166418-A2 WO-2023166420-A1 WO-2023178181-A1 WO-2023178354-A1 WO-2023183817-A1 WO-2023196784-A1 WO-2023205719-A1 WO-2023205850-A1 WO-2023212504-A1 WO-2023218320-A1 WO-2023242769-A1 WO-2023249714-A1 WO-2024003773-A1 WO-2024006929-A1 WO-2024009191-A1 WO-2024015566-A1 WO-2024019995-A1 WO-2024020534-A2 WO-2024033513-A1 WO-2024035688-A1 WO-2024064668-A1 WO-2024074977-A1 WO-2024086094-A1 WO-2024105563-A1 WO-2024187153-A1 WO-2024189607-A1 WO-2024192373-A1 WO-2024193570-A1 WO-2024193570-A9 WO-2024209339-A1 WO-2024213979-A1 WO-2024215754-A1 WO-2024218686-A1 WO-2024220917-A1 WO-2024246965-A1 WO-2025006704-A1 WO-2025006720-A1 WO-2025024663-A1 WO-2025024811-A1 WO-2025031307-A1 WO-2025038726-A2 WO-2025049966-A2 WO-2025049966-A9 WO-2025054347-A1 WO-2025054530-A1 WO-2025059027-A1 WO-2025085536-A1 WO-2025094035-A1 WO-2025096589-A1 WO-2025121805-A1 WO-2025121807-A1 WO-2025137640-A1 WO-2025151706-A1 WO-2025245003-A1 WO-9012007-A1 WO-9522521-A1 WO-9954305-A1
AS ON OCT2025 4.511 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
Mechanism of action
Mevrometostat is a small molecule inhibitor that targets EZH2, the catalytic subunit of polycomb repressive complex 2 (PRC2).[1][3] EZH2 plays a crucial role in epigenetic regulation by modifying gene expression patterns that control cellular fate decisions, including differentiation and self-renewal.[1]
In prostate cancer, EZH2 dysregulation contributes to treatment resistance through multiple pathways, including:
- Silencing of tumor suppressor genes
- Activation of androgen receptor transcription factors
- Promotion of neuroendocrine transdifferentiation[4]
Mevrometostat demonstrates dose-dependent EZH2 inhibition, leading to reactivation of tumor suppressor genes while suppressing genes involved in tumor progression.[5]
Clinical development
Phase I/II trials
The primary clinical evaluation of mevrometostat is being conducted through a phase 1/2 dose-expansion study (NCT03460977) investigating the combination of mevrometostat with enzalutamide and androgen deprivation therapy in patients with mCRPC.[6]
The dose-expansion portion of this study enrolled patients with mCRPC who had previously received abiraterone, with evidence of disease progression per modified Prostate Cancer Working Group 3 criteria.[2]
Key efficacy results
In the randomized dose-expansion study, the combination of mevrometostat (1,250 mg twice daily on an empty stomach) plus enzalutamide demonstrated:
- 49% relative reduction in the rate of progression or death
- Approximately 8-month improvement in median radiographic progression-free survival (rPFS)
- Hazard ratio of 0.51 (90% CI: 0.28–0.95)[7]
The median radiographic progression-free survival was 14.3 months with the combination therapy compared to 6.2 months with enzalutamide alone.[8]
Phase III trials
Based on promising phase I/II results, Pfizer has initiated multiple phase 3 clinical trials:
MEVPRO-1 study
The MEVPRO-1 study (NCT06551324) is a randomized phase 3 trial evaluating mevrometostat in combination with enzalutamide versus physician’s choice of therapy in patients with mCRPC previously treated with abiraterone acetate.[9][10]
- Study design: Randomized 1:1 to receive mevrometostat (875 mg twice daily with food) plus enzalutamide (160 mg daily) versus physician’s choice of enzalutamide or docetaxel
- Target enrollment: Approximately 600 patients
- Primary endpoint: Blinded independent central review-assessed rPFS per RECIST 1.1 and PCWG3 criteria
- Key secondary endpoint: Overall survival
MEVPRO-2 study
The MEVPRO-2 study (NCT06629779) is evaluating mevrometostat plus enzalutamide in androgen receptor pathway inhibitor (ARPI)-naïve patients with mCRPC.[11][12]
Additional development
Pfizer has also initiated phase 3 trials evaluating mevrometostat plus enzalutamide in first-line metastatic castration-sensitive prostate cancer.[8][13]
Safety profile
The most common adverse events considered related to mevrometostat treatment include:
Dose optimization studies found that mevrometostat 875 mg twice daily with food showed similar efficacy and better safety compared to the 1,250 mg dose on an empty stomach.[15]
Pharmacokinetics
Based on safety and pharmacokinetic findings from phase 1 trials, mevrometostat 875 mg twice daily with food was selected as the recommended dose for phase 3 clinical development in combination with enzalutamide.[16]
Regulatory status
As of 2025, mevrometostat remains an investigational agent under clinical development by Pfizer. The drug has not received regulatory approval from the Food and Drug Administration (FDA), European Medicines Agency (EMA), or other regulatory authorities.
See also
- Polycomb repressive complex 2
- Tazemetostat (approved EZH2 inhibitor)
- Prostate cancer
- Enzalutamide
References
- “Mevrometostat (PF-06821497)”. Pfizer Oncology Development. Retrieved 11 September 2025.
- Schweizer MT, Calvo M, Moreno V, Mellado B, Castellano D, Spira AI, et al. (2025). “Mevrometostat (PF-06821497), an enhancer of zeste homolog 2 (EZH2) inhibitor, in combination with enzalutamide in patients with metastatic castration-resistant prostate cancer (mCRPC): A randomized dose-expansion study”. Journal of Clinical Oncology. 43 (5_suppl) LBA138. doi:10.1200/JCO.2025.43.5_suppl.LBA138.
- Schweizer MT, Penkov K, Choudhury AD, Calvo E, Frank RC, Liu L, et al. (2024). “Phase 1 trial of mevrometostat (PF-06821497), a potent and selective inhibitor of enhancer of zeste homolog 2 (EZH2), in castration-resistant prostate cancer (CRPC)”. Journal of Clinical Oncology. 42 (16_suppl): 5061. doi:10.1200/JCO.2024.42.16_suppl.5061.
- “SUO 2024: Mevrometostat (PF-06821497) in Combination with Enzalutamide in Patients with Metastatic Castration-Resistant Prostate Cancer Previously Treated with Abiraterone Acetate”. UroToday. Retrieved 11 September 2025.
- “Mevrometostat and enzalutamide in mCRPC: gene expression and EZH2 modulation”. VJ Oncology. 17 February 2025. Retrieved 11 September 2025.
- Pfizer (4 September 2025). A PHASE I DOSE ESCALATION AND EXPANDED COHORT STUDY OF PF 06821497 (MEVROMETOSTAT) IN THE TREATMENT OF ADULT PATIENTS WITH RELAPSED/REFRACTORY SMALL CELL LUNG CANCER (SCLC), CASTRATION RESISTANT PROSTATE CANCER (CRPC) AND FOLLICULAR LYMPHOMA (FL) (Report). clinicaltrials.gov.
- “ASCO GU 2025: Mevrometostat (PF-06821497), an EZH2 Inhibitor, in Combination with Enzalutamide in Patients with mCRPC”. UroToday. Retrieved 11 September 2025.
- “Mevrometostat/enzalutamide combo shows rPFS benefit in mCRPC”. Urology Times. 21 February 2025. Retrieved 11 September 2025.
- Agarwal N, Schweizer MT, Castro E, Azad A, George DJ, Chakrabarti J, et al. (2025). “Mevrometostat (PF-06821497) in combination with enzalutamide in patients with metastatic castration-resistant prostate cancer previously treated with abiraterone acetate: The phase 3, randomized MEVPRO-1 study”. Journal of Clinical Oncology. 43 (5_suppl) TPS288. doi:10.1200/JCO.2025.43.5_suppl.TPS288.
- Pfizer (4 September 2025). A PHASE 3, RANDOMIZED, OPEN-LABEL STUDY OF PF-06821497 (MEVROMETOSTAT) IN COMBINATION WITH ENZALUTAMIDE COMPARED WITH ENZALUTAMIDE OR DOCETAXEL IN PARTICIPANTS WITH METASTATIC CASTRATION RESISTANT PROSTATE CANCER PREVIOUSLY TREATED WITH ABIRATERONE ACETATE (MEVPRO-1) (Report). clinicaltrials.gov.
- “ASCO GU 2025: Mevrometostat (PF-06821497) in Combination With Enzalutamide for ARPI-Naïve Patients With mCRPC: The Phase 3, Randomized MEVPRO-2 Trial”. UroToday. Retrieved 11 September 2025.
- Pfizer (4 September 2025). A PHASE 3, RANDOMIZED, DOUBLE BLIND, PLACEBO CONTROLLED STUDY OF PF-06821497 (MEVROMETOSTAT) WITH ENZALUTAMIDE IN METASTATIC CASTRATION RESISTANT PROSTATE CANCER (MEVPRO-2) (Report). clinicaltrials.gov.
- Pfizer (4 September 2025). A Phase 3, Randomized, Double-Blind, Placebo-Controlled Study of Mevrometostat (PF-06821497) With Enzalutamide in Metastatic Castration-Sensitive Prostate Cancer (MEVPRO-3) (Report). clinicaltrials.gov.
- “ASCO 2025: Mevrometostat in Combination with Enzalutamide in Patients with mCRPC Previously Treated with Abiraterone Acetate”. UroToday. Retrieved 11 September 2025.
- “Mevrometostat Plus Enzalutamide Improves rPFS vs Enzalutamide in Metastatic CRPC”. OncLive. 21 February 2025. Retrieved 11 September 2025.
- “ASCO 2025: Safety and Pharmacokinetics of Mevrometostat in Combination with Enzalutamide in Patients with mCRPC”. UroToday. Retrieved 11 September 2025.
| Clinical data | |
|---|---|
| Other names | PF-06821497 |
| Identifiers | |
| IUPAC name | |
| CAS Number | 1844849-10-0 |
| PubChem CID | 118572065 |
| IUPHAR/BPS | 10516 |
| DrugBank | DB14799 |
| ChemSpider | 65321668 |
| UNII | S4L4MM20B6 |
| KEGG | D12845 |
| ChEMBL | ChEMBL4080228 |
| PDB ligand | CJD (PDBe, RCSB PDB) |
| Chemical and physical data | |
| Formula | C22H24Cl2N2O5 |
| Molar mass | 467.34 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| SMILES | |
| InChI | |
/////////mevrometostat, enhancer of zeste homolog 2 (EZH2) inhibitor, antineoplastic, PF-06821497, PF 06821497, S4L4MM20B6
#mevrometostat, #enhancer of zeste homolog 2 (EZH2) inhibitor, #antineoplastic, #PF-06821497, #PF 06821497, #S4L4MM20B6
Maritupirdine
Maritupirdine
CAS 1025725-91-0
MF C21H24N2 MW304.4 g/mol
2,3,4,5-TETRAHYDRO-2,8-DIMETHYL-5-PHENETHYL-1H-PYRIDO(4,3-B)INDOLE
2,8-dimethyl-5-(2-phenylethyl)-2,3,4,5-tetrahydro-1H-pyrido[4,3-b]indole
serotonin receptor antagonist, antidepressant, AVN-101, AVN 101, CD 008 0045, 6MHR5IV28S
- OriginatorChemDiv
- DeveloperAllaChem; Avineuro Pharmaceuticals; ChemDiv
- ClassAntidementias; Indoles; Neuroprotectants; Pyridines; Small molecules
- Mechanism of ActionAdrenergic receptor antagonists; Dopamine receptor antagonists; Histamine receptor antagonists; Serotonin 6 receptor antagonists
- Phase IIAlzheimer’s disease; Anxiety disorders
- 27 Sep 2022No development reported – Phase-II for Anxiety disorders in Russia (PO)
- 22 Dec 2020Chemical structure information added
- 22 Oct 2020Avineuro Pharmaceuticals and Avineuro Pharmaceuticals plans a phase III trial in Anxiety disorders in December 2020 (PO, Capsules) (NCT04598867)
MARITUPIRDINE is a small molecule drug with a maximum clinical trial phase of II and has 1 investigational indication.
Maritupirdine (developmental code name AVN-101), a close structural analogue of latrepirdine, is a selective 5-HT6 receptor antagonist which is under development by Avineuro Pharmaceuticals for the treatment of Alzheimer’s disease and anxiety disorders.[1][2][3] As of November 2013, it was in phase II clinical trials for these indications.[2][3][4][needs update]
It was approved in Russia on May 31, 2023 under the brand name Aviandr for the treatment of generalized anxiety disorder, mild-to-moderate anxiety conditions (stress reactions and adjustment disorders) and anxiety after COVID-19.[5]
SYN
PAT
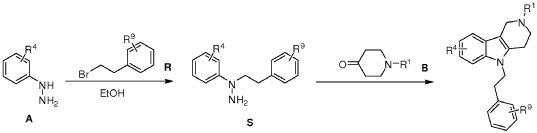
REF
- Alzheimer’s disease: Updated multi-targets therapeutics are in clinical and in progressPublication Name: European Journal of Medicinal ChemistryPublication Date: 2022-08-05PMID: 35635955DOI: 10.1016/j.ejmech.2022.114464
- Structure–Activity Relationships and Therapeutic Potentials of 5-HT7Receptor Ligands: An UpdatePublication Name: Journal of Medicinal ChemistryPublication Date: 2018-05-16PMID: 29767995DOI: 10.1021/acs.jmedchem.7b01898
- Serotonin 5-HT6Receptor Antagonists for the Treatment of Cognitive Deficiency in Alzheimer’s DiseasePublication Name: Journal of Medicinal ChemistryPublication Date: 2014-06-03PMID: 24850589DOI: 10.1021/jm5003952
- Synthesis and biological activity of 5-styryl and 5-phenethyl-substituted 2,3,4,5-tetrahydro-1H-pyrido[4,3-b]indolesPublication Name: Bioorganic & Medicinal Chemistry LettersPublication Date: 2010-01-01PMID: 19945877DOI: 10.1016/j.bmcl.2009.11.037
PAT
- Ligands of 5-ht6 receptors, a pharmaceutical composition, method for the production and use thereofPublication Number: EP-2184064-A2Priority Date: 2006-11-16
- Ligands of 5-ht6 receptors, a pharmaceutical composition, method for the production and use thereofPublication Number: US-2011046368-A1Priority Date: 2006-11-16
- Substituted 2,3,4,5-tetrahydro-1h-pyrido[4,3-b]indoles, methods for the production and use thereofPublication Number: AU-2008236872-A1Priority Date: 2007-04-05
- Substituted 2,3,4,5-tetrahydro-1h-pyrido[4,3-b]indoles, methods for the production and use thereofPublication Number: WO-2008123796-A2Priority Date: 2007-04-05
- Substituted 2,3,4,5-Tetrahyrdo-1H-Pyrido[4,3-B]Indoles, Methods for the Production and Use ThereofPublication Number: US-2010120792-A1Priority Date: 2007-04-05
- Sustituted 2,3,4,5-tetrahydro-1h-pyrido[4,3-b]indoles, methods for use thereofPublication Number: US-2013217703-A1Priority Date: 2007-04-05
- Ligands of 5-ht6 receptors, a pharmaceutical composition, method for the production and use thereofPublication Number: WO-2008060190-A2Priority Date: 2006-11-16
AS ON OCT2025 4.511 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
References
- Ivachtchenko V, Ivanenkov Y (2013). “Small Molecule 5-HT6R Ligands: A Comprehensive Insight into their Selectivity and Activity”. Current Bioactive Compounds. 9 (1): 64–100. doi:10.2174/1573407211309010007. ISSN 1573-4072.
- Griebel G, Holmes A (September 2013). “50 years of hurdles and hope in anxiolytic drug discovery”. Nature Reviews. Drug Discovery. 12 (9): 667–87. doi:10.1038/nrd4075. PMC 4176700. PMID 23989795.
- Benhamú B, Martín-Fontecha M, Vázquez-Villa H, Pardo L, López-Rodríguez ML (September 2014). “Serotonin 5-HT6 receptor antagonists for the treatment of cognitive deficiency in Alzheimer’s disease”. Journal of Medicinal Chemistry. 57 (17): 7160–81. doi:10.1021/jm5003952. PMID 24850589.
- “AVN 101”. AdisInsight. Retrieved 2015-06-10.
- “Aviandr (2,8-dimethyl-5-(2-phenylethyl)-2,3,4,5-tetrahydro-1H-pyrido[4,3-b]indole hydrochloride) film-coated tablets. Full prescribing information”. Russian State Register of Medicines (in Russian). Avineuro Pharmaceuticals, Inc.
External links
| Identifiers | |
|---|---|
| IUPAC name | |
| CAS Number | 1025725-91-0 1061354-48-0 (hydrochloride) |
| ChemSpider | 24643855 |
| UNII | 6MHR5IV28S |
| ChEMBL | ChEMBL592752 |
| CompTox Dashboard (EPA) | DTXSID901032403 |
| Chemical and physical data | |
| Formula | C21H24N2 |
| Molar mass | 304.437 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| SMILES | |
| InChI | |
////////////maritupirdine, serotonin receptor antagonist, antidepressant, AVN-101, AVN 101, CD 008 0045, 6MHR5IV28S
Luvometinib
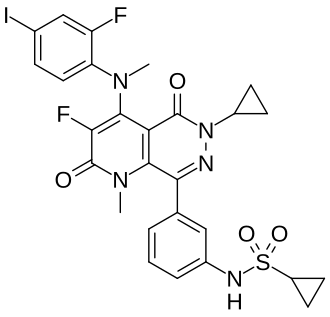
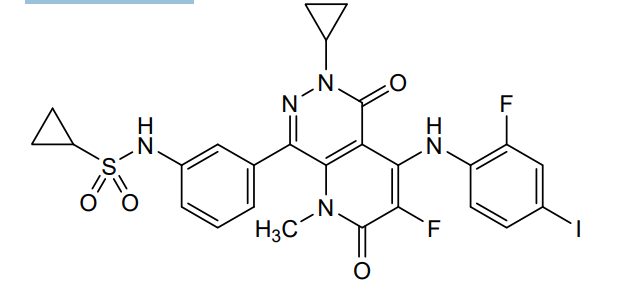
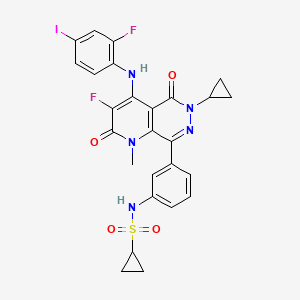
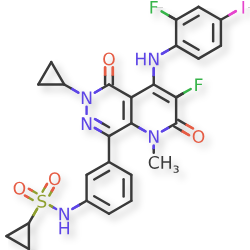
Luvometinib
CAS 2739690-43-6
MF C26H22F2IN5O4S MW665.5 g/mol
CHINA 2025, APPROVALS 2025
N-[3-[6-cyclopropyl-3-fluoro-4-(2-fluoro-4-iodoanilino)-1-methyl-2,5-dioxopyrido[2,3-d]pyridazin-8-yl]phenyl]cyclopropanesulfonamide
N-{3-[6-cyclopropyl-3-fluoro-4-(2-fluoro-4-iodoanilino)-1-methyl-2,5-dioxo-1,2,5,6-tetrahydropyrido[2,3-
d]pyridazin-8-yl]phenyl}cyclopropanesulfonamide
mitogen-activated protein kinase (MEK) inhibitor, antineoplastic, FCN 159, FCN-159, B2DYT4V89X
Luvometinib is a drug for the treatment of various types of cancer. It is a selective, orally administered inhibitor of mitogen-activated protein kinase kinases 1 and 2 (MEK1/MEK2), developed by Fosun Pharma for the treatment of rare malignancies, especially those driven by abnormal abnormal mitogen-activated protein kinase (MAPK) activation.[1][2]
In May 2025, it was approved in China for the treatment of histiocytic neoplasms such as Langerhans cell histiocytosis (LCH) and the genetic disease neurofibromatosis type 1 (NF1).[2]
Luvometinib is an orally bioavailable inhibitor of mitogen-activated protein kinase kinase (MAP2K, MAPK/ERK kinase, or MEK) 1 and 2, with potential antineoplastic activity. Upon administration, luvometinib selectively binds to and inhibits the activity of MEK1 and MEK2, preventing the activation of MEK1/2-dependent effector proteins and transcription factors, which may result in the inhibition of growth factor-mediated cell signaling and tumor cell proliferation. MEK1/2 are dual-specificity threonine/tyrosine kinases that play key roles in the activation of the RAS/RAF/MEK/ERK pathway that regulates cell growth. This pathway is often dysregulated in a variety of tumor cell types through BRAF, KRAS and NRAS mutations.
Luvometinib is a small molecule drug. The usage of the INN stem ‘-tinib’ in the name indicates that Luvometinib is a tyrosine kinase inhibitor. Luvometinib is under investigation in clinical trial NCT07004075 (FCN-159 Monotherapy Versus Chemotherapy by Investigator’s Choice in Pediatric Low-grade Glioma Patients With BRAF Alteration). Luvometinib has a monoisotopic molecular weight of 665.04 Da.
SYN
Example 8
N-(3-(6-allyl-3-ƒluoro-4-(2-ƒluoro-4-iodophenylamino)-1-methyl-2,5-dioxo-1,2,5,6- tetrahydropyrido[2,3-d]pyridazin-8-yl)phenyl)cyclopropanesulƒonamide (8)
The title compound 8 was prepared following the same procedure as described for Example 5 by substituting methanesulfonyl chloride with cyclopropanesulfonyl chloride. MS-ESI (m/z): 666 [M + 1]+.
PAT
Example 8
N-(3-(6-cyclopropyl-3-fluoro-4-(2-fluoro-4-iodophenylamino)-1-methyl-2,5-dioxo-1,2,5,6-tetrahydropyrido[2,3-d]pyridazin-8-yl)phenyl)cyclopropanesulfonamide (8)
[0136] The title compound 8 was prepared following the same procedure as described for Example 5 by substituting methanesulfonyl chloride with cyclopropanesulfonyl chloride. MS-ESI (m/z): 666 [M + 1] +.
PAT
- Protein kinase inhibitorsPublication Number: CN-106905316-BPriority Date: 2013-04-18Grant Date: 2021-06-01
- Certain protein kinase inhibitorsPublication Number: EP-2986611-B1Priority Date: 2013-04-18Grant Date: 2019-02-06
- Certain protein kinase inhibitorsPublication Number: US-10022374-B2Priority Date: 2013-04-18Grant Date: 2018-07-17
AS ON OCT2025 4.511 LAKHS VIEWS ON BLOG WORLDREACH AVAILABLEFOR YOUR ADVERTISEMENT
join me on Linkedin
Anthony Melvin Crasto Ph.D – India | LinkedIn
join me on Researchgate
RESEARCHGATE
join me on Facebook
Anthony Melvin Crasto Dr. | Facebook
join me on twitter
Anthony Melvin Crasto Dr. | twitter
+919321316780 call whatsaapp
EMAIL. amcrasto@gmail.com
References
- Cheng Y, Tian H (2017). “Current Development Status of MEK Inhibitors”. Molecules. 22 (10). Basel, Switzerland: 1551. doi:10.3390/molecules22101551. PMC 6151813. PMID 28954413.
- Keam SJ (2025). “Luvometinib: First Approval”. Drugs. 85 (9): 1177–1183. doi:10.1007/s40265-025-02217-6. PMID 40751881.
| Clinical data | |
|---|---|
| Trade names | 复迈宁 (Fu Mainin) |
| Other names | FCN-159 |
| Routes of administration | Oral |
| Identifiers | |
| IUPAC name | |
| CAS Number | 2739690-43-6 |
| PubChem CID | 135210935 |
| IUPHAR/BPS | 13495 |
| UNII | B2DYT4V89X |
| Chemical and physical data | |
| Formula | C26H22F2IN5O4S |
| Molar mass | 665.45 g·mol−1 |
| 3D model (JSmol) | Interactive image |
| SMILES | |
| InChI | |
//////////luvometinib, CHINA 2025, APPROVALS 2025, antineoplastic, FCN 159, FCN-159, B2DYT4V89X, ANAX, PTFEON, ADVECT, BLUE JET
ADVERTISEMENT
ANAX LABORATORIES
WEBSITE https://www.anaxlab.com/
Discovery Solutions, Supporting the chemistry needs of clients in the Medical, Analytical and Bio Sciences
Development Solutions, Developing from Lab scale to PR&D, Kilo Scale-ups and Commercial Scales
SEE MORE………Integrated Solutions, Manufacturing Solutions, Products,
Can’t Find? Let’s Connect

Phone : +91 897704 2010 / +91 9177075735, Email : info@anaxlab.com
ADVERTISEMENT
Advect Process Systems Ltd.
ADVECT PROCESS SYSTEMS CANADA LTD
51 Beechwood Rd., Cambridge, ON Canada N1S 3S1, Call Now +1 306 850 6737, Mail Now, ask@advectprocess.com
ADVERTISEMENT
BLUE JET HEALTHCARE LTD, https://bluejethealthcare.com
Looking for a Reliable SNAC Manufacturer? Let’s Talk.
At Blue Jet Healthcare Ltd, we specialize in the scalable, high-purity production of SNAC—a critical excipient powering the next generation of oral peptide therapeutics.
With increasing demand for SNAC across global pharma pipelines, choosing the right manufacturing partner is essential. Quality, timelines, and consistency matter.

Phone No. +91 (22) 22075307 / +91 (22) 22071691
Business Development/ Contract Manufacturing: marketing1@bluejethealthcare.com, madhu.gautam71@gmail.com
DR ANTHONY MELVIN CRASTO

ORGANIC SPECTROSCOPY


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}